CPRC: é possível estabelecer
qual o melhor
sequenciamento?
Luiz Flávio Coutinho
Tiradentes
13/08/2016
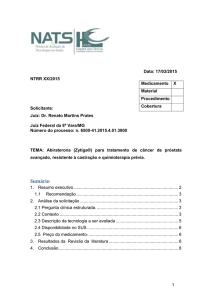
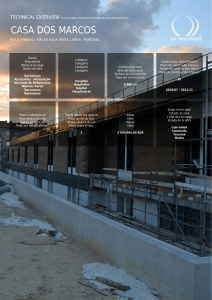
Prostate Cancer Clinical States: December 2015
Sip or AR
or Both
Clinically
Localized
Disease
Rising PSA:
Non-Castrate
Clinical
Metastases
CHAARTED
Rising PSA:
Castrate
AR COMBINATION STUDIES
Sipuleucel studies
Clinical
Metastases:
Castrate:
Sipuleucel
ENZA
Abi
Ra
Clinical
Metastases:
Castrate
1st Line
Docetaxel
Sip or AR
or Both
Clinical
Metastases:
Castrate
2nd Line
Abi
ENZA
Cabazitaxel
Ra
FDA mandated 1st
Line doce vs. CBZ
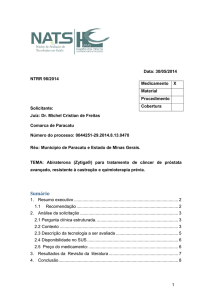
OBITUÁRIO
DES
CIPROTE
RONA
BICALUTA
MIDA
Estudos STRIVE e TERRAIN
Contexto:
• Nos pacientes com tumores de próstata avançados, castração
resistentes, oligosintomáticos, qual a melhor hormonioterapia
a ser combinada com o bloqueio hormonal central?
• Historicamente o uso da bicalutamida, antes das drogas novas
(abiraterona e enzalutamida), ainda é prática bastante
utilizada.
• Dois estudos fase II, randomizados, compararam a
enzalutamida com a bicalutamida neste cenário.
STRIVE – Diagrama CONSORT
STRIVE – Resultados
•
Sobrevida
livre
de
progressão favorece de
forma indubitável o braço
da Enzalutamida
SLP: 19,4 meses versus
5.7 meses (p<0,001)
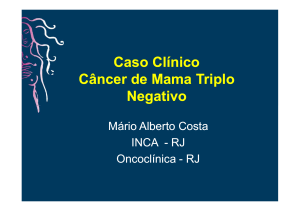
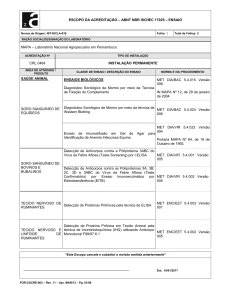
STRIVE – Resultados
Sobrevida Global não foi
atingida no braço da
Enzalutamida
SG de 8,3 meses no braço
da bicalutamida
O resultado sobre o PSA
pode ser visto no
gráfico ao lado, com
uma resposta muito
mais acentuada no
braço da
enzalutamida.
Tratamento mCPRC pós falha ADT
Características
Paciente e Doença
Docetaxel1
(TAX 327)
Abiraterona2
(COU-AA 302)
Enzalutamida3
(PREVAIL)
Radium-2234
(ALSYMPCA)
Sintomáticos
Sim
Não
Não
Sim
Doença Visceral
Sim
Não
Sim
Não
Doença Linfonodal
Sim
Sim
Sim
Não
Resposta
PSA
Sim
Sim
Sim
Não
1.
2.
3.
4.
Tannock IF, et al. N Engl J Med. 2004;351:1502-1512.
Ryan CJ et al. N Engl J Med. 2013;368(2):138-48.
Beer TM. Et al. N Engl J Med. 2014 Jul 31;371(5):424-33
Ryan CJ. Et al. N Engl j Med, 369:213-223, 2013.
Tratamento mCPRC pós falha ADT e Docetaxel
Características
Paciente e
Doença
Cabazitaxel1
(TROPIC)
Sintomáticos
Sim
Sim
Sim
Sim
Doença Visceral
Sim
Sim
Sim
Não
Doença Linfonodal
Sim
Sim
Sim
Não
Resposta
PSA
Sim
Sim
Sim
Não
1.
2.
3.
4.
Abiraterona2 Enzalutamida3
(COU-AA 301)
(AFFIRM)
Radium-2234
(ALSYMPCA)
de Bono JS et al; for the TROPIC Investigators. Lancet 2010;376(9747):1147-1154
de Bono JS, et al. N Engl J Med. 2011;364:1995-2005
Scher HI et al. N Engl J Med, August 2012
Parker CJ. Et al. N Engl j Med, 369:213-223, 2013.
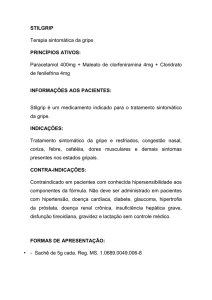
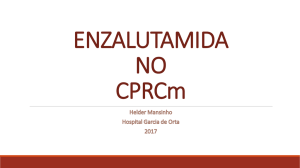
Use of endocrine manipulations without proven
survival benefit in mCRPC
Are endocrine manipulations other than abiraterone or enzalutamide still appropriate treatments for asymptomatic
metastatic CRPC (M1) patients with rising PSA on ADT when abiraterone and/or enzalutamide are available?
16%
1 - Yes, in the majority of patients
32%
2 - In a minority of selected patients
52%
3 - No
0%
10%
20%
Adaptado de Gillessen S. et al. St Gallen Consensus - 2015
30%
40%
50%
60%
70%
80%
90% 100%
First-line Chemotherapy
Asymptomatic/minimally symptomatic
Do you recommend chemotherapy as first-line therapy for otherwise healthy
asymptomatic / minimally symptomatic CRPC patients?
9%
1 - Yes, in the majority of patients
42%
2 - Yes, in a minority of selected patients
49%
3 - No
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Adaptado de Gillessen S. et al. St Gallen Consensus - 2015
First-line Chemotherapy
Asymptomatic / minimally symptomatic with short-response to primary ADT
Do you recommend docetaxel chemotherapy as first-line CRPC treatment in an otherwise healthy
asymptomatic / minimally symptomatic patient with short-response (≤12 months) to primary ADT?
49%
1 - In a minority of selected patients
21%
2- No
30%
3 - Yes, in the majority of patients
0%
10%
20%
Adaptado de Gillessen S. et al. St Gallen Consensus - 2015
30%
40%
50%
60%
70%
80%
90% 100%
First-line Chemotherapy
Symptomatic
Do you recommend chemotherapy (usually taxane based) as first-line therapy for
otherwise healthy symptomatic CRPC patients in addition to ADT?
41%
1 - Yes, in the majority of patients
50%
2 - Yes, in a minority of selected patients
9%
3 - No
0%
10%
Adaptado de Gillessen S. et al. St Gallen Consensus - 2015
20%
30%
40%
50%
60%
70%
80%
90% 100%
Ausência de Metástases
Estadiamento / Imagem
MET Observação
Mantendo ADT
Terapia Hormonal
de Segunda Linha
ABIRATERONA
ENZALUTAMIDA
MET +, sem QTx, Assintomático ou
minimamente sintomático
MET +
DOCETAXEL ASSINTOMÁTICO OU MINIMAMENTE
SINTOMATICO
ABIRATERONA
ENZALUTAMIDA
MET +, sem QTx, Assintomático ou
minimamente sintomático
MET +
DOCETAXEL ASSINTOMÁTICO OU MINIMAMENTE
SINTOMATICO
ABIRATERONA
ENZALUTAMIDA
Metástase visceral
MET +, sem QTx, Sintomático, Bom
PS
DOCETAXEL SINTOMÁTICO
ABIRATERONA
BOM PS
ENZALUTAMIDA
DOCETAXEL
RADIUM 223
MET +, sem QTx, Sintomático, Bom
PS
DOCETAXEL SINTOMÁTICO
ABIRATERONA
BOM PS
ENZALUTAMIDA
DOCETAXEL
RADIUM 223
Metástase visceral
MET +, sem QTx, Sintomático, PS
Ruim
DOCETAXEL SINTOMÁTICO
PS RUIM
ABIRATERONA
ENZALUTAMIDA
DOCETAXEL – CASOS SELECIONADOS
RADIUM 223
CETOCONAZOL
SAMARIO
MET +, sem QTx, Sintomático, PS
Ruim
DOCETAXEL SINTOMÁTICO
PS RUIM
ABIRATERONA
ENZALUTAMIDA
DOCETAXEL – CASOS SELECIONADOS
RADIUM 223
CETOCONAZOL
SAMARIO
Metástase visceral
MET +, pós QTx, Bom PS
DOCETAXEL +
ABIRATERONA
ENZALUTAMIDA
BOM PS
CABAZITAXEL
RADIUM 223
DOCETAXEL
MET +, pós QTx, PS Ruim
DOCETAXEL +
PS RUIM
ABIRATERONA
ENZALUTAMIDA
RADIUM 223
CETOCONAZOL
CUIDADOS PALIATIVOS
Eu Acredito!
Luiz Flávio Coutinho
Tel (31) 2126-8600
E-mail : [email protected]