HERPESVÍRUS HUMANOS
Os herpesvírus humanos (conhecidos)
TIPO
SINONIMIA
Sub-Família
PATOFISIOLOGIA
HHV-1
Vírus do Herpes simples (HSV-1)
Alfa (α)
Herpes oral ou genital (predomina orofacial)
HHV-2
Vírus do Herpes simples 2 (HSV-2)
Alfa (α)
Herpes oral ou genital (predomina orofacial)
HHV-3
Vírus varicela-zoster
Alfa (α)
Varicela ou catapora, herpes zoster
HHV-4
Epstein-Barr
virus (EBV), lymphocryptovirus
γ
(Gamma)
Mononucleose infecciosa, Linfoma de
Burkitt, Linfoma do CNS em pacientes com
AIDS,
sindrome linfoproliferativa pós-transplante
(PTLD), carcinoma nasofarínfgeo
HHV-5
Cytomegalovirus (CMV)
β (Beta)
Síndrome ~ à mononucleose infecciosa,
retinite, doença de inclusão citomegálica.
HHV6, 7
Roseolovirus
HHV-8
Herpesvírus associado ao
sarcoma de Kaposi
(KSHV), um tipo de rhadinovírus
β
γ
(Gamma)
Sexta doença (roséola infantum ou
exantema súbito)
Sarcoma de Kaposi e outros tumores
Família Herpesviridae
• Subfamília:
• Alfaherpesvirinae
– Simplexvirus (Herpes simples humano, ou HSV, ou
HHV-1 e HHV-2 (human herpesvirus type 1 or 2)
– Varicellovirus (vírus da varicela, ou catapora, ou
varicela-zoster, VZV (varicella-zoster virus)
ou HHV-3 (human herpesvirus type 3)
Herpes
Simples Humano
(HSV; HHV1, HHV-2)
- alfaherpesvírus, envelopado
- icosaédricos, 162 capsômeros
- codifica cerca de 70 polipeptídeos
- tipos 1 e 2 muito semelhantes
- latência nos gânglios nervosos
Latência
Infecção
Primária
Gânglio
Nervoso
Genoma
celular
Terminações
nervosas
Genoma
Viral
Núcleo
Latência
Infecção
Primária
neurônios
Gânglio
Nervoso
regional
Latência
Gânglio
Nervoso
Infecção
Primária
Genoma
celular
Terminações
nervosas
Núcleo
Latência
Genoma
celular
Genoma
Viral
Núcleo
Reativação
Gânglio
Nervoso
Genoma
celular
Stress
Imunodepressão
Corticosteróides
UV
Núcleo
Reativação
Com ou
sem
lesões
neurônios
Pele/
mucosas
Gânglio
Nervoso
regional
Reativação
Com ou
sem
lesões
Gânglio
Nervoso
Genoma
celular
Núcleo
Terminações
nervosas
Genoma
Viral
Stress
Imunodepressão
HSV tipo 1; HHV-1:
Doenças associadas:
Herpes labial
Queratite
Estomatites (Aftas)
Herpes labial
(HSV tipo 1; HHV-1)
Herpes labial
(HSV tipo 1; HHV-1)
Lesões herpéticas
Herpes neonatal
Lesões cutâneas
Encefalites
Herpes genital (HSV tipo 2; HHV-2)
HSV
DIAGNÓSTICO:
Clínico
Diagnóstico laboratorial:
rápido: esfregaços de células
- IFD
Isolamento de vírus:
fluido vesicular, swabs nasais e conjuntivais,
abortos, fragmentos de encéfalo, LCR
inoculação em MDBK, e muitas outras
ECP característico em 1-3 dias
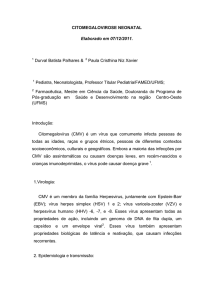
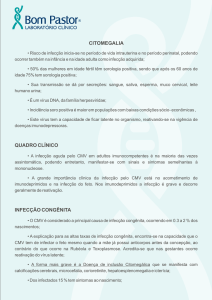
PCR para detecção de
fragmentos de genoma de
HERPESVÍRUS
1
1100 bp
2
3
750 bp
Imunofluorescência- Herpes
Imunoperoxidase (IPX)
Negativo
Positivos
Negativo
ELISA
Positivos
Negativos
HERPESVÍRUS
Sorologia:
- útil na infecção primária (SN, ELISA)
Tipagem de vírus:
- AcMs diferenciais (ELISA)
- SN diferencial
Família Herpesviridae
• Subfamília:
• Alfaherpesvirinae
– Simplexvirus (Herpes simples humano,
ou HSV, ou HHV-1 e 2)
– Varicellovirus (vírus da varicela, ou
catapora, ou varicela-zoster, VZV, ou
HHV-3)
VARICELA
p.i. 14-20 DIAS
EVOLUÇÃO RÁPIDA
ALTAMENTE CONTAGIOSA
LESÕES EM DIFERENTES ESTÁGIOS
VARICELA
DIAGNÓSTICO:
Geralmente clínico em imunocompetentes
No laboratório:
diagn. rápido em células da lesão (início):
IF, IPX
células gigantes
leucopenia
Isolamento em células: VERO, BHK, RK13
1árias de rim de
macaco
ECP em 2 a 14 dias
VARICELA
Lesões
VARICELA
Zoster
HERPES
Tratamento
- Idoxuridina (IDU) uso somente tópico
- Aciclovir e análogos (guanosina acíclica)
ação sobre a timidina quinase viral
- a longo prazo - efeito na recorrência
- ocular : idoxuridina, trifluridina (tópicos)
(resistentes: ácido fosfonofórmico)
NENHUMA DROGA EVITA COMPLETAMENTE
RECORRÊNCIAS !
NENHUMA DROGA AGE SOBRE A LATÊNCIA !
Análogos de nucleosídeos para HSV
Família Herpesviridae
• Subfamília Betaherpesvirinae
– Citomegalovírus (CMV ou HHV-5)
– Roseolovírus (vírus da roséola, HHV-6)
Citomegalovírus (CMV)
-é um betaherpesvírus; HHV 5, um só sorotipo
-latência em células linfóides
-infecção muito prevalente; doença rara:
-(pós natal: mononucleose infecciosa negativa para Acs. Heterófilos)
-( Pré-natal: - neonatos: doença de inclusão citomegálica
- pneumonia em imunocomprometidos
- Quase sempre reativado em transplantados
Citomegalovírus HHV-5
• É o maior membro da família Herpesviridae
• Genoma DNA dupla fita > 240 kbp
• Capacidade codificante de > 200 proteínas.
•
•
•
•
•
Replicação muito vagarosa em cultivo (em contraste com HSV).
O ciclo replicativo é dividido The replication cycle of cytomegalovirus is temporally divided into the
following 3 regulated classes: immediate early, early, and late.
Immediate early gene transcription occurs in the first 4 hours following viral infection, when key
regulatory proteins that allow the virus to take control of cellular machinery are made. The major
immediate early promoter of this region of the cytomegalovirus genome is one of the most powerful
eucaryotic promoters described in nature; this has been exploited in modern biotechnology as a
useful promoter for driving gene expression in gene therapy and vaccination studies.
Following synthesis of immediate early genes, the early gene products are transcribed. Early gene
products include DNA replication proteins and some structural proteins.
Finally, the late gene products are made approximately 24 hours after infection, and these proteins
are chiefly structural proteins that are involved in virion assembly and egress. Synthesis of late genes
is highly dependent on viral DNA replication and can be blocked by inhibitors of viral DNA
polymerase, such as ganciclovir. The lipid bilayer outer envelope contains the virally encoded
glycoproteins, which are the major targets of host neutralizing antibody responses. These
glycoproteins are candidates for human vaccine design. The proteinaceous layer between the
envelope and the inner capsid, the viral tegument, contains proteins that are major targets of host
cell–mediated immune responses. The most important of these tegument proteins is the so-called
major tegument protein, UL83 (phosphoprotein 65 [pp65]).
• Outro produto de gene clinicamente
importante, o UL97, é uma
fosfotransferase. Embora sua função no
ciclo viral seja desconhecida, este gene é
importante porque um substrato da quinase
é o antiviral ganciclovir, que é fosforilado e
torna-se um antiviral anti-citomegalovirus
muito efiaz..
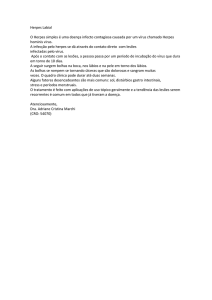
Características - CMV
• Em espécimes clínicos uma característica das infecções por
CMV é a célula com inclusão citomegálica – que dão
origem ao nome do vírus. Estas contém grandes inclusões
intranucleares que lembram um “olho de coruja”.
• A presença destas células indica infecção produtiva,
embora estas possam estar ausentes mesmo em tecidos
ativamente infectados.
• Na maioria das linhagens celulares de laboratório, CMV é
de difícil multiplicação.
• A infecção in vivo envolve principalmente células
epiteliais. Em doença severa disseminada, o vírus pode ser
ientificado na maioria dos órgãos.
Distribuição - epidemiologia
• In developing countries, most children acquire
cytomegalovirus infection early in life, with adult
seroprevalence approaching 100% by early adulthood.
• In contrast, in developed countries, the seroprevalence of
cytomegalovirus approximates 50% in young adults of
middle-upper socioeconomic status.
• This observation has important implications for congenital
cytomegalovirus epidemiology because women of
childbearing age who are cytomegalovirus seronegative are
at major risk of giving birth to infants with symptomatic
congenital infection if primary infection is acquired during
pregnancy.
Transmissão CMV
• Transmissão de CMV pode ocorrer durante toda a
vida, principalmente por contato com secreções
infectadas.
• Infecção com CMV em neonatos é comum.
• Infecção congênita ocorre em aproximadamente
1% (entre 0.5-2.5%) de todos os nascidos estão
infectados com CMV.
• A maioria dessas infecções ocorre em bebês
nascidos de mães como imunidade pré-existente,
sendo os bebês clinicamente assitomáticos.
Entretanto, sequelas de longo termo, incluindo
surdez.
Patogenia da infecção congênitaCMV
• Presume-se que a rota da infecção congênita seja
transplacentária. CMV também pode ser transmitido por via
perinatal, por aspiração de secreções cérvico-vaginais e por
amamentação.
• Mais de 50% dos nascidos alimentados com leite materno que
contém vírus infeccioso são infectados.
• Bebês/crianças que não são infectadas congenitamente tem
alto rico de adquirirem a infecção em creches. Em alguns
estudos, a prevalência de CMV em crianças que frequentam
creches com menos de 2 anos de idade se aproximam de 80%.
• O vírus pode ser prontamente transmitido a crianças suscetíveis
através de saliva, urina e fômites; estas crianças podem
transmitir a infecção a seus pais. Esta transmissão horizontal
em creches parece ser importante na epidemiologia da
infecção em pais jovens adultos.
• Em adultos: atividade sexual provavelmente a forma mais importante
det ransmissão, mas o vírus está presente na saliva, secreções
cervicovaginal, e sêmen.
• Saliva parece ser sufieicnet para infecção e pode ser responsável por
casos de mononucleose negativa para anticorpos heterófilos.
• Beijos parecem ser uma forma de transmissão de crianças para os pais.
• Outras vias importantes de transmissão : transfusões, e transpantes de
órgãos sólidos.
• Em prematuros- sangue deve ser negativo para CMV. Antes disso o
CMV era uma importante causa de mortalidade
• CMV pós- transfusão é ainda um risco em pacientes soronegativos
para CMV, seguidamente se apreentando na forma de hepatite.
• Mortality/Morbidity
• Cytomegalovirus is a substantial cause of morbidity in newborns. As
the most common so-called toxoplasmosis, rubella, cytomegalovirus,
and herpes simplex (TORCH) infection in the developed world,
cytomegalovirus accounts for extensive neurodevelopmental
morbidity, including sensorineural deafness in infants.
Cytomegalovirus also accounts for substantial mortality in
immunocompromised patients.
• Age
• The annual seroconversion rate for acquisition of
cytomegalovirus infection is approximately 1%. However,
two age groups have higher rates of acquisition of
infection: toddlers who attend group daycare and
adolescents. Accordingly, these represent two potential
groups in which to implement vaccination.
Doença de inclusão citomegálica
(CID)
•
•
•
•
•
Cytomegalic inclusion disease (CID)
Approximately 10% of infants with congenital infection have clinical evidence of disease at birth.12 The most severe
form of congenital CMV infection is referred to as CID.
CID almost always occurs in women who have primary cytomegalovirus infection during pregnancy, although rare
cases are described in women with preexisting immunity who presumably have reactivation of infection during
pregnancy.
CID is characterized by intrauterine growth retardation, hepatosplenomegaly, hematological abnormalities
(particularly thrombocytopenia), and various cutaneous manifestations, including petechiae and purpura (ie, blueberry
muffin baby). However, the most significant manifestations of CID involve the CNS. Microcephaly,
ventriculomegaly, cerebral atrophy, chorioretinitis, and sensorineural hearing loss are the most common neurological
consequences of CID.
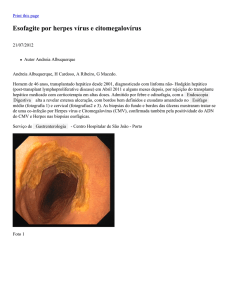
Intracerebral calcifications typically demonstrate a periventricular distribution and are commonly encountered using
CT scanning (see the image below). The finding of intracranial calcifications is predictive of cognitive and audiologic
deficits in later life and predicts a poor neurodevelopmental prognosis.
•
•
•
•
•
•
Cranial CT scan of infant born with symptomatic congenital cytomegalovirus infection. Neurological
involvement is evident, manifest as ventriculomegaly and periventricular calcifications.
[ CLOSE WINDOW ]
Cranial CT scan of infant born with symptomatic congenital cytomegalovirus infection. Neurological
involvement is evident, manifest as ventriculomegaly and periventricular calcifications.
Most infants who survive symptomatic CID have significant long-term neurological and neurodevelopmental
sequelae. Indeed, it has been estimated that congenital cytomegalovirus may be second only to Down syndrome as an
identifiable cause of mental retardation in children.
Infecções com CMV congênitas
assintomáticas
• A maioria dos infectados congenitamente nascem de mulheres com
imunidade pré-existente ao CMV. Estes parecem clinicamente
saudáveis ao nascimento; entretanto, podem ter retardos de
crescimento sutís, e, não obstante estão sob risco de desenvolver
sequelas neurodesenvolvimentais.
• The major consequence of inapparent congenital cytomegalovirus
infection is sensorineural hearing loss. Approximately 15% of these
infants will have unilateral or bilateral deafness. Routine newborn
audiologic screening may not detect cases of cytomegalovirus–
associated hearing loss because this deficit may develop months or
even years after birth.13
Perinatal infection
• Perinatal acquisition of cytomegalovirus usually occurs secondary to
exposure to infected secretions in the birth canal or via breastfeeding.
Most infections are asymptomatic. Indeed, in some reviews,
cytomegalovirus acquired through breast milk has been referred to as a
form of natural immunization.
• Some infants who acquire cytomegalovirus infection perinatally may
have signs and symptoms of disease, including lymphadenopathy,
hepatitis, and pneumonitis, which may be severe. Disease secondary to
acquisition by breast milk is generally limited to premature infants
with low birth weight. These infants may suffer considerable
morbidity. Whether interventions, such as freezing or pasteurization,
are warranted to decrease the risk of transmission to these high-risk
infants is unclear. More studies of long-term neurodevelopmental
outcomes of premature infants who acquire cytomegalovirus infection
perinatally from breast milk are needed.
Cytomegalovirus mononucleosis
• Typical cytomegalovirus mononucleosis is a disease found in young
adults. Although cytomegalovirus mononucleosis may be acquired by
blood transfusion or organ transplantation, cytomegalovirus
mononucleosis is usually acquired via person-to-person transmission.
• The hallmark symptoms of cytomegalovirus mononucleosis are fever
and severe malaise. An atypical lymphocytosis and mild elevation of
liver enzymes are present.
• Clinically differentiating cytomegalovirus mononucleosis from
Epstein-Barr virus (EBV)-induced mononucleosis may be difficult.
Cytomegalovirus mononucleosis is typically associated with less
pharyngitis and less splenomegaly. As with EBV mononucleosis, the
use of b-lactam antibiotics in association with cytomegalovirus
mononucleosis may precipitate a generalized morbilliform rash.
Transfusion-acquired
cytomegalovirus infection
• Posttransfusion cytomegalovirus infection has a
presentation similar to that of cytomegalovirus
mononucleosis. Incubation periods range from 2060 days.
• The use of seronegative blood donors, frozen
deglycerolized blood, or leukocyte-depleted blood
can decrease the likelihood of transmission and is
recommended for high-risk patients (eg, neonates,
immunocompromised patients).
Cytomegalovirus infections in
immunocompromised patients:
• Cytomegalovirus causes various clinical syndromes in
immunocompromised patients. Disease manifestations
vary in severity depending on the degree of host
immunosuppression. Infection may occur because of
reactivation of latent viral infection or may be newly
acquired via organ or bone marrow transplant from a
seropositive donor. Infections may also be mixed in nature,
with donor and recipient isolates both present. Viral
dissemination leads to multiple organ system involvement,
with the most important clinical manifestations consisting
of pneumonitis, GI disease, and retinitis.
Cytomegalovirus pneumonitis
•
•
•
•
Cytomegalovirus is a major cause of pneumonitis in immunosuppressed
children and adults. This disease may be observed in the setting of HIV
infection, congenital immunodeficiency, malignancy, and solid organ or bone
marrow transplant.
The mortality rate is based on the degree of immunosuppression, with
mortality rates of at least 90% reported in bone marrow transplant recipients.
Solid organ transplant recipients are at risk of developing cytomegalovirus
pneumonitis also, although mortality rates are lower.
The illness usually begins 1-3 months following transplantation and starts with
symptoms of fever and dry, nonproductive cough. The illness progresses
quickly with retractions, dyspnea, and hypoxia becoming prominent.
The illness is an interstitial pneumonitis, with a radiographic appearance of
diffuse bilateral interstitial infiltrates. Because the differential diagnosis of
pneumonitis is extensive in immunocompromised patients, consider
performing a bronchoalveolar lavage or open lung biopsy to confirm the
diagnosis and direct appropriate therapy.
Cytomegalovirus GI disease
• GI tract disease caused by cytomegalovirus can include esophagitis,
gastritis, gastroenteritis, pyloric obstruction, hepatitis, pancreatitis,
colitis, and cholecystitis. Characteristic signs and symptoms may
include nausea, vomiting, dysphagia, epigastric pain, icterus, and
watery diarrhea.
• Stool may be Hemoccult positive or frankly bloody. Endoscopy and
biopsy are warranted, and characteristic cytomegalic inclusion cells
may be observed in GI endothelium or epithelium.
• Although CMV enteritis does not carry the same ominous prognosis as
cytomegalovirus pneumonitis, antiviral therapy is warranted.
• Differentiating cytomegalovirus hepatitis from chronic rejection in
liver transplant patients may be difficult, even with biopsy.
Cytomegalovirus retinitis
• Antes da “highly active antiretroviral therapy (HAART)”
para HIV, a retinite por CMV era a causa mais comum de
cegueira em adultos com AIDS, com prevalência de mais
de 90%
• HIV-associated cytomegalovirus retinitis in children, in
contrast to adults, has been relatively rare, probably
reflecting overall differences in cytomegalovirus
seroprevalence between the populations. Retinitis is less
common in transplant patients.
• Cytomegalovirus produz um retinite necrótica de
progressão rápida, com caraterístico infiltrado perivascular
de leucócito com hemorragia (brushfire retinitis).
• Peripheral lesions may be asymptomatic, and even
advanced disease does not cause pain. In children,
strabismus or failure to fix and follow objects may be
Citomegalovírus (CMV)
TRANSMISSÃO E EPIDEMIOLOGIA:
- Anticorpos em ~80% adultos
- eliminação de vírus esporádica
- através do leite => mais comum
- transmissão sexual (sêmen, secr. cervicais)
- transmissão por hemoderivados
- transplantados renais: reativação e disseminação do vírus
INFECÇÃO PÓS-NATAL:
CMV
- geralmente na infância (Mononucleose Infecciosa rara)
- É causa comum de retinites
- infecção em adultos
= maior chance de mononucleose infecciosa
- pode ocorrer durante o parto
CMV
INFECÇÃO PRÉ-NATAL:
- pode ocorrer em qualquer estágio da gestação
- risco de transmissão: 0,2 a 2%
- 5 a 15% destes podem apresentar lesões congênitas
- infecção intrauterina => crianças disseminam o vírus
por mais tempo
- Maior risco = quando ocorre a infecção 1ária na gestação
- infecção prévia = risco muito baixo
CMV
Infecção intrauterina
Sinais clínicos:
- microcefalia
- convulsões
- icterícia
- hepatosplenomegalia
- retardo mental
- surdez (mais comum)
CMV
Congênito
Doença de
inclusão
citomegálica
CMV
Infecção pós-natal:
- MI heterófilo- negativa;
- Febre, letargia, linfócitos anormais no
sangue periférico;
- usualmente sem faringite ou linfadenopatia
-retinites
- às vezes após transfusão com sangue fresco
(vírus inativado em refrigeração)
Doença de inclusão citomegálica
As duas mononucleoses:
CMV
EBV
CMV
Em imunodeprimidos:
- infecções frequentes
- transplantes renais: assintomáticas
- grave em transpl. de medula e coração =>
pneumonia intersticial e retinite
CMV
Diagnóstico virológico:
- PCR (rapidamente se tornando de eleição)
- Urina, lavados de garganta, sangue não coagulado
- isolamento de vírus ( demorado) : 1-2 semanas em céls embrionárias de pulmão humano
WI 38 ou MRC 5)
- Detecção de focos fluorescentes: em 24-48 h
- Histologia : inclusões (“olho de coruja”) em células gigantes: urina
glândulas salivares
fígado
pulmão
CMV - Imunofluorescência
(Virology Laboratory, Yale-New Haven Hospital)
Teste de antigenemia para p65
do CMV
(Virology Laboratory, New-Yale Haven Hospital)
Infecção pelo
Citomegalovírus
DIAGNÓSTICO SOROLÓGICO (pouca utilidade):
- IgM alta=> infecção aguda
- IgM baixa e IgG alta= infecção prévia
- aumento no título de Anticorpos igual ou maior do que 4 vezes = significativo
CMV -
Tratamento:
- acyclovir : não muito eficaz
- ganciclovir (em pneumonias e retinites)
- foscarnet (retinites): inibidor da
DNA polimerase viral
CMV
Prevenção:
- não há vacina
- transfusões em neonatos => a partir de
soronegativos
- transplantes (se possível) => de
soronegativos para soronegativos
Família Herpesviridae
• Subfamília:
Gammaherpesvirinae
– Lymphocryptovirus (vírus Epstein-Barr, EBV, ou herpesvírus
humano tipo 4 HHV-4)
- Latência em células linfóides
- Alta prevalência na população
Mononucleose infecciosa
Transmissão / Patogenia
- transmissão por saliva (90% adultos +)
- vírus intermitente na saliva
- 10-5 a 10 -6 linfócitos infectados
- orofaringe => linf. B => Linf T reagem =>
muitas cópias do genoma no citoplasma;
poucas integradas no genoma.
MONONUCLEOSE INFECCIOSA
- EBV 1 = na maioria das populações caucasianas
- EBV 2 = africanos (50% de afric. com linf. Burkitt)
- EBV 1 e 2 diferem em somente 5 genes
que codificam EBNA na latência
- células epiteliais e linfócitos B
(lítica somente epiteliais)
- adsorção nos linfócitos via receptor de C3
- linfócitos T
Mononucleose Infecciosa - EBV
Células alvo = Linfócitos B não sensibilizados
Os quais são estimulados a proliferar continuamente…
- Podem se multiplicar seriadamente (dão origem a
linhagens linfoblastóides)
- Em suma, os linfócitos B infectados se comportam como
se tivesse sido sensibilizados por antígenos: secretam proteínas,
Imunoglobulinas, sofrem trocas de trocas de classe…
MONONUCLEOSE INFECCIOSA
“Clássica”
ou
“Mononucleose Paul-Bunnel positiva”
A “mononucleose” = consiste de
linfócitos T atípicos,
maiores, com o
citoplasma vacuolizado e o
núcleo deformado e lobulado
Mononucleose infecciosa
CARACTERÍSTICAS CLÍNICAS:
-
Síndrome agudo
Febre, dor de garganta, mal-estar, linfadenopatia
Esplenomegalia
Eritema maculopapular (< 15%). Ampicilina eleva a >90%.
Mononucleose com linfócitos T atípicos (10% - 30%)
Linfocitose > 50% (incluso os 10%)
Anticorpos heterófilos
Anomalias de funções hepáticas são freqüentes.
Mononucleose Infecciosa - EBV
Mononucleose infecciosa
Diagnóstico:
- Teste de Paul Bunnel (Anticorpos heterófilos)
- IgM específica anti-ag capsídeo viral (ACV)
- IgG anti- ACV em elevação
- anti-EBNA: 3-4 semanas p.i. e persiste por toda a vida
Mononucleose infecciosa
Associação com cânceres linfóides:
Linfoma de Burkitt em crianças africanas
Carcinoma nasofaríngeo (CNF) => (China)
Linfoma de Burkitt
Outros herpesvírus humanos:
HHV-6: exantema súbito ou roséola
HHV-7: igual ao HHV-6
HHV-8: herpesvírus associado ao
Sarcoma de Kaposi (KSHV)
Herpesvírus Humano 8 (HHV-8)
• Associado à ocorrência do Sarcoma de Kaposi (KS) e outros
linfomas menos conhecidos.
• KS prevalente em homossexuais masculinos com AIDS.
(DNA viral em 100% dos casos de KS).
• A maioria dos pacientes com KS tem anticorpos anti-HHV-8.
• A soroprevalência de anticorpos anti-HHV-8 é baixa na população
em geral, mas alta em suscetíveis ao KS, como homossexuais
masculinos.
• Diferente dos demais herpes humanos, o HHV-8 não tem
distribuição ubíqua.
Fim do bloco