PowerPoint Slides
English Text
Brazilian Portuguese Translation
Treatment Modalities: Drug Therapy, Part 2
VideoTranscript
Modalidades de Tratamento: Terapia
a
Medicamentosa, 2 Parte
Transcrição do vídeo
Educação Profissional em Oncologia
Modalidades de Tratamento: Terapia
a
Medicamentosa, 2 Parte
Duração: 18:16
Jeffrey Bryan, Pharm.D.
Especialista em Farmácia Clínica
Programas de Farmácia Clínica
MD Anderson Cancer Center – Universidade do
Texas
Olá, eu sou Jeffrey Bryan. Sou especialista em
farmácia clínica no MD Anderson Cancer Center da
Universidade do Texas. Gostaria de dar-lhes as
boas-vindas à segunda parte das Modalidades de
Tratamentos: Terapia Medicamentosa.
Professional Oncology Education
Treatment Modalities: Drug Therapy, Part 2
Time: 18:16
Treatment Modalities:
Drug Therapy Part II
Jeffrey Bryan, Pharm.D.
Clinical Pharmacy Specialist
Pharmacy Clinical Programs
The University of Texas MD Anderson Cancer
Center
Hello, my name is Jeffrey Bryan. I am a Clinical
Pharmacy Specialist with The University of Texas
MD Anderson Cancer Center. I would like to
welcome you to the second part of Treatment
Modalities: Drug Therapy.
Treatment Modalities:
Drug Therapy – Part II
Jeffrey Bryan, Pharm.D.
Clinical Pharmacy Specialist
Pharmacy Clinical Programs
1
Treatment Modalities:
Drug Therapy Part II
Objectives
Upon completion of this lesson, participants will
be able to:
• Discuss the goals and roles of drug therapy
Upon completion of this lesson, participants should
be able to discuss the goals and roles of drug
therapy; identify classifications of chemotherapy;
differentiate between chemotherapy, hormone
therapy, immune-based therapy, and targeted
therapy; and identify some common toxicities
associated with chemotherapeutic agents.
Na conclusão desta apresentação, os participantes
devem ser capazes de discutir os objetivos e as
funções da terapia medicamentosa, de identificar as
classificações da quimioterapia e de diferenciar a
quimioterapia, hormonoterapia, imunoterapia e
terapia alvo, além de identificar as toxicidades
comuns associadas aos agentes quimioterápicos.
At first, we will start off with immune-based therapy,
then discuss targeted therapy.
Primeiro, começaremos com a
depois, discutiremos a terapia alvo.
• Identify classifications of chemotherapy
• Differentiate between chemotherapy, hormone,
immune-based, and targeted therapy
• Identify common toxicities of drug treatment
Treatment Modalities:
Drug Therapy Part II
imunoterapia;
Immune-based Therapy and
Targeted Therapy
2
Treatment Modalities:
Drug Therapy Part II
ImmuneImmune-based Therapy
• Treatment with agents from biologic sources
and/or agents able to affect biologic responses
• Stimulates host’s immune system to fight
against cancer
The idea of stimulating or augmenting the body’s
own immune system to fight or prevent cancer led to
the development of immune-based therapies. This
is now referred to by many as the fourth cancer
treatment modality. The idea is to use various
cytokines and other biologic response modifiers,
such as interferon, monoclonal antibodies, and
vaccines, to stimulate the host immune system to
attack the tumors.
A ideia de estimular ou reforçar o sistema
imunológico do organismo para combater ou
impedir o câncer levou ao desenvolvimento de
imunoterapias. Hoje, muitos se referem a essa ideia
como sendo a quarta modalidade de tratamento
antineoplásico. A ideia é utilizar várias citocinas e
outros modificadores da resposta biológica, como o
interferon, anticorpos monoclonais e vacinas, para
estimular o sistema imunológico do hospedeiro e
atacar tumores.
Interferons, interleukins are part of a family of
cytokines and proteins that are normally produced in
the body in response to stress or inflammation.
Genetically-engineered interferon and interleukin
have been shown to have anti-tumor effects in
several malignancies. Although their toxicities differ
from conventional chemotherapy, they are
associated with a constellation of symptoms, such
as fever, chills, myalgias, depression, and
sometimes myelosuppression.
Os interferons, as interleucinas, formam parte de
uma família de citocinas e proteínas normalmente
produzidas no corpo em resposta ao estresse ou à
inflamação. O interferon e a interleucina
geneticamente modificados demonstraram ter
efeitos antineoplásicos em diversos cânceres.
Embora sua toxicidade seja diferente da
quimioterapia convencional, está associada a uma
constelação de sintomas, como febre, calafrios,
mialgias, depressão e, às vezes, mielossupressão.
• A means to deliver systemic anticancer therapy
Treatment Modalities:
Drug Therapy Part II
ImmuneImmune-based Therapy Interferons/Interleukins
• Cytokines - proteins that are normally produced in
the body in response to stress
• Act as chemical signals to:
–
–
–
–
Directly slow tumor growth
Slow angiogenesis (formation of new blood vessels)
Stimulate cancer cells to produce antigens
Stimulate immune system cells to attack cancer cells
• Interferon-alfa: CML, melanoma, lymphoma
• Interleukin-2 (IL-2): melanoma, renal cell
3
Treatment Modalities:
Drug Therapy Part II
ImmuneImmune-based Therapy Monoclonal Antibodies (MoAb)
• Developed to target specific proteins/antigens
involved in the development and progression
of cancer
• High specificity to tumor-specific targets
In recent years, a number of monoclonal antibodies
have been developed for the treatment of patients
with a variety of cancers. These agents target
specific proteins or antigens that are expressed on
tumor cells. Additionally, these agents can be given
as a single agent or in combination with
conventional chemotherapy without overlapping or
increasing toxicity.
Nos últimos anos, foram desenvolvidos diversos
anticorpos monoclonais para o tratamento de
pacientes com diferentes cânceres. Esses agentes
atacam proteínas ou antígenos específicos
expressos nas células tumorais. Além disso, podem
ser administrados sozinhos ou em combinação com
a quimioterapia convencional sem sobreposição ou
aumento da toxicidade.
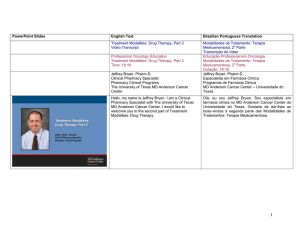
Monoclonal antibodies are synthesized from
different sources.
The majority of monoclonal
antibodies are chimeric, meaning that they have a
murine variable region fused to a human constant
region or humanized, meaning they are
predominantly of human origin.
Os anticorpos monoclonais são sintetizados de
diferentes fontes. A maioria dos anticorpos
monoclonais é quimérica; isto é, têm uma região
variável murina ligada a uma região constante
humana ou humanizada, que significa serem de
origem predominantemente humana.
• Different toxicity profile from conventional
cytotoxic agents
• Synergy with chemotherapy agents
Treatment Modalities:
Drug Therapy Part II
Monoclonal Antibodies (MoAbs)
• Four Types of MoAbs
Murine (100% Murine)
Chimeric (30% Murine, 70% human)
Humanized (5% Murine, 95% human)
Human (100% human)
Mouse (Murine = Mouse)
Human
4
Treatment Modalities:
Drug Therapy Part II
Monoclonal Antibodies Conjugated vs. Unconjugated
Treatment Modalities:
Drug Therapy Part II
ImmuneImmune-based Therapy Monoclonal Antibodies
Additionally, monoclonal antibodies can be
conjugated
or
unconjugated.
Conjugated
monoclonal antibodies have a toxin or a
radionucleotide attached to the antibody that allows
the toxin to be delivered to the tumor. Whereas
unconjugated monoclonal antibodies rely on
activating the host immune system, which in turn
attacks the tumor.
Além disso, os anticorpos monoclonais podem ser
conjugados ou não conjugados. Os anticorpos
monoclonais conjugados têm uma toxina ou um
radionucleotídio ligado ao anticorpo que permite
que a toxina seja entregue ao tumor. Em
comparação, os anticorpos não conjugados contam
com a ativação do sistema imunológico, que, por
sua vez, ataca o tumor.
This is a list of some of the FDA-approved
monoclonal antibodies along with their main
characteristics and indications. You can see that
each monoclonal antibody has a very specific
antigen it targets. For example, rituximab targets
CD20 on B-cells and gemtuzumab target CD33 on
myeloid cells.
Esta é uma lista de alguns anticorpos monoclonais
aprovados pela FDA com suas principais
características e indicações. Vocês podem ver que
cada anticorpo monoclonal tem como alvo um
agente bem específico. Por exemplo, o alvo do
rituximabe é o CD20 em células B e o alvo do
gemtuzumab é o CD33 em células mieloides.
5
Treatment Modalities:
Drug Therapy Part II
Targeted Therapy
• Agents that specifically target cell processes that
are aberrant or more abundant in malignant cells
than normal cells
• Target cellular processes and signaling pathways
that affect:
–
–
–
–
Cell growth and differentiation
Angiogenesis (new blood vessel formation)
Apoptosis (programmed cell death)
Cell motility
Treatment Modalities:
Drug Therapy Part II
Targeted Therapy (continued)
• Systemic-like chemotherapy designed to target
cancer cells
• Optimal targets vary widely between cancers
• Effectiveness depends on the expression of
target antigen, receptor, or other molecules
• Different toxicity profile from conventional
cytotoxic agents
We have discussed conventional chemotherapy,
hormone therapy, and immune-based therapy.
Now, I will spend some time discussing what is
called targeted therapy and the implications on the
treatment of cancer. A major limitation of current
cytotoxic therapy is the lack of sensitivity on
malignant cells. Chemotherapy can affect any cell
that is rapidly dividing whether it be normal or
malignant. As our knowledge of tumor biology
increases, novel therapeutic strategies, such as
targeted therapy have evolved. What is unique
about targeted therapy [is] that it targets processes.
Targeted therapy blocks growth of cancer cells by
interfering with specific molecules, a process very
different from conventional chemotherapy, hormone
therapy, and immune-based therapy.
Similar to conventional chemotherapy, targeted
therapy is considered systemic therapy, but
designed to affect predominantly cancer cells. For
this reason, these drugs are associated with very
different and sometimes less side effects. The
effectiveness of these drugs often depends on the
expression of the target antigen receptor and other
molecules on the cancer cells. A benefit of targeted
therapy is that they often come in oral formulations.
Já discutimos a quimioterapia convencional, a
hormonoterapia
e
a
imunoterapia.
Agora,
dedicaremos parte do nosso tempo discutindo o
que se conhece como terapia alvo e as implicações
no tratamento do câncer. A principal limitação da
terapia citotóxica atual é a falta de sensibilidade nas
células malignas. A quimioterapia pode afetar
qualquer célula que se divida rapidamente, seja
normal ou maligna. Com o aumento do
conhecimento sobre a biologia dos tumores,
surgem novas estratégias terapêuticas, como a
terapia alvo. O aspecto singular da terapia alvo [é]
ser dirigida aos processos. A terapia alvo bloqueia o
crescimento das células tumorais interferindo em
moléculas específicas, um processo muito diferente
do da quimioterapia convencional, hormonoterapia
e imunoterapia.
À semelhança da quimioterapia convencional, a
terapia alvo é considerada uma modalidade
sistêmica, mas projetada para afetar principalmente
as células tumorais. Por essa razão, esses
fármacos estão associados a efeitos secundários
bastante diferentes e, às vezes, a um menor
número deles. Frequentemente, a eficácia desses
fármacos depende da expressão do receptor do
antígeno alvo e outras moléculas nas células
tumorais. Um benefício da terapia alvo é que,
frequentemente, é oferecida em formulações orais.
• Intravenous and oral formulations
6
Treatment Modalities:
Drug Therapy Part II
Targeted Therapy - Mechanism of Action
Treatment Modalities:
Drug Therapy Part II
Targeted Therapy - Mechanism of Action
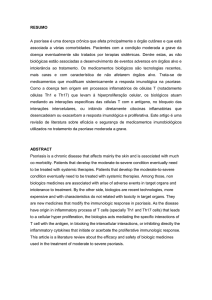
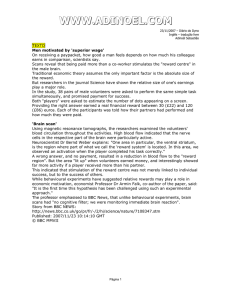
This diagram shows the different targets for drug
therapy. You can see that outside of the cell, or on
the cell surface, there are growth factors that bind to
the receptors. The binding triggers a cascade of
intracellular events involving many tyrosine kinases.
This results in increasing cell growth, proliferation,
and differentiation along with angiogenesis. By
inhibiting one of these proteins, you can prevent the
downstream effects.
Este diagrama mostra os diferentes alvos da terapia
medicamentosa. Vocês podem ver que na parte
externa da célula, ou na sua superfície, há fatores
de crescimento que se ligam aos receptores. A
ligação desencadeia uma cascata de eventos
intracelulares nas quais participam muitas tirosinoquinases. Isso resulta no aumento do crescimento,
proliferação e diferenciação celular, juntamente com
a angiogênese. Ao inibir uma dessas proteínas,
pode-se impedir os efeitos posteriores.
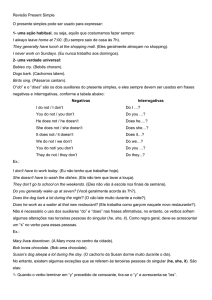
This is another depiction of the targets for some of
our monoclonal antibodies and/or tyrosine kinase
inhibitors. For instance, gemtuzumab targets the
CD33. Gemtuzumab is complexed with a toxin
called calicheamicin. Upon binding the CD33, the
calicheamicin is engulfed by the cell, which causes
ultimate cell death. On the bottom half of this
picture, a lot of these monoclonal antibodies are
used for solid tumors.
But these target cell
processes. And internally a lot of the tyrosine
kinases such as imatinib and dasatinib target
pathways that are responsible for cell differentiation
and cell survival.
Esta é outra ilustração dos alvos para alguns dos
anticorpos monoclonais e/ou inibidores da tirosinoquinase. Por exemplo, o alvo do gemtuzumab é o
CD33. O gemtuzumab forma um complexo com
uma toxina denominada calicheamicina. Após ligarse ao CD33, a calicheamicina é engolfada pela
célula, causando sua morte. Na parte inferior desta
foto, muitos destes anticorpos monoclonais são
utilizados para tumores sólidos, mas seus alvos são
processos celulares. E, internamente, os alvos de
muitas das tirosino-quinases, como imatinibe e
dasatinibe, são as rotas responsáveis pela
diferenciação e sobrevivência das células.
7
Treatment Modalities:
Drug Therapy Part II
Targeted Therapy - Summary of Agents
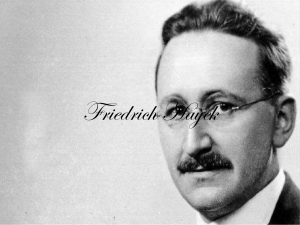
This list lists --- this table lists many FDA-approved
targeted
therapies
and
summarizes
their
mechanisms of action, targets, and indications. For
example, bevacizumab targets VGEF, which is the
vascular endothelial growth factor. And cetuximab
covers --- cetuximab binds to the epidermal growth
factor receptor. And we get a whole list of tyrosine
kinase inhibitors, which target the cell processes
within the cell, for instance, imatinib, dasatinib and
erlotinib.
Esta lista relaciona... esta tabela relaciona muitas
terapias alvo aprovadas pela FDA e resume seus
mecanismos de ação, alvos e indicações. Por
exemplo, o alvo do bevacizumabe é o VGEF, que é
o fator de crescimento endotelial vascular. E o
cetuximabe cobre... o cetuximabe liga-se ao
receptor do fator de crescimento epidérmico. E
temos toda uma lista de inibidores da tirosinoquinase, cujos alvos são os processos celulares
dentro da célula, por exemplo, imatinibe, dasatinibe
e erlotinibe.
In summary, immune-based therapy and targeted
therapy blocks the growth of cancer cells by
interfering with specific targeted molecules needed
for tumor growth. These play an important role for
monotherapy and in combination in chemotherapy
for the treatment of cancers. And this is the future of
cancer drug development.
Resumindo, a imunoterapia e a terapia alvo
bloqueiam o crescimento de células tumorais ao
interferir
com
moléculas
alvo
específicas
necessárias para o crescimento do tumor. Essas
terapias desempenham um importante papel na
monoterapia e em combinação na quimioterapia
para o tratamento do câncer. E este é o futuro do
desenvolvimento de antineoplásicos.
Vascular endothelial growth factor = VEGF
Epidermal growth factor receptor = EGFR
Tyrosine kinase inhibitor = TKI
Platelet-derived growth factor receptor = PDGFR
Treatment Modalities:
Drug Therapy Part II
ImmuneImmune-based and Targeted Therapy Summary
• Blocks the growth of cancer cells by interfering with
specific targeted molecules needed for tumor growth
• Important role as monotherapy or in combination with
chemotherapy for the treatment of cancers
• Future of cancer drug development
8
Treatment Modalities:
Drug Therapy Part II
Now we are going to switch gears a little bit and talk
about dosing and toxicity.
Agora, mudaremos um pouco de assunto e
falaremos sobre doses e toxicidade.
Conventional chemotherapy is generally dosed off
of BSA, which is calculated off the height and weight
2
of the patient. For instance, a dose of 20 mg/m in
the BSA of a patient is 2, the dose will be 40 mg.
Oftentimes, single-agent chemotherapy is used in
the palliative role, but it is generally less toxic and
less toxic to cancer cells, whereas chemotherapy
given in combination capitalizes on different
mechanisms of action of the chemotherapy for
achieving greater cell kill and preventing resistant
cell lines.
Geralmente, na quimioterapia convencional, a dose
é obtida levando em conta a superfície corporal,
que é calculada utilizando a altura e o peso do
2
paciente. Por exemplo, a dose de 20 mg/m na
superfície corporal de um paciente é 2, a dose será
de 40 mg. Com frequência, a quimioterapia de um
único agente é utilizada na função paliativa, mas é
geralmente menos tóxica e menos tóxica para as
células tumorais, enquanto que a quimioterapia
administrada em combinação capitaliza diferentes
mecanismos de ação da quimioterapia por alcançar
uma grande morte celular e impedir linhagens
celulares resistentes.
Dosing and Toxicity
Treatment Modalities:
Drug Therapy Part II
Dosing Strategies
• Body Surface Area (BSA)
– BSA(m2) =
√
height (cm) x weight (kg)
3600
• Single Agent Chemotherapy
– Less toxicity to normal tissue BUT
less toxicity to cancer cells
– Palliative role
• Combination Chemotherapy
– Different mechanisms of action
– Greater cell kill
– Fewer resistant cell lines
9
Treatment Modalities:
Drug Therapy Part II
Dosing Strategies (continued)
• Dose Intensity - dose delivered over a specified
period of time (mg/m2/week)
– ⇑ dose intensity = ⇑ response rate
– Leukemias, lymphomas, breast, ovarian
• Dose Density - shortening the usual interval between
doses; designed to maximize the drug’s effects on
tumor growth kinetics
– May require growth factor support
Treatment Modalities:
Drug Therapy Part II
Common Drug Therapy Toxicities
• Gastrointestinal toxicity
• Cardiotoxicity
• Neurotoxicity
Now that we are familiar with dosing chemotherapy,
effecting --- effective dosing can be a factor limiting
the ability of chemotherapy to achieve a cure. There
are generally two types of dosing strategies: dose
intensity and dose density. Dose intensity is the
total amount of drug administered at one time or
over a week, every 28 days for instance. There can
be a positive relationship between dose intensity
and response rate. However, there is also a
correlation with increased toxicity with dose intense
regimens. Dose density, on the other hand - you
give the drug, give smaller doses of the drug more
often, for instance, once a week or every two
weeks.
Agora que nos familiarizamos com a dose na
quimioterapia, a dose eficaz pode ser um fator
limitante da capacidade de a quimioterapia alcançar
a cura. Em geral, existem dois tipos de estratégias
para as doses: intensidade da dose e densidade da
dose. Por exemplo, a intensidade da dose é a
quantidade total do fármaco administrada uma vez
ou durante uma semana cada 28 dias. Pode haver
uma relação positiva entre a intensidade da dose e
a taxa de resposta. No entanto, também existe uma
correlação entre esquemas com doses intensas e
aumento da toxicidade. Por outro lado, quanto à
densidade, a dose é administrada em pequenas
quantidades e com mais frequência; por exemplo,
uma vez por semana ou cada duas semanas.
The ideal chemotherapeutic medication will kill
tumor cells and spare normal cells. Unfortunately,
this is not the case when it comes to most --- most
chemotherapy. Toxicities from chemotherapy can
potentially affect any organ in the body and result in
affecting both the patient’s quality of life and
treatment outcomes. I will spend some time going
over some of the toxicities of chemotherapy.
O medicamento quimioterápico ideal destrói as
células tumorais e preserva as células normais.
Infelizmente, não é o caso da maioria das
quimioterapias. As toxicidades da quimioterapia
pode afetar qualquer órgão do corpo e,
consequentemente, a qualidade de vida e os
resultados do tratamento do paciente. Dedicarei
parte do nosso tempo à discussão de algumas
toxicidades da quimioterapia.
• Hepatotoxicity
• Nephrotoxicity
• Dermatologic toxicity
• Myelotoxicity
10
Treatment Modalities:
Drug Therapy Part II
Drug Therapy Toxicity
• Factors that may influence treatment toxicity
– Dose of chemotherapy
• High dose vs. low dose
– Treatment schedule
• Weekly vs. biweekly vs. monthly
– Combination therapy
• Anthracycline with antimetabolite
– Patient specific factors
• Age, BSA, organ function, comorbidities,
response to prior therapies
But, before we do this, there are many factors that
influence treatment toxicity, for instance the dose of
chemotherapy, the treatment schedule, whether the
chemotherapy is given in combination or as a single
agent, and patient-specific factors, such as age.
Elderly patients have less --- are less tolerable of
chemotherapy, oftentimes because they might have
poor organ function or other comorbidities.
Additionally, the method of administration, whether it
is given continuous versus bolus, can affect the
toxicity of the drug. And you have to consider other
drugs and
herbal products when
giving
chemotherapy as well.
Mas, antes disso, existem muitos fatores que
afetam a toxicidade do tratamento, por exemplo, a
dose da quimioterapia, o horário do tratamento, se
a quimioterapia for administrada em combinação ou
como agente único, além de fatores específicos dos
pacientes, como a idade. Os pacientes idosos são
menos tolerantes à quimioterapia, frequentemente
por causa do mau funcionamento dos órgãos ou
outras comorbidades. Além disso, o método de
administração, se for contínuo ou em bolus, pode
afetar a toxicidade do fármaco. E temos que
considerar outros fármacos e produtos à base de
ervas quando a quimioterapia for administrada.
Nausea and vomiting are common side effects of
chemotherapy and are feared by most patients. In
the setting of chemotherapy, nausea and vomiting is
medically known as chemotherapy-induced nausea
and vomiting.
It is often the first side effect of
patients that --- it is often the first side effect patients
experience.
Nausea and vomiting can be
characterized as acute, occurring within the first 24
hours of starting chemotherapy, or delayed nausea
and vomiting occurs within 24 hours after
chemotherapy. Breakthrough nausea and vomiting
is that which occurs despite being on medication to
preventive it. Refractory nausea and vomiting is
that that does not respond at all to treatment.
Finally, anticipatory nausea and vomiting is when a
patient experiences symptoms prior to starting their
next cycle of chemotherapy.
Náuseas e vômitos são efeitos colaterais comuns
da quimioterapia e temidos pela maioria dos
pacientes. No ambiente de quimioterapia, são
conhecidos clinicamente como náuseas e vômitos
induzidos por quimioterapia. Com frequência, é o
primeiro efeito colateral que os pacientes
apresentam. As náuseas e os vômitos podem ser
caracterizados como agudos, quando ocorrem nas
primeiras 24 horas do início da quimioterapia, ou
tardios, quando ocorrem nas 24 horas após a
quimioterapia. As náuseas e os vômitos incidentais
são aqueles que ocorrem mesmo tomando
medicamentos para evitá-los. As náuseas e os
vômitos refratários são os que não respondem ao
tratamento. Finalmente, as náuseas e os vômitos
antecipatórios ocorrem quando o paciente
experimenta sintomas antes de iniciar o próximo
ciclo de quimioterapia.
– Method of administration
• Continuous vs. bolus
– Drug-drug and drug-herbal interactions
Treatment Modalities:
Drug Therapy Part II
Gastrointestinal Toxicity
• Nausea and vomiting
– Most common early manifestation of toxicity
– Mechanisms
• Stimulation of chemoreceptor zones
• Damage to gastrointestinal mucosa
• Alterations in taste and smell
• Five distinct clinical syndromes
–
–
–
–
–
Acute: < 24 hours after chemotherapy
Delayed: ≥ 24 hours after chemotherapy
Breakthrough: Symptoms despite prophylaxis
Refractory: Ineffective treatment
Anticipatory: Symptoms prior to therapy
11
Treatment Modalities:
Drug Therapy Part II
Emetogenic Potential of Commonly
used Agents
Interestingly, not all chemotherapeutic agents cause
the same degree of nausea or vomiting. There are
several
classification
systems
that
define
emetogenicity of chemotherapy. And this helps us
choose what kind of antiemesis regimen we will use.
Although this table is not all inclusive, it shows
examples of chemotherapeutic agents that are
thought to be of high emetogenic risk and
associated with minimal emetogenic risk. As you
may have noticed, the emetogenic potential - some
chemotherapy is dose --- dose-dependent.
Curiosamente,
nem
todos
os
agentes
quimioterápicos causam o mesmo grau de náuseas
e vômitos. Existem vários sistemas de classificação
que definem a emetogenicidade da quimioterapia.
Essa informação facilita a escolha do regime
antiemético que usaremos. Embora esta tabela não
seja completamente abrangente, mostra exemplos
de agentes quimioterápicos que supostamente são
de alto risco emetogênico e estão associados a
mínimos riscos emetogênicos. Como podem ter
observado, o potencial emetogênico... algumas
quimioterapias são dependentes da dose.
And, if nausea and vomiting is not enough, certain
agents also destroy the mucosal lining throughout
the gastrointestinal tract.
Tissue lining this
gastrointestinal tract is usually rapidly dividing cells.
Hence, these cells are susceptible to the actions of
chemotherapy. Agents, such as methotrexate and
5-fluorouracil,
can
cause
mucositis
and
inflammatory reactions of the mucosal lining.
Irinotecan, used for the treatment of colon cancer,
almost always causes diarrhea, whereas vincristine
does the opposite, causes constipation.
E, como se não bastassem as náuseas e os
vômitos, alguns agentes também destroem a
mucosa que reveste todo o trato gastrointestinal. O
tecido que reveste o trato gastrointestinal é
constituído por células que se dividem rapidamente.
Por isso, essas células são suscetíveis aos efeitos
da quimioterapia. Agentes, como o metotrexato e o
5-flurouracilo, podem causar mucosite e reações
inflamatórias na mucosa. O irinotecano, utilizado
para o tratamento do câncer de cólon, quase
sempre causa diarreia, embora a vincristina cause o
oposto, constipação.
NCCN v.1.2010 Antiemesis Practice Guidelines
http://www.nccn.org/professionals/physician_gls/PDF/antiemesis.pdf
Treatment Modalities:
Drug Therapy Part II
Gastrointestinal Toxicity
• Mucositis
– Inflammatory reaction and ulcerative lesions
of mucosal surfaces
– Most commonly caused by methotrexate,
5-fluorouracil, vinca alkaloids
• Diarrhea
– Common adverse effect of irinotecan
• Constipation
– Common adverse effect of vincristine
12
Treatment Modalities:
Drug Therapy Part II
Cardiotoxicity
• Rare but serious complication of cancer therapy
• Incidence and severity depends on agent, dose,
schedule, patient factors, and other treatments
• Cardiomyopathy
A rare, but serious, complication with some
chemotherapy agents is cardiotoxicity. Cardiotox --Cardiotoxicity can manifest as cardiomyopathy,
congestive heart failure, ischemia, arrhythmias, or
hypertension. Anthracyclines are well recognized
as the agents that cause cardiomyopathies and
congestive heart failure when certain cumulative
doses of the anthracycline have been reached.
Uma complicação rara, mas grave, com alguns
agentes quimioterápicos é a cardiotoxicidade. A
cardiotoxicidade pode se manifestar como
cardiomiopatia, insuficiência cardíaca congestiva,
isquemia, arritmias ou hipertensão. As antraciclinas
são bem reconhecidas como agentes que causam
cardiomiopatias e insuficiência cardíaca congestiva
quando certas doses cumulativas de antraciclina
são atingidas.
Neurotoxic effects of chemotherapy occur fairly
frequently and are often reasons to limit the dose or
delay therapy. Some agents cause both central and
peripheral neurotoxicity. For example, high-dose
cytarabine, ifosfamide, and nelarabine are
commonly known for their central neurotoxic side
effects.
Os efeitos neurotóxicos da quimioterapia ocorrem
com bastante frequência e, muitas vezes, são
razões para limitar a dose ou adiar a terapia. Alguns
agentes causam neurotoxicidade central e
periférica. Por exemplo, altas doses de citarabina,
ifosfamida e nelarabina são bastante conhecidas
pelos seus efeitos colaterais neurotóxicos do
sistema nervoso central.
– Anthracyclines, interferon
• Ischemia
– Fluorouracil, sorafenib
• Arryhthmias
– Anthracyclines, arsenic, taxanes
• Hypertension
– Bevacizumab, sorafenib
Treatment Modalities:
Drug Therapy Part II
Neurotoxicity
• Cerebellar toxicity
– Ataxia, nystagmus, gait and coordination abnormalities
– High dose cytarabine (> 1 gm/m2)
• Encephalopathy
– Confusion, aphasia, headache
– Methotrexate, ifosfamide
• Arachnoiditis
– Headache, nausea/vomiting, fever, photophobia
– Intrathecal methotrexate and cytarabine
• Seizures
– Nelarabine
13
Treatment Modalities:
Drug Therapy Part II
Neurotoxicity (continued)
• Peripheral neuropathy
– Manifest as stocking-glove like distribution,
pain, tingling
– Vinca Alkaloids
• Vincristine
Chemotherapy can also induce peripheral
neuropathy that is related to the cumulative dose
and the type of drug used. The vinca alkaloids, the
platinum analogs, and the taxanes are notorious for
inducing peripheral neuropathy. The early signs
and symptoms are pain or tingling in the hands and
feet and sometimes loss of reflexes. And this is
usually a reason for delaying or reducing the dose
of the next cycle.
A quimioterapia também pode induzir a neuropatia
periférica relacionada à dose cumulativa e ao tipo
de fármaco utilizado. Os alcaloides da vinca, os
análogos da platina e os taxanos são conhecidos
por induzirem a neuropatia periférica. Os sinais e
sintomas precoces são dor ou formigamento nas
mãos e nos pés e, às vezes, perda dos reflexos. E,
geralmente, isso é razão para adiar ou reduzir a
dose no próximo ciclo.
And some --- additional neurotoxic effects can
involve the bowel system, the eyes, and the ears.
E outros efeitos neurotóxicos podem afetar o
sistema intestinal, os olhos e os ouvidos.
– Platinum Analogs
• Cisplatin and oxaliplatin
– Taxanes
• Paclitaxel > Docetaxel
Treatment Modalities:
Drug Therapy Part II
Neurotoxicity (continued)
• Constipation, Bowel obstructions
– Vinca alkaloids, cisplatin
• Ocular Toxicity
– Chemical conjuctivitis
– High dose cytarabine
• Ototoxicity
– Loss of high frequency ranges,
acute tinnitus, chronic hearing loss
– Cisplatin
14
Treatment Modalities:
Drug Therapy Part II
Hepatotoxicity
• Hepatotoxicity manifests in a variety of patterns
–
–
–
–
Hepatocellular necrosis - acute toxicity
Cholestasis - impaired flow of bile from liver to duodenum
Steatosis - fatty liver
Veno-occlusive disease (VOD) - injury to hepatic venous
endothelium
• Hepatocellular injury is generally reversible and nonfatal
• Many drugs require dose reduction or avoidance in the
setting of hepatic insufficiency
• Hepatotoxic agents include: vinca alkaloids, cytarabine,
methotrexate, clofarabine, gemtuzumab, imatinib,
L-asparaginase
Treatment Modalities:
Drug Therapy Part II
Nephrotoxicity
• Chemotherapy can impair kidney function
• Impairment can range from asymptomatic elevations
of serum creatinine to renal failure requiring dialysis
– Methotrexate and cisplatin are well-known nephrotoxins
Chemotherapy can also cause hepatotoxicity that
can manifest as elevated liver function tests,
cholestasis, and veno-occlusive disease, which is
injury to the hepatic venous endothelium. Many of
these drugs are cleared through the liver, hence, will
require dose adjustment in the setting of
hepatocellular injury or reduced liver function. I’ve
provided a list of drugs that are typically hepatotoxic
or hepatically-cleared agents.
Some of them
include vinca alkaloids, cytarabine, methotrexate,
clofarabine, imatinib, and L-asparaginase.
A
quimioterapia
também
pode
causar
hepatotoxicidade que se manifesta como resultados
elevados dos exames de função hepática, colestase
e doença veno-oclusiva, que é a lesão do endotélio
venoso hepático. Muitos desses medicamentos são
metabolizados pelo fígado. Por conseguinte, haverá
necessidade de ajustar a dose quando de lesões
hepatocelulares ou redução da função hepática.
Relacionei uma lista de fármacos que são
caracteristicamente
hepatotóxicos
ou
metabolizados pelo fígado. Alguns deles incluem:
alcaloides da vinca, citarabina, metotrexato,
clofarabina, imatinibe e L-asparaginases.
And you cannot forget about nephrotoxicity. Many
of the chemotherapy agents are renally cleared
through the kidneys. Two common agents are
methotrexate and cisplatin. They are both renally
eliminated and cause --- can cause renal
insufficiency or renal failure. Impaired renal function
can increase systemic toxicities. Hence many drugs
require dose reduction or avoidance in the setting of
renal insufficiency.
E não podem esquecer a nefrotoxicidade. Muitos
dos agentes quimioterápicos são metabolizados
pelos rins. Dois agentes comuns são o metotrexato
e a cisplatina. Ambos são eliminados pelos rins e
causam... podem causar insuficiência renal. O
comprometimento da função renal pode aumentar
as toxicidades sistêmicas. Por isso, em caso de
insuficiência renal, é necessário reduzir a dose de
alguns fármacos ou evitá-los.
• Impaired renal function can increase systemic
toxicities
• Many drugs require dose reduction or avoidance in
the setting of renal insufficiency
– Cytarabine, methotrexate, cisplatin, carboplatin, etoposide
15
Treatment Modalities:
Drug Therapy Part II
Dermatologic Toxicity
Treatment Modalities:
Drug Therapy Part II
Myelotoxicity
• Neutropenia
– Decrease in the number of circulating neutrophils
– Single most important predisposing factor to infection
• Anemia
– Decrease in hemoglobin or circulating erythrocytes
• Thrombocytopenia
– Decrease in the number of circulating platelets
It is not surprising that some of these medications
cause problems with the skin. The good news is
that many of these agents --- many of these
problems are reversible. Hair loss is a common
side effect of some of these agents. Extravasation
occurs when the drug leaks through the tubing into
the skin and causes skin necrosis. Occasionally,
this may require surgical intervention. Interesting --interestingly, some targeted therapies cause acnelike rash on the face, trunk, and extremities.
Não é estranho que alguns desses medicamentos
causem problemas na pele. A boa notícia é que
muitos desses agentes... muitos desses problemas
são reversíveis. A perda de cabelo é um efeito
colateral comum de alguns desses agentes. O
extravasamento ocorre quando o fármaco se infiltra
na pele através dos vasos e causa sua necrose. Às
vezes, para isso é necessário uma intervenção
cirúrgica. Curiosamente, algumas terapias alvo
causam erupção cutânea tipo acne no rosto, tronco
e membros.
Adverse effects on the bone marrow production
called myelosuppression is a serious toxicity that
can manifest as neutropenia, anemia, or
thrombocytopenia.
Myelosuppression is often
dictated by the dose, schedule, and type of agent
being used. Patient characteristics as well, the age,
renal function, liver function, etc., can affect the
dosing and the toxicity of these drugs. Neutropenia
is a very serious side effect due to the risk of
infection.
Febrile neutropenia often requires
hospitalization and IV antibiotics. Anemia is --often causes fatigue and thrombocytopenia,
increases your risk for bleeding.
These
complications can be thwarted by transfusions.
Efeitos adversos na produção da medula óssea,
denominada mielossupressão, é uma toxicidade
grave que pode se manifestar como neutropenia,
anemia ou trombocitopenia. Muitas vezes, a
mielossupressão é ditada pela dose, o horário [das
doses] e o tipo de agente utilizado. As
características do paciente, bem como a idade, a
função renal, etc., podem afetar a dose e a
toxicidade desses fármacos. A neutropenia é um
efeito colateral muito grave por causa do risco de
infecção. Frequentemente, a neutropenia febril
exige hospitalização e antibióticos por via IV. Muitas
vezes, a anemia causa fadiga e trombocitopenia e
aumenta
o
risco
de
hemorragia.
Estas
complicações
podem
ser
impedidas
por
transfusões.
16
Treatment Modalities:
Drug Therapy Part II
Dosing and Toxicity Summary
• Drug therapy can affect any organ system in
the body
• Factors that influence treatment toxicity may
include drug dose, organ function, age and method
of administration
So, in summary of dosing and toxicity, drugs can
affect any organ system in the body. And factors
that often influence treatment toxicity can include
the drug, the drug dose, organ function, age, and
method of administration.
And monitoring and
management of drug-induced toxicity requires a
multidisciplinary approach.
Resumindo, quanto à dose e toxicidade, os
fármacos podem afetar qualquer sistema de órgãos
do corpo. E os fatores que muitas vezes influenciam
a toxicidade do tratamento podem abranger o
fármaco, a dose do fármaco, a função do órgão, a
idade e o método de administração. Além disso, o
monitoramento e o tratamento da toxicidade
induzida por fármacos exigem uma abordagem
multidisciplinar.
In summary, the purpose of chemotherapy may vary
depending on patient-specific factors, such as age,
comorbidity, tumor stage, and type of malignancies.
The mainstay of oncology therapy still involves
cytotoxic agents that indiscriminately kill rapidly
dividing cells.
Novel therapies, such as
immunotherapy and targeted therapy, targets tumorspecific molecules and processes while hopefully
preserving normal tissue. Often targeted therapy is
combined with conventional chemotherapy.
Em resumo, o objetivo da quimioterapia pode variar
dependendo de fatores específicos do paciente,
como idade, comorbidade, estágio do tumor e tipo
de câncer. O principal suporte da terapia oncológica
ainda implica o uso de agentes citotóxicos que
destroem indiscriminadamente as células que se
dividem rapidamente. Terapias originais, como
imunoterapia e terapia alvo, são dirigidas a
moléculas e processos específicos do tumor e, ao
mesmo tempo, preservam o tecido normal. Muitas
vezes, a terapia alvo é combinada com a
quimioterapia convencional.
• Monitoring and management of drug-induced toxicity
plays an important role in caring for cancer patients
Treatment Modalities:
Drug Therapy Part II
Conclusions
• Drug therapy may be used for various goals in
cancer treatment depending on a patient’s disease
and prognosis
• Chemotherapy drugs are classified by mechanisms
of action and differ in cytotoxic mechanisms of action
• Newer immune-based and targeted therapies are
emerging and serve an important role in cancer
care
• Drug therapy may result in a wide variety
of side effects
17
Treatment Modalities:
Drug Therapy Part II
Cancer Resources
And lastly, I would like to leave you with this slide
with a list of resources for additional cancer and
chemotherapy information.
I hope you have
enjoyed this lecture and we welcome your feedback.
Thank you.
E, finalmente, gostaria de terminar com este slide
que mostra uma lista de recursos com mais
informações sobre câncer e quimioterapia. Espero
que tenham gostado da apresentação e
agradeceríamos suas opiniões e comentários.
Obrigado.
18