UNIVERSIDADE FEDERAL DO ABC
Curso de Pós-Graduação em Biossistemas
Dissertação de Mestrado
Claudia Januário dos Santos
INVESTIGAÇÃO DA PRESENÇA DO CITOMEGALOVÍRUS HUMANO EM
LESÕES TUMORAIS E SANGUE PERIFÉRICO DE PACIENTES COM
GLIOBLASTOMA MULTIFORME
Santo André
2014
Curso de Pós-Graduação em Biossistemas
Dissertação de Mestrado
Claudia Januário dos Santos
INVESTIGAÇÃO DA PRESENÇA DO CITOMEGALOVÍRUS HUMANO EM
LESÕES TUMORAIS E SANGUE PERIFÉRICO DE PACIENTES COM
GLIOBLASTOMA MULTIFORME
Trabalho apresentado como requisito parcial
para obtenção do título de Mestre em
Biossistemas, sob orientação do Professora Doutora
Maria Cristina Carlan da Silva.
Santo André
2014
Nada na vida deve ser temido, somente compreendido. Agora é hora de compreender mais
para temer menos.
Marie Curie
Dedicatória
Aos meus avôs, José Januário e Eli Correia dos Santos, que foram, sem saber, os primeiros
cientistas que eu conheci.
Agradecimentos
Agradeço a minha orientadora, agora de longa data, Profª Drª Maria Cristina Carlan da
Silva, por todo apoio e paciência durante todos esses anos (e pelos próximos por vir).
As agências de fomento FAPESP pela verba disponibilizada para a realização do
trabalho e UFABC e CAPES pela bolsa de mestrado.
Aos doutores Eberval Gadelha Figueiredo, Clemar Corrêa, Manoel Jacobsen Teixeira,
Hector Navarro Cabrera e Matheus Schmidt Soares pela colaboração no trabalho quanto a
parte cirúrgica e disponibilização das amostras.
As professoras Ana Carolina e Márcia Sperança pela ajuda antes e durante a
qualificação.
Aos meus colegas de laboratório, tanto novos quanto já formados por aqui: Lucas,
Fabi, Aquiles, Grazi, Lívia, Aninha, Ed.
Aos colegas dos outros laboratórios, que só Deus sabe o quanto tiveram que me
aguentar esse tempo: Karina, Renan, Mayra, Michelle e Kelly.
Aos meus amigos de hoje e sempre, aqueles para os quais eu sempre corria quando
algo dava errado no laboratório (e fora dele): Camila, Leo e Thaís.
Aos meus amigos de longa e curta data: Luan, Pedro, Íris, Julia, Fabi, Gi, Jéssica,
Daia, Mayra, João e Gabriel.
As minhas pequenas irmãs de coração: Hevelin, Ana, Camila, Silene, Thaís.
As minhas famílias, Januário e Santos.
A Erik, pela infindável paciência, carinho, respeito e amor dedicados a mim (mesmo
quando eu não merecia).
E
principalmente,
mãe
e
pai,
por
sempre
acreditarem
em
mim.
Lista de figuras
Figura 1: Estrutura do HCMV. Microscopia eletrônica do HCMV (esquerda) e
desenho esquemático do mesmo (direita). Na imagem são identificadas as regiões do
envelope (com gliocoproteínas de superfície), tegumento e capsídeo icosaédrico (com
DNA dupla fita de 235kb, com aproximadamente 192 ORFs).
Figura 2: Esquema do DNA viral do HCMV. Esquema do genoma do HCMV, com
regiões UL e US, flanqueadas pelas regiões TRL e IRL, IRS e TRS, respectivamente.
Figura 3: Esquema da replicação do HCMV. Inicialmente a partícula viral liga-se a
receptores celulares através das glicoproteínas de envelope, fusionando-se com a
membrana plasmática, e liberando o capsídeo e proteínas/RNAs virais no citoplasma
celular. O capsídeo é então deslocado até o núcleo onde o DNA viral é liberado através
dos poros e inicia-se a expressão dos genes virais. Os genes primeiramente expressos
são os IE (prevalentemente fatores de transcrição), seguidos pelos E (envolvidos na
replicação viral) e por fim os L (responsáveis pela formação de proteínas estruturais, do
capsídeo, do tegumento e envelope). O DNA viral é então empacotado no
nucleocapsídeo no núcleo celular e transportado para o citoplasma, onde adquire o
envelope final em membranas do Retículo Endoplasmático/Complexo de Golgi, onde
estão as glicoproteínas de tegumento. A partícula completa é liberada por exocitose.
Figura 4: Imagem de ressonância magnética de cérebro com Glioblastoma
Multiforme. A imagem axial em (A) o círculo apontado pela seta indica a região
central do tumor (necrose) circundada por um padrão de anel. (B) Imagem axial T2 do
mesmo tumor, a seta indica região periférica a zona necrótica com células tumorais
infiltrativas e edema vasogênico (Adaptado de Rong & Brat, 2009).
Figura 5: Ativação da pró-droga TMZ. Em pH ~7.4 ocorre abertura do anel de 6
membros produzindo o intermediário MTIC. O MTIC ativo libera metildiazônio que
metila o DNA liberando N2 altamente estável. Cerca de 70%, 10% e 5% dos grupos
metil transferidos para o DNA estão em sítio N7-guanina, N3-adenina e O6-guanina,
respectivamente (adaptado de Ramirez et al, 2013).
iv
Figura 6: Limite de detecção de HCMV obtido por nPCR e qPCR. (a) Eletroforese
em gel de agarose 1,5% dos produtos de amplificação obtidos por nPCR e (b) Curvas de
amplificação dos produtos obtidos por qPCR. Em ambos os casos os limites de detecção
foram determinados amplificação de diluições seriadas de 10x do HCMV FIX-BAC de
concentrações conhecidas adicionadas a DNA genômico (extraído de sangue de
paciente HCMV negativo). Em ambos os casos, o gene GAPDH foi amplificado como
controle da presença de DNA celular (dados não mostrados). Os melhores limites de
detecção obtidos foram de 9 cópias/µl por nPCR (gene UL55) e 2 cópias/µl por qPCR
(gene UL83).
Figura 7: Detecção do HCMV por nPCR em amostras de sangue e tumor de
pacientes com tumores cerebrais.. Eletroforese em gel de agarose 1,5% dos produtos
obtidos a partir da amplificação do DNA extraído de amostras de tumores (A) e de
sangue (B), amplificados utilizando-se primers para a região variável do gene que
codifica a proteína gB (316 pb) do HCMV. O fragmento do gene GAPDH (203 pb) foi
amplificado como controle celular, verificando-se assim a presença de DNA genômico.
H2O foi utilizada como controle negativo. P01 à P22 referem-se a pacientes com GBM
e OT a outros tumores que não GBMs (não incluídos neste estudo).
Figura 8: Detecção do HCMV por qPCR em amostras de tumor de pacientes com
tumores cerebrais. Curvas de amplificação obtidas por qPCR de amostras de tumor
extraído de amostras de tumores utilizando-se de primers para as regiões pp65 do
HCMV (a) e o gene celular GAPDH (b). Nestas curvas cada cor representa um diferente
paciente.
Figura 9: Quantificação de DNA viral do HCMV por qPCR em amostras de
tumores e sangue periférico de pacientes com GBM. (a) Vinte e duas amostras de
tecido tumoral foram analisadas por qPCR utilizando-se de primers para a região do
gene que codifica a proteína viral pp65 e para o gene celular GAPDH. A relação entre o
DNA celular e o DNA viral é expressa como log10. (b) Nove e oito amostras de sangue
provenientes de pacientes com GBM e transplantados renais, respectivamente foram
analisadoa por qPCR para a região viral pp65. A carga viral é expressa em número de
cópias do vírus/ml.
v
Lista de tabelas
Tabela 1. Frequência da detecção de HCMV por qPCR (gene UL83) e nPCR (gene
UL55) e correlação da positividade nas amostras de sangue e tumor de pacientes com
GBM.
Tabela 2: Frequência do genótipo de gB nas amostras de tumor e sangue periférico de
pacientes com GBM.
vi
Lista de abreviaturas e siglas
aa - Aminoácidos
AIDS (“Acquired Immunodeficiency Syndrome”) - Síndrome da imunodeficiência
adquirida
ATL (“Adult T-cell leukemia”) - Leucemia de células T
BBB (“Blood–brain-barrier”) - Barreira hemato-encefálica
BCNU - Carmustina
BL (“Burkitt's lymphoma”) – Linfoma de Burkitt
BLAST (“Basic Local Alignment Search Tool”) - Ferramenta de procura de
alinhamento local básica
BTB (“Blood–tumor-barrier”) - Barreira encéfalo-tumoral
cPCR (“Conventional PCR”)– PCR convencional
DMBT1 (“Deleted in malignant brain tumors 1 protein”) – Proteína deletada em
tumores malignos de cérebro.
DNA (“Deoxyribonucleic acid”) – Ácido Desoxirribonucleico
dNTPs (“Deoxyribonucleotid”) – Dexoxirribonucleotídeo
dsDNA (“Double strand DNA”) - DNA dupla fita
E (“Early”) –Genes precoces
EBV (“Epstein-Barr Virus”) - Vírus Epstein-Barr
EGRF (“Epidermal growth factor receptor”) - Receptor do fator de crescimento
epidérmico
FDA-EUA (“Food and Drug Administration”) – Agência americana de fiscalização de
alimentos e drogas.
vii
GAPDH (“Glyceraldehyde 3-Phosphate Dehydrogenase”) - Gliceraldeído 3-Fosfato
Desidrogenase
gB – Glicoproteína B
GBM – Glioblastoma
gH – Glicoproteína H
gL – Glicoproteína L
gM - Glicoproteína M
gN- Glicoproteína N
gO – Glicoproteína O
GPCR (“G-protein-coupled receptor”) - Receptor viral acoplado a proteína G
HAART (“Antiretroviral Therapy”) - Terapia Antiretroviral Altamente Ativa
HBV (“Hepatitis B Virus”) - Vírus da Hepatite B
HCMV (“Human Cytomegalovirus”) – Citomegalovírus Humano
HCMV FIX-BAC – Linhagem clínica FIX do HCMV clonado como Cromossomo
Bacteriano Artificial
HCV (“Hepatitis C Virus”)- Vírus da Hepatite C
HE - Hematoxilina e Eosina
HHV-6 (“Human Herpesvirus 6”)- Herpesvírus humano 6
HHV-7 (“Human Herpesvirus 7”)- Herpesvírus humano 7
HIV (“Human immunodeficiency virus”) - Vírus da imunodeficiência humana
HPV (“Human Papillomavirus”)- Papilomavírus Humano
HPV16 (“Human Papillomavirus 16”)- Papilomavírus Humano 16
HPV18 (“Human Papillomavirus 18”)- Papilomavírus Humano 18
viii
HTLV-1 (“Human T lymphotropic virus type 1”) - Vírus Linfotrópico de células T
humano tipo 1
IARC (“International Agency for Research on Cancer”) – Agência Internacional de
Pesquisa em câncer
IE (“Immediate-early”)– Genes imediatamente precoces
IE1 ou IE1-72 (“Immediate-early Protein 1”)– Proteína imediatamente precoce 1
IE2 ou IE2-86 (“Immediate-early Protein 2 ”) – Proteína imediatamente precoce 2
IHC (“Immunohistochemistry”) – Imunohistoquímica
INK4a – Inibidor 2A dependente de ciclina-quinase
INK4b - Inibidor 2A dependente de ciclina-quinase
IRL (“Internal reapet long”) - Seqüência interna repetida longa
IRS (“Internal reapet short”) - Seqüência interna repetida curta
ISH (“In situ hybridization”) – Hibridização in situ
kb (“kilobase”) – quilobase
kD (“kiloDalton”) – quilo Dalton
KS (“Kaposi's sarcoma”) – Sarcoma de Kaposi
KSHV (“Kaposi's sarcoma-associated herpesvirus”)- Herpesvírus associado ao
Sarcoma de Kaposi
L (“late”)-Genes tardios
LB - Lysogeny broth
MCP (“major capsid protein”) - Proteína maior do capsídeo
MCPγV (“Merkel cell polyomavirus”)- Poliomavírus de células Merkel
MIE (“major IE”) – região maior de IE
ix
MTIC (“open-chain triazene”) – Triazeno de cadeia aberta
mRNA (“messengers RNAs”) – RNAs mensageiros
mTOR (“mammalian target of rapamycin”) - Alvo mamífero da rapamicina
NCBI-USA (National Center for Biotechnology Information)- Centro Nacional para
Informalção em Biotecnologia dos Estados Unidos da América
nPCR – semi-nested PCR
nm – nanometros
ORFs (“open reading frames”) – Fases abertas de leitura
p15 – Proteína 15kDa
p16 – Proteína 16kDa
p53 – Proteína 53 kDa
p107 – Proteína 107kDa
p130 - Proteína 130 kDa
pp28 – Fosfoproteína 28 kDa
pp65 – Fosfoproteína 65 kDa
pp71 – Fosfoproteína 71 kDa
pp150 – Fosfoproteína 150 kDa
PCR (“Polymerase chain reaction”) – Reação em cadeia da polimerase
PDGF (“platelet-derived growth factor”) - Fator de crescimento derivado de plaquetas
PDGFR (“platelet-derived growth factor receptor”)- Receptor do fator de crescimento
derivado de plaquetas
pH – potencial hidrogeniônico
PORT (“portal protein”) - Proteína portal
ppUL48- Fosfoproteína UL48
x
pRb – Proteína retinoblastoma
PTEN (“Phosphatase and tensin homolog”)- Homólogo de fosfatase e tensina
pUL83 – Proteína UL83
pUS28 – Proteína US28
qPRC – PCR quantitativo em tempo real
RNA (“Ribonucleic acid”) - Ácido Ribonucleico
SCP (“smallest capsid protein ”) - Menor proteína do capsídeo
SNC – Sistema Nervoso Central
SSDNA IQUSP - Serviço de Sequenciamento de DNA do Instituto de Químicada
Universidade de São Paulo
TE – tampão Tris EDTA
TRI2 (“minor capsid protein”) - Proteína menor do capsídeo
TRL ( “terminal repeat long”) - Seqüência terminal repetida longa
TRL-2 (“Toll-like receptor 2”) - Receptor como Toll 2
TRS (“terminal repeat short”) - Seqüência terminal repetida curta
TMZ - Temozolamida
UFABC – Universidade Federal do ABC
UL (“unique long”) – Sequência única Longa
US (“unique short”) – Sequência única Curta
xi
Resumo
Glioblastoma multiforme (GBM) é o tumor mais prevalente e maligno do sistema
nervosa central. Nos últimos anos, evidências sugeriram uma associação entre a
infecção pelo citomegalovírus humano (HCMV) e o glioblastoma multiforme. Neste
estudo, amostras de tumor e sangue periférico de pacientes com GBM foram
examinadas quanto a presença do DNA do HCMV. Vinte e duas amostras tumorais
provenientes de biópsisas e 20 amostras de sangue periférico foram analisadas por PCR
em tempo real (qPCR) e semi-nested PCR (nPCR) para a presença das regiões
genômicas virais pp65 e glicoproteína B (gB), respectivamente.DNA do HCMV foi
detectado na maioria das amostras de tumor analisadas (95% por qPCR e 91% por
nPCR). Cerca de metade dos pacientes com tumores positivos para HCMV também
tiveram DNA viral detectável em seu sangue periférico (47% por qPCR e 61% por
nPCR). O número de cópias foi também determinado e na maioria das amostras de
tumor o DNA celular está presente em número muito maior que o DNA viral (média de
1 célula infectada a cada 33 células. O genótipo gB foi determinado nas amostras
positivas para HCMV, sendo o genótipo gB2 o mais prevalente nas amostras de sangue
e tumor. Os resultados mostram uma alta prevalência do HCMV em amostras de GBM,
reforçando a possível associação entre a infecção do HCMV e o desenvolvimento do
tumor.
xii
Abstract
Glioblastoma multiforme is the most prevalent and malignant tumor of the central
nervous system. In the last few years, accumulating evidence has suggested an
association between human cytomegalovirus (HCMV) infection and glioblastoma
multiforme. In this study, tumor tissues and peripheral blood of patients with
glioblastoma multiforme were examined for the presence of HCMV DNA. Twenty-two
fresh surgical brain specimens and 20 peripheral blood samples were analyzed by realtime PCR (qPCR) and hemi-nested PCR (nPCR) for the presence of pp65 and
(glycoprotein B) gB viral genomic regions, respectively. HCMV DNA was detected in
the majority of the tumor samples analyzed (95% by qPCR and 91% by nPCR). About
half of the patients with tumors positive for HCMV also had detectable viral DNA in
their peripheral blood (47% by qPCR and 61% by nPCR). Genome copy numbers were
determined and in the majority of the tumor samples cellular DNA outnumbers viral
DNA (average of 1 infected cell in 33 cells). The gB genotypes were determined in
HCMV-positive samples and gB2 was the most prevalent genotype in the tumor and
blood samples. The results show a high prevalence of HCMV in glioblastoma
multiforme samples reinforcing a possible association between HCMV infection and
tumor development.
xiii
Índice
Introdução ..................................................................................................................................... 2
Vírus e câncer ............................................................................................................................ 2
Citomegalovírus Humano (HCMV) .......................................................................................... 4
Histórico do HCMV e câncer .................................................................................................. 11
Glioblastoma ........................................................................................................................... 12
HCMV e glioblastoma ............................................................................................................ 15
Possíveis mecanismos moleculares de indução da oncomodulação pelo HCMV ................... 16
Objetivo ....................................................................................................................................... 18
Materiais e Métodos .................................................................................................................... 19
Amostras Clínicas ................................................................................................................... 19
Extração de DNA .................................................................................................................... 19
DNA viral ................................................................................................................................ 19
PCR qualitativo ....................................................................................................................... 20
PCR em tempo real quantitativo. ............................................................................................ 20
semi-nested PCR e caracterização dos genótipos da glicoproteína gB. .................................. 20
Determinação dos genótipos nas amostras de sangue e tumor. ............................................... 21
Determinação dos limites de detecção do DNA viral e quantificação de DNA genômico. .... 21
Resultados ................................................................................................................................... 23
Cálculo do limite de detecção do DNA viral da pelas técnicas de cPCR, qPCR nPCR.......... 23
Detecção do genoma viral nas amostras de tumores e sangue de pacientes com GBM .......... 25
Determinação e correlação entre genótipos de gB em amostras de sangue periférico e tumores
de pacientes com GBM. .......................................................................................................... 29
Discussão..................................................................................................................................... 32
Conclusão .................................................................................................................................... 36
Referências .................................................................................................................................. 37
Anexos......................................................................................................................................... 55
Sequências obtidas durante o trabalho .................................................................................... 55
Apêndice ..................................................................................................................................... 63
Resumos apresentados em Congressos ................................................................................... 63
Artigo publicado em revista científica .................................................................................... 67
Introdução
Vírus e câncer
Evidências crescentes mostram que agentes infecciosos são causas frequentes de
cânceres em humanos. Segundo dados da Agência Internacional para a Pesquisa no
Câncer (IARC, do inglês International Agency for Research on Cancer) cerca de 20%
de todos os casos de câncer registrados no mundo são causados por infecções, sendo a
maioria de origem viral (Moore & Chang, 2010). A presença de vírus em tumores, com
ou sem expressão gênica, pode levar a: perda de controle do ciclo celular, inibição de
supressores de crescimento, indução de angiogênese, prevenção de apoptose,
imortalidade celular, dentre outros. Todas essas anormalidades são também conhecidas
como hallmarks do câncer: fatores que podem levar uma célula normal a um estado
tumoral (Hanahan & Weinberg, 2011). Os vírus mais comumente associados a
carcinogênese são o Vírus Epstein-Barr (EBV), o Vírus da Hepatite B (HBV), o
Papilomavírus Humano (HPV), o Vírus Linfotrópico de células T Humano (HTLV-1), o
Vírus da Hepatite C (HCV), o Vírus Associado ao Sarcoma de Kaposi (KSHV) e o
Poliomavírus de Células Merkel (MCPγV) (Bergonzini, Salata, Calistri, Parolin, &
Palù, 2010).
Em 1964, Epstein, Barr e colaboradores, localizaram a partir de estudos em
microscopia eletrônica, partículas virais similares a de herpervírus em uma linhagem
celular de Linfoma de Burkitt (BL, do inglês “Burkitt's lymphoma”) (Epstein, M. A.,
Achong, B. G. & Barr, 1964). O vírus identificado foi denominado Vírus Epstein-Barr
(EBV). Estudos posteriores mostraram que a infecção por EBV estava associada com
carcinoma nasofaringeal, linfomas pós-transplantacionais e alguns linfomas de
Hodgkin. (Bergonzini et al., 2010).
Em 1975, Blumberg et al, correlacionaram a infecção crônica por HBV com
carcinoma hepatocelular, um dos cânceres mais comuns no mundo (Blumberg et al.,
1975). O HBV foi o primeiro vírus cuja vacina foi produzida, vacina esta, que previne
além da hepatite aguda o desenvolvimento do hepatocarcinoma celular (Chang MH,
Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS, Liang DC & DS, 1997; Hilleman,
2003).
Em 1976, Harald zur Hausen propôs que o Papilomavírus Humano (HPV)
poderia ser o agente etiológico do carcinona cervical (Zur Hausen, 1976), especialmente
2
no que se trata aos tipos HPV16 e HPV18 (Boshartb et al., 1984; Dürst, Gissmann,
Ikenberg, & zur Hausen, 1983). Hoje se sabe que este dois tipos de HPV são
responsáveis por quase todos os tipos de cânceres cervicais, sendo a terceira causa de
morte correlacionada a cânceres em mulheres no mundo inteiro (Zur Hausen, 2002).
Poiesz, Gallo et al, 1980 mostraram que em culturas celulares provenientes de
linfomas de células T ocorria atividade de transcrição reversa (transcriptase reversa) e
produção de partículas retrovirais imunologicamente distintas de outras partículas
conhecidas (Poiesz et al., 1980). Este novo vírus, denominado HTLV-1, foi identificado
um ano mais tarde em linhagens celulares provenientes de pacientes com leucemia de
células T (ATL, do inglês “adult T-cell leukemia”). Além disso, observou-se que
anticorpos contra partículas de HTLV-1 eram produzidos somente em pacientes
portadores de ATL, e não em pacientes controles (pacientes com tumores diferentes de
ATL), sugerindo que o vírus era o agente etiológico deste tipo de tumor (Hinuma et al.,
1981).
Em 1989, Choo e colaboradores demostraram que um novo vírus, denominado
Vírus da Hepatite C (HCV), era o agente etiológico de hepatite pós-transfusional (não
causada por HBV). Este estudo também demonstrou uma associação entre o
Hepatocarcinoma crônico e a infecção por HCV (Choo et al., 1989; Colombo et al.,
1989; Tan, Yeh, Liu, Cheung, & Chen, 2008).
Em 1994, estudos visando à associação entre o risco de desenvolvimento do
Sarcoma de Kaposi (KS) em pacientes com a Síndrome da Imunodeficiência Adquirida
(AIDS, do inglês Acquired Immunodeficiency Syndrome) levaram ao descobrimento do
Vírus do Sarcoma de Kaposi (KSV). Estudos posteriores mostraram a correlação entre o
desenvolvimento do KS e a presença do KSHV(Bergonzini et al., 2010).
O mais recente vírus tumoral detectado foi um novo tipo de poliomavírus, o
MCPγV (do inglês, Merkel Cell Polyomavirus), isolado de amostras de pacientes com
um tipo de carcinoma de pele altamente agressivo, chamado de carcinoma de células
Merkel (Feng H, Shuda M, Chang Y, 2008; zur Hausen, 2008).
Ao longo dos anos estudos demonstraram que estes vírus estão intimamente
relacionados ao desenvolvimento do fenótipo tumoral maligno. No entanto, mesmo
vírus
não considerados oncogênicos (iniciadores de tumor) podem alterar eventos
moleculares celulares e potencialmente contribuir para a progressão do tumor ou
malignidade, sendo o Citomegalovírus Humano (HCMV) considerado um destes vírus.
3
Citomegalovírus Humano (HCMV)
O HCMV, também conhecido como Herpesvírus Humano-5 (HHV-5) pertence à
família Herpesviridae, subfamília -herpesvirinae, juntamente com o HHV-6 e o HHV7 (Mockarsi et al, 2006). O HCMV é um agente ubíquo de alta prevalência mundial,
com soropositividade variando de 40 a 70% em países desenvolvidos e 90% a 100% em
países em desenvolvimento (Mocarski, Shenk, & Pass, 2006). Como todos os
citomegalovírus, o HCMV é um vírus espécie específico.
A transmissão viral pode ocorrer verticalmente da mãe para o feto (ou recémnascido), ou horizontalmente de um indivíduo para outro. A transmissão vertical pode
ocorrer via intrauterina, na qual a infecção é o resultado de viremia materna. Já a
infecção perinatal ocorre geralmente devido ao contato com secreções genitais
infectadas durante o parto ou tardiamente via leite materno. A transmissão horizontal
corre frequentemente durante a infância via contato com fluídos corpóreos infectados,
sendo comum a transmissão via saliva ou urina de crianças infectadas para não
infectadas. Apesar de muito comum em crianças, este tipo de contaminação também
ocorre, em menor frequência, entre crianças infectadas para adultos saudáveis. Em
adultos, a maior rota de infecção é a transmissão sexual, seguida pela transmissão via
transfusão sanguínea e transplantes de órgãos e medula óssea.
A infecção primária por HCMV caracteriza-se por uma fase aguda de replicação
em vários tipos celulares (como células epiteliais, endoteliais, musculares e outros tipos
celulares). Nesta etapa o vírus é secretado na urina, saliva, sêmen e secreções cervicais
do hospedeiro, processo este que pode levar de semanas a meses. Após a infecção
primária ocorre uma fase de persistência, na qual o vírus se replica lentamente devido à
ativação do sistema imune e controle da replicação viral. Por fim, como todos os
herpesvírus, o HCMV fica em estado de latência por toda vida do indivíduo infectado,
estado este que se caracteriza pela presença do DNA viral no núcleo das células
infectadas, na forma de um epissomo, e ausência de replicação viral. O vírus latente
pode ser reativado por estímulos externos como câncer, imunodeficiência e estresse
(Sinclair & Sissons, 2006).
Em indivíduos inumocompetentes a infecção é geralmente assintomática, devido
a um equilíbrio entre o sistema imune e a replicação viral. No entanto, em pacientes
inumocomprometidos, ou naqueles em que o sistema inume não está completamente
desenvolvido o vírus pode causar graves doenças. Em pacientes transplantados, o
HCMV é um dos principais agentes responsáveis por morte, especialmente em
4
pacientes recipientes de órgãos sólidos (Mocarski et al., 2006). O vírus pode também
tornar-se letal em indivíduos com AIDS, pois apesar da Terapia Antiretroviral
Altamente Ativa contra o HIV (HAART, do inglês Antiretroviral Therapy), alguns
pacientes não respondem ou não tem acesso ao tratamento (Gilbert & Boivin, 2005).
Além disso, o vírus também é um grave problema de morbidade e mortalidade em
recém-nascidos: a transmissão vertical comumente afeta o sistema nervoso central e os
órgãos de percepção do feto, sendo o HCMV a principal causa de surdez em recém –
nascidos (Gaytant, Steegers, Semmekrot, Merkus, & Galama, 2002; Stagno & Whitley,
1985).
Atualmente existem quatro drogas anti-virais aprovadas pelo Food and Drug
Administration (FDA – EUA): ganciclovir, valganciclovir, cidofovir e foscarnet
(Komatsu, Pikis, Naeger, & Harrington, 2013) . No entanto, estas drogas são tóxicas e
não são recomendadas para uso em mulheres grávidas ou recém – nascidos. Além disso,
o uso prolongado em pacientes imunocomprometidos e transplantados pode levar a
resistência do vírus a estes medicamentos (Limaye, 2002). Apesar de todas as tentativas
ainda não existe uma vacina completamente eficaz contra o HCMV e, devido a sua
infecciosidade, o Instituto de Medicina e o Programa de Vacinação dos EUA
estabeleceu como prioritário o desenvolvimento de uma vacina contra o HCMV
(Limaye, 2002).
Quanto a sua estrutura, a partícula viral tem aproximadamente 250 nm e é
composta por um capsídeo icosaédrico, contendo uma dupla fita de DNA linear, envolto
por uma camada de proteínas e RNA virais, denominada tegumento, e por fim pelo
envelope contendo glicoproteínas (Figura 1). Estima-se que a partícula viral seja
composta de aproximadamente 59 proteínas estruturais e várias proteínas celulares
(Varnum, Streblow, & Monroe, 2004), além do DNA e RNA virais (Bresnahan &
Shenk, 2000; Greijer, van de Crommert, Stevens, & Middeldorp, 1999).
5
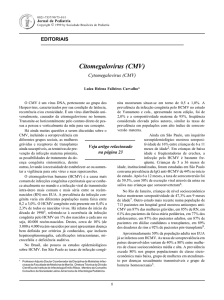
Figura 1: Estrutura do HCMV. Microscopia eletrônica (esquerda) e desenho
esquemático (direita) do HCMV. Na imagem são identificadas as regiões do envelope
(com glicoproteínas de superfície), tegumento e capsídeo icosaédrico (com DNA dupla
fita de 235kb, com aproximadamente 192 ORFs).
O genoma do HCMV, composto por um DNA de dupla fita linear com
aproximadamente 235 kbp, é formado por duas regiões únicas: a região única longa
(UL, do inglês, “unique long”) e uma região curta (US, do inglês, “unique short”). Estas
regiões são flanqueadas por seqüências terminais repetidas longas e curtas (TRL, do
inglês, “terminal repeat long” e TRS, “terminal repeat short”) e por seqüências internas
repetidas (IRL, do inglês, “internal repeat long” e IRS, “internal repeat short”) (Figura
2) (Mocarski et al., 2006). O genoma viral contém 192 fases abertas de leitura (ORFs,
do inglês “open reading frames” ) capazes de codificar cerca de 200 proteínas, muitas
com funções caracterizadas (Mocarski et al., 2006).
Figura 2: Esquema do DNA viral do HCMV. Esquema do genoma do HCMV, com
regiões UL e US, flanqueadas pelas regiões TRL e IRL, IRS e TRS, respectivamente.
6
O capsídeo viral é composto de cinco proteínas: proteína maior do capsídeo
(major capsid protein, MCP), proteína menor do capsídeo (minor capsid protein,
TRI1); proteína ligadora da proteína menor do capsídeo (minor capsid protein binding
protein, TRI2); menor proteína do capsídeo (smallest capsid protein, SCP) e a proteína
portal (portal protein, PORT).
O tegumento contém pelo menos 25 proteínas, em sua maioria fosforiladas. A
fosfoproteína básica (pp150) codificada pelo gene UL32 e a proteína menor de matriz
(pp65) codifica por UL83, são as proteínas mais abundantemente expressas durante a
replicação viral. Outras proteínas relevantes presentes no tegumento são ppUL99
(pp28), ppUL82 (pp71) e ppUL48. As proteínas de tegumento são importantes em
várias etapas da infecção viral, como liberação do capsídeo, liberação do DNA viral no
núcleo da célula, transativação dos genes virais, encapsidação do DNA, egresso do
capsídeo e envelopamento.
O envelope viral é formado por uma bicamada lipídica, derivada de membranas
do retículo endoplasmático e do complexo de Golgi, contendo proteínas virais e
celulares (Mocarski et al., 2006). As proteínas presentes no envelope são geralmente
glicosiladas, sendo as mais importantes as glicoproteínas gB, gH, gL, gO, gM e gN,
codificadas pelos genes virais UL55, UL75, UL155, UL74, UL100 e UL73,
respectivamente. Algumas destas proteínas ligam-se a receptores celulares como:
complexos de gB ligam-se a heparan sulfato, ao Receptor do Fator de Crescimento
Epidérmico (EGRF, do inglês “Epidermal growth factor receptor”), a integrinas a ao
Receptor tipo Toll 2 (TRL-2, do inglês “Toll-like receptor 2”); complexos de gM:gN
ligam-se a heparan sulfato e a integrinas e o complexo de gH:gL se liga a EGRF. Estas
interações possuem papel na fusão do vírus com a célula hospedeira, além da ativação
de diversas vias de sinalização intracelular na célula hospedeira.
A glicoproteína gB é um dos componentes essenciais do vírus (Isaacson &
Compton, 2009), produzida como um precursor de 160 kD que é clivado pela protease
furina durante seu transporte através da via exocítica, gerando duas moléculas, uma de
116kD e outra de 55kD, presentes no envelope viral como um complexo ligado por
ligações dissulfeto (Britt & Auger, 1986). O gene da gB é altamente variável em seu
sítio de clivagem (aminoácidos 460 a 461) e de acordo com sua variação na sequência
linhagens de HCMV são classificadas em genótipos gB1 à gB4 (Chou & Dennison,
1991), gB5 (Shepp et al., 1996), e gB6 e gB7 (Trincado et al., 2000). A relevância
clínica destes diferentes genótipo ainda é assunto de debate: alguns estudos de
7
diferentes partes do mundo mostram uma possível correlação entre o tropismo de um
genótipo específico de gB com aumento de carga viral e manifestações clínicas (Aldo
Albuquerque Cunha, Vitor Hugo Aquino, Viviane Mariguela, Maurício Lacerda
Nogueira, 2011; de Campos Dieamant et al., 2010; Fries, Chou, Boeckh, & TorokStorb, 1994; Jin & Li, 2007; Madi, Al-Nakib, Pacsa, & Saeed, 2011; Meyer-König et
al., 1998; Roubalová, Strunecký, Zufanová, Procházka, & Vitek, 2010; Shepp et al.,
1996; Vogel et al., 2013; Y. Wu et al., 2007; Zhao & Zheng, 2012), enquanto outros não
encontraram essa correlação (Carraro & Granato, 2003; Görzer, Kerschner, RedlbergerFritz, & Puchhammer-Stöckl, 2010; Paradowska et al., 2012; Sarcinella, Mazzulli,
Willey, & Humar, 2002; Kaori Tanaka, Numazaki, & Tsutsumi, 2005; Tarrago,
Quereda, & Tenorio, 2003; Trincado et al., 2000; Yamamoto et al., 2007). No que se
trata de câncer nenhuma correlação foi ainda estudada entre os genótipos de gB e
tropismo ou aumento da malignidade tumoral.
Estudos in vitro visando elucidação de mecanismos virais levaram a descoberta
de diferenças nos genomas do HCMV, levando a criação do termo “linhagens virais”
para designar as mesmas. Linhagens conhecidas como laboratoriais são aquelas
passadas por várias vezes em cultura celular (geralmente de fibroblastos) como AD169
e Towne, e apresentam deleções e mutações adquiridas durante sua adaptação a cultura
(Davison, 2003; Ma et al., 2012). Estas linhagens diferem das chamadas linhagens
clínicas, como FIX e Toledo que não apresentam estes tipos de mutações e replicam-se
bem em células endoteliais e epiteliais.
O ciclo de replicação viral é lento, levando de 48 a 72 horas para produção de
progênie, com maior liberação viral dentre 72 a 96 horas. De forma geral o ciclo é
dividido em: adesão celular, penetração, expressão dos genes virais, replicação do DNA
viral, montagem dos capsídeos, aquisição do envelope e liberação celular (Mocarski et
al., 2006). Inicialmente a partícula viral se liga a superfície celular por interação das
glicoproteínas de envelope com receptores celulares, como heparan sulfato (T Compton,
Nowlin, & Cooper, 1993). Após esta primeira interação ocorre uma ligação entre a
glicoproteína gB e o receptor celular EGFR (do inglês, “epidermal growth factor
receptor”) (Wang, Huong, Chiu, Raab-Traub, & Huang, 2003), levando a fusão do
envelope com a membrana plasmática (Teresa Compton, Nepomuceno, & Nowlin,
1992) e liberação do capsídeo e proteínas/RNAs do tegumento no citoplasma celular.
No citoplasma, os capsídeos deslocam-se até o núcleo e o DNA viral é liberado através
8
dos poros nucleares (Dal Monte, Bessia, Landini, & Michelson, 1996; Ogawa-Goto et
al., 2003), iniciando-se a expressão dos genes virais.
Na chamada replicação produtiva a expressão gênica ocorre temporariamente em
forma de cascata. Os genes imediatamente precoces (IE, do inglês “Immediate-early”)
são os primeiros a serem expressos, seguidos pelos genes precoces (E, do inglês
“early”) e por fim os tardios ( L, do inglês “Late”) (Courcelle, Courcelle, Prichard, &
Mocarski, 2001). Os genes IE, mais abundantemente expressos, são transcritos a partir
da região conhecida como maior de IE (MIE, do inglês “major IE”), produzindo as
proteínas IE1 e IE2 (produtos do processamento alternativo do transcrito proveniente
da região UL122/23). As proteínas IE são transativadoras da expressão gênica e tem um
papel importante na expressão de genes virais e celulares: uma das funções destas
proteínas é a otimização do ambiente celular para a replicação viral e expressão gênica.
A expressão de proteínas IE é crucial para a expressão dos genes E, envolvidos na
replicação do DNA viral. Por fim, após a replicação do genoma viral os genes tardios
são expressos, sendo estes responsáveis pela formação de proteínas estruturais do
capsídeo viral, tegumento e envelope. O DNA recém-sintetizado é empacotado no
nucleocapsídeo que é transportado para o citoplasma através da membrana perinuclear,
onde adquire um envelopamento primário. No citoplasma o nucleocapsídeo adquire o
envelope secundário (e final) em membranas derivadas do Complexo golgiense onde
estão presentes glicoproteínas virais e algumas proteínas do tegumento. Finalmente, a
partícula completa é liberada da célula por exocitose (Figura 3). (Courcelle et al., 2001;
Sanchez, Sztul, & Britt, 2000; Silva, Yu, Enquist, & Shenk, 2003).
9
Figura 3: Esquema da replicação do HCMV. Inicialmente a partícula viral
liga-se a receptores celulares através das glicoproteínas de envelope, fusionando-se com
a membrana plasmática, e liberando o capsídeo e proteínas/RNAs virais no citoplasma
celular. O capsídeo é então deslocado até o núcleo onde o DNA viral é liberado através
dos poros e inicia-se a expressão dos genes virais. Os genes primeiramente expressos
são os IE (prevalentemente fatores de transcrição), seguidos pelos E (envolvidos na
replicação viral) e por fim os L (responsáveis pela formação de proteínas estruturais, do
capsídeo, do tegumento e envelope). O DNA viral é então empacotado no
nucleocapsídeo no núcleo celular e transportado para o citoplasma, onde adquire o
envelope final em membranas do retículo endoplasmático/complexo de Golgi, onde
estão as glicoproteínas virais. A partícula completa é liberada por exocitose.
10
Histórico do HCMV e câncer
A associação do HCMV com diferentes tipos de cânceres têm sido investigada
por décadas (Michaelis, Doerr, & Cinatl, 2009). Em 1971, Fuccillo et al. detectaram um
aumento nos títulos de anticorpos anti-HCMV em pacientes com carcinoma de cérvix,
quando comparado a indivíduos saudáveis. Desde então, muitos estudos detectaram
anticorpos anti-HCMV em pacientes com câncer e não em pessoas saudáveis, embora
com resultados inconclusivos (Michaelis et al., 2009).
Estudos realizados por Geder e colaboradores demonstraram que fibroblastos de
camundongos eram transformados pelo HCMV (Geder, Lausch, O’Neill, & Rapp,
1976). Estudos posteriores demonstraram que o HCMV é capaz de induzir mutações em
genes críticos para transformação oncogênica, no entanto, o DNA viral não foi
detectado na maioria das células transformadas. Em uma tentativa de explicar o
processo de transformação tumoral foi criada a teoria “hit and run”, a qual sugere que o
HCMV pode ser um fator responsável somente pela iniciação tumoral (Doniger,
Muralidhar, & Rosenthal, 1999)
Estudos subseqüentes não foram capazes de reproduzir os achados anteriores e
demonstraram que o HCMV não é capaz de induzir por si só a transformação em células
normais. Contudo, o DNA viral, mRNA virais e proteínas continuaram a serem
detectados em diversos tecidos tumorais e as evidências destes achados levaram a
criação do termo oncomodulação em 1996. Esta teoria postula que os distúrbios em uma
célula cancerosa, como alterações em vias de sinalização celular e controle
transcricional proporcionam um ambiente propício para que o vírus exerça seu potencial
oncomodulatório, aumentando assim a malignidade do tumor (Cinatl, Scholz, & Doerr,
2005; Cinatl Jr et al., 1996). Suporte para a teoria de oncomodulação veio a partir de
estudos que mostraram a influência de proteínas do HCMV em anormalidades presentes
em
células
tumorais
incluindo
proliferação
celular,
sobrevivência,
invasão,
imunogenicidade, angiogênese tumoral e instabilidade cromossomal (Michaelis et al.,
2009).
Estudos em biópsias utilizando-se de técnicas altamente sensíveis continuaram a
detectar o HCMV em vários tipos de tumores como: carcinoma coloretal (Dimberg et
al., 2013; Harkins et al., 2002), câncer de próstata (Samanta, Harkins, Klemm, Britt, &
Cobbs, 2003), câncer de pele (Zafiropoulos, Tsentelierou, Billiri, & Spandidos, 2003),
rabdomiosarcomas (Price RL, Bingmer K, Harkins L, Iwenofu OH, Kwon CH, Cook C,
Pelloski C, 2012), Câncer de mama (El-Shinawi & Mohamed, 2013), carcinoma
11
mucoepidermoide de glândulas salivares (Melnick, Deluca, Sedghizadeh, & Jaskoll,
2013), (Baryawno et al., 2011; Wolmer-Solberg et al., 2013) e glioblastoma multiforme
(compilado em (Dziurzynski et al., 2012)).
Glioblastoma
Os tumores cerebrais são uma das principais causas de morte entre a população
em geral. No total, estima-se que cânceres do sistema nervoso central (SNC)
compreendam 1,1% dos tumores malignos de ocorrência recente, sendo a terceira causa
de mortes entre 15 a 34 anos de idade e a quarta em homens entre 35 a 54 anos. Estes
tumores apresentam uma grande variedade de tipos e são classificados de acordo com o
local, o tipo de tecido envolvido e invasividade, além de outros fatores (Pytel & Lukas,
2009). Dois cortes de uma imagem de ressonância magnética de um cérebro com
glioblastoma multiforme são mostrados na Figura 4.
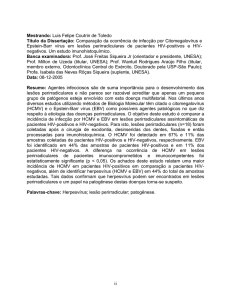
Figura 4: Imagem de ressonância magnética de cérebro com glioblastoma
multiforme. A imagem axial em (A) o círculo apontado pela seta indica a região central
do tumor (necrose) circundada por um padrão de anel. (B) Imagem axial T2 do mesmo
tumor, a seta indica região periférica a zona necrótica com células tumorais infiltrativas
e edema vasogênico (Adaptado de Rong & Brat, 2009).
Os tumores conhecidos como gliomas (provenientes de células da glia), são os
mais comuns. Quando ocorrem nos astrócitos recebem a denominação de astrocitoma,
12
que podem ocorrer em quatro graus. Os graus inferiores (I e II) correspondem a tumores
benignos com células diferenciadas, que não invadem tecidos adjacentes e não resultam
em metástases, nem todos os tumores de grau I e II evoluem para tumores de alto grau .
Já os de níveis superiores (III e IV) são tumores malignos que apresentam baixa taxa de
sobrevivência. Gliomas de grau IV são chamados de glioblastomas e correspondem a
0,0257% de todos os tumores humanos (Holland, 2000; Kleihues P, Louis DN,
Scheithauer BW, Rorke LB, Reifenberger G, Burger PC, 2002; Marumoto & Saya,
2012; Newton, 1994).
O glioblastoma multiforme (GBM) é o tumor do SNC mais frequente e o mais
maligno, representando cerca de 50,7% dos tumores do cérebro (Kneifel et al., 2006).
Caracteriza-se por apresentar uma população celular heterogênea, geneticamente
instável, proliferação celular muito acelerada, angiogênese, alta taxa de infiltração e
resistência a quimioterapia (Ramirez, Weatherbee, Wheelhouse, & Ross, 2013).
GBMs são ainda patologicamente caracterizados pela presença de áreas
necróticas e vasculatura aberrante com agloremados glomeroides e hiperproliferativos, e
vasos sanguíneos desorganizados e vazantes (Ramirez et al., 2013). Clinicamente
podem ser divididos em dois tipos: o primário, que acomete pessoas mais velhas e não
são correlacionados com evidências anteriores de outros tipos de tumores de baixo grau;
e secundário, que ocorre em indivíduos mais jovens (menos de 45 anos), e são
provenientes de gliomas de baixo grau, desenvolvendo-se em 5 a 10 anos após o
diagnóstico inicial (Marumoto & Saya, 2012).
O tratamento padrão para GBM é a cirurgia associada à radioterapia e
quimioterapia; sendo a Temozolomida (comercializada como Temodal® pela empresa
Schering-Plough) a droga mais comumente utilizada. A Temozolamida (TMZ) é um
ácido estável administrado oralmente, uma pró-droga alquilante que atravessa as
barreiras hemato-encefálica e encéfalo-tumoral (BBB e BTB, do inglês “blood–brain” e
“blood–tumor” respectivamente). Em pH neutro ou alcalino ocorre a abertura hidrolítica
do anel de seis membros, produzindo o intermediário triazeno de cadeia aberta (MTIC,
do inglês “open-chain triazene”). O intermediário MTIC ativo libera então um
grupamento metildiazônio, que metila o DNA. Cerca de 70%, 10% e 5% dos grupos
metil transferidos para o DNA estão em sítio N7-guanina, N3-adenina e O6-guanina,
respectivamente (Ramirez et al., 2013). A via de ativação de MTIC e metilação de DNA
é mostrada na Figura 5.
13
Figura 5: Ativação da pró-droga TMZ. Em pH ~7.4 ocorre abertura do anel de 6
membros produzindo o intermediário MTIC. O MTIC ativo libera metildiazônio que
metila o DNA liberando N2 altamente estável. Cerca de 70%, 10% e 5% dos grupos
metil transferidos para o DNA estão em sítio N7-guanina, N3-adenina e O6-guanina,
respectivamente (adaptado de Ramirez et al, 2013).
Mesmo com a ressecção do tumor e tratamentos quimioterápico e radioterápico
combinados a média de sobrevivência dos pacientes após diagnóstico é de 15 meses
(Affronti et al., 2009). Uma possível explicação a esta baixa taxa de sobrevivência é a
falta de especificidade do tratamento quimioterápico as células tumorais, uma vez que
as drogas utilizadas são de amplo espectro (agentes alquilantes, inibidores de
topoisomerases) (Newton, Turowski, TJ, & Al, 1999; Newton, 2006). Outra possível
explicação é a liberação inadequada das drogas através das BBB e BBT, além do alto
grau de resistência intrínseca a quimioterapia presente na maior parte dos tumores de
alto grau (Newton, 2010).
A etiologia deste tipo de tumor ainda é desconhecida, entretanto alguns estudos
mostraram que a exposição à radiação ionizante ou campo magnético podem ser fatores
de risco (Ohgaki, 2009). Atualmente é aceito que o fenótipo transformado das células
tumorais é resultante de disfunções de uma variedade de vias regulatórias
interrelacionadas (Chung & Seizinger, 1991; Maehama & Dixon, 1998; Shapiro &
Coons, 1998; von Deimling, Louis, & Wiestler, 1995). Sendo o processo de
transformação uma amplificação e superexpressão de oncogenes em combinação com a
perda ou falha na expressão de genes supressores de tumor.
14
Os oncogenes mais relevantes para a gliomagênese incluem o fator de
crescimento derivado de plaquetas e seu receptor (PDGF e PDGFR, do inglês “plateletderived growth factor” e “platelet-derived growth factor receptor”), o fator de
crescimento epidermal (EGF, do inglês “epidermal growth factor”) e seu receptor
EGFR, o gene do sarcoma de ratos (Ras, do inglês, “Rat sarcoma gene”), o gene Akt, e
a alvo mamífero da rapamicina (mTOR, do inglês “mammalian target of rapamycin”).
Em um subconjunto de tumores do tipo GBM observa-se a expressão de uma variante
de EGFR, a EGFRVIII que não contém o domínio extracelular do receptor, levando a
ativação constitutiva do mesmo (Ramirez et al., 2013).
Os genes supressores de tumores relevantes na transformação glial geralmente
mutados incluem p53, retinoblastoma (Rb), p16 e p15 (como INK4a, INK4b), DMBT1
e PTEN (Arita, Hayakawa, Izumoto, & Al, 1989; Choe et al., 2003; Feldkamp, Lala,
Lau, & Al, 1999; Frederick, Wang, Eley, & James, 2000; Gilbertson et al., 2001; a
Guha, Feldkamp, Lau, Boss, & Pawson, 1997; A. Guha, Dashner, Black, Wagner, &
Stiles, 1995; Heimberger et al., 2005; LaRochelle, Jeffers, McDonald, & Al, 2001;
Lokker, Sullivan, Hollenbach, Israel, & Giese, 2002; Maher et al., 2001; Newton, 2010;
Normanno et al., 2006; Sakata, Kato, Fox, & Al, 2002; Shapiro & Coons, 1998; von
Deimling et al., 1995; Westermark, Heldin, & Nister, 1995). A maioria destes genes
supressores de tumores funcionam como reguladores negativos do ciclo celular,
enquanto outros são importantes inibidores de vias de transdução de sinais associados a
proliferação e sobrevivência celular.
O efeito geral destas anormalidades adquiridas é uma falta de balanço entre a
atividade do ciclo celular e as vias de morte celular programada, gerando então um
ambiente celular alterado e a posterior carcinogênese.
HCMV e glioblastoma
Os estudos de investigação da relação entre o HCMV e glioblastoma iniciaramse com o trabalho de Cobbs et al, 2002 (Cobbs et al., 2002) no qual a proteína IE1 foi
detectada por imunohistoquímica (IHC) em 100% de amostras de GMB, com expressão
restrita a células tumorais (não sendo encontrada expressão viral em células normais
adjacentes). Entretanto, estudos subsequentes falharam na detecção do HCMV em
amostras tumorais (Lau et al., 2005; Poltermann et al., 2006) ou detectaram a presença
viral em baixos níveis (Sabatier et al., 2005), levando a uma controvérsia na literatura
quanto à presença ou não do vírus neste tipo de tumor.
15
Estudos posteriores de Scheurer et al, 2008 e Mitchell et al, 2008 (D. a Mitchell
et al., 2008; Scheurer, Bondy, Aldape, & Albrecht, 2010) demostraram que a
discrepância entre os resultados obtidos por Cobbs et al e os de outros grupos era
proveniente de diferenças entre a sensibilidade das técnicas utilizadas por cada grupo.
Utilizando-se de técnicas altamente sensíveis, Scheurer et al, 2008 detectaram a proteína
IE1 em 100% das amostras de GBM e em 82% das amostras de glioblastomas de baixo
grau por IHC (Scheurer et al., 2010), validando os resultados inicialmente publicados
por Cobbs et al, 2002 (Cobbs et al., 2002).
Estudos mais recentes também confirmaram a presença do genoma do HCMV e
proteínas virais em uma alta porcentagem em amostras de GBM. Mitchell et al, 2008
(93% por IHC para IE1) (D. a Mitchell et al., 2008); Lucas et al, 2010 (51% por IHC
para pUL83) (Lucas, Bao, Bruggeman, Dunham, & Specht, 2011); Soroceanu et al,
2011(65% por IHC para pUS28) (Soroceanu et al., 2011); Ranganathan et al, 2011
(70% por PCR para múltiplas regiões do HCMV) (Ranganathan, Clark, Kuo, Salamat,
& Kalejta, 2012); Slinger et al, 2012 (96% por IHC para IE1) (Slinger et al., 2010);
Fonseca et al, 2012 (36% por PCR para pUL83) (Fonseca & Kawamura, 2012); Rahbar
et al, 2012 (99% por IHC para IE1) (Rahbar et al., 2012) , Rahbar et al, 2013 (99% por
IHC para IE1) (Rahbar et al., 2013), dos Santos et al, 2013 (95% por qPCR para UL83
(Dos Santos et al., 2013).
Atualmente há um consenso na literatura de que o HCMV está presente na
maioria, se não em todos os tumores do tipo GBMs, e que é possível que o mesmo
module o fenótipo maligno do tumor, sendo então considerado um agente
oncomodulatório neste tipo de tumor (Dziurzynski et al., 2012).
Possíveis mecanismos moleculares de indução da oncomodulação pelo HCMV
A biologia dos tumores está associada com um uma desregulação de processos
normais das células, tais como: ciclo celular, proliferação, motilidade e reconhecimento
do sistema imune, sendo várias proteínas codificadas pelo HCMV capazes de interferir
com estes processos.
As proteínas immediate early 1 (IE1-72), immediate early 2 (IE2-86) e a
proteína do tegumento pp71 são capazes de se ligar a proteínas da família Rb (pRb,
p107 e p130) e inibir suas funções promovendo entrada da células na fase S do ciclo
celular (Hagemeier, Caswell, Hayhurst, Sinclair, & Kouzarides, 1994; Kalejta & Shenk,
2003; Poma, Kowalik, Zhu, Sinclair, & Huang, 1996; K. Tanaka et al., 1999). A
16
proteína kinase UL97, é capaz de fosforilar e inativar pRb inibindo assim sua função
(Hume et al., 2008).
Diversas proteínas virais são capazes de inibir apoptose. A proteína IE2-86, em
alguns tipos celulares, é capaz de se ligar a p53 e inibir sua função de transativação,
impedindo a indução de apoptose mediada por p53 (K. Tanaka et al., 1999); a proteína
codificada pelo gene UL36 se liga caspase 8, inibindo apoptose mediada por Fas
(Skaletskaya et al., 2001); a proteína produto do gene UL37 exon1 (UL37x1) bloqueia o
recrutamento dos membros da família Bcl-2, Bax e Bak para a mitocôndria resultando
em inibição de sua função (Goldmacher et al., 1999), já a proteína codificada pelo gene
UL38 bloqueia ativação de caspase 3 (Terhune et al., 2007).
Particularmente no que se trata de GBMs, evidências sugerem que o HCMV é
capaz contribuir na indução do processo angiogênico, através da ligação da proteína
viral US28 a um receptor celular tipo GPCR (do inglês “G-protein-coupled receptor”).
Experimentos demonstraram que a proteína US28 induz expressão de EGF in vitro e in
vivo. Além disso, linhagens celulares de glioblastoma que expressam esta proteína
produzem tumores mais malignos quando injetadas em camundongos (Maussang et al.,
2006). Recentemente foi ainda demonstrado que as proteínas IE72 e IE86 são capazes
de ativar a expressão da enzima telomerase, evento crucial para transformação celular
(Strååt et al., 2009).
Além disso, estudos clínicos recentes mostraram que pacientes com baixos
níveis de expressão de HCMV mostraram índices de sobrevivência melhores que
aqueles com altas cargas virais (Rahbar et al., 2012, 2013; Söderberg-Nauclér, 2008),
corroborando assim as evidências de que a presença do vírus colabora com a modulação
do fenótipo maligno
17
Objetivo
Objetivo geral
Investigação da presença do citomegalovírus humano em glioblastoma
multiforme
Objetivos específicos
Otimização das técnicas de PCR convencional, PCR em tempo real e
semi-nested PCR para a detecção do DNA viral;
Detecção do DNA viral em amostras de tumores e de sangue periférico
de pacientes com GBM;
Determinação dos genótipos da glicoproteína gB presentes no sangue e
tumor dos mesmos pacientes;
Correlação entre os genótipos de gB presentes no sangue e tumor dos
mesmos pacientes;
Quantificação de carga viral em sangue periférico e tumores de pacientes
com GBM;
Correlação entre a carga viral do sangue periférico de pacientes com
GBM e pacientes transplantados renais.
18
Materiais e Métodos
Amostras Clínicas
Vinte e duas amostras de biópsias tumorais e vinte amostras de sangue periférico
de pacientes com GBM foram obtidas do Centro de Neurologia do Hospital das Clínicas
de São Paulo, em um estudo colaborativo (processo FAPESP: 2010/14830-7) com
aprovação do comitê de ética local (aprovação nº0654/10). Sete amostras de DNA de
sangue de pacientes transplantados renais também foram gentilmente cedidos pela
Faculdade de Medicina de São José do Rio Preto, as amostras foram submetidas a testes
imunológicos e apresentaram alta carga viral. Todos os pacientes foram informados do
procedimento e assinaram um termo de consentimento livre e esclarecido. As amostras
tumorais foram histopatologicamente diagnosticadas através do método tradicional de
coloração de hematoxilina e eosina (HE) e classificadas de acordo com os critérios da
Organização Mundial de Saúde (Louis, 2006) como GBMs. As amostras de sangue
foram coletadas em tubos de heparina e as amostras tumorais em solução de RNAlater
(Invitrogen). Todas as amostras foram mantidas a 4ºC até o transporte para a
Universidade Federal do ABC (UFABC) aonde foram processadas para realização das
técnicas descritas abaixo.
Extração de DNA
O DNA total das amostras foi extraído a partir de 20 mg de tecido tumoral ou de
200 µl de sangue periférico, utilizando-se os kits: Pure Link genomic DNA mini kit
(Invitrogen)
e
ReadyAmpTM
Genomic
DNA
purification
system
(Promega),
respectivamente, de acordo com as instruções do fabricante.
DNA viral
O DNA da linhagem clínica FIX do HCMV, clonado como um Cromossomo
Bacteriano Artificial (HCMV FIX-BAC), gentilmente doado por Thomas Shenk
(Universidade de Princeton), foi utilizado no estabelecimento do limite de detecção nas
reações de PCR.
Para obtenção de estoques de DNA viral células de E. Coli contendo o HCMV
FIX-BAC foram crescidas em 200 ml de meio Lysogeny broth (LB) contendo 25mg/ml
de clorafenicol a 37ºC por 16 horas. O DNA foi purificado com coluna NucleoBondXtra Midi Plus e ressuspendido em 100µl de tampão TE (10 mM Tris, 1 mM EDTA, pH
19
8). Após purificação o DNA foi quantificado por espectofotometria por absorbância em
comprimento de onda 260 nm.
PCR qualitativo
Amplificações por PCR convencional (cPCR) foram realizadas em reações com
volume final de 50 µL contendo 2 µL de DNA; 2 mM MgCl2; 200 µM dNTPs; 0,75 mM
de cada primer, e 5U de Taq Polimerase (Ludwig Biotec). As condições do cPCR
foram: 94ºC por 3 min, seguido por 40 ciclos de 94ºC por 30 seg; 55,6ºC por 30 seg;
72ºC por 45 seg, finalizado por 72ºC por 10 min.
Para amplificação do DNA viral foram utilizados os seguintes primers: UL44
(5’-TAC AAC AGC GTG TCG TGC TCC G-3’ e 5’-GGC GTG AAA AAC ATG CGT
ATC AAC-3’), UL123 (5’-GCC TTC CCT AAG ACC ACC AAT-3’e 5’-ATT TTC TGG
GCA TAA GCC ATA ATC-3’), UL99 (5’-GTG TCC CAT TCC CGA CTC G-3’ e 5’TTC ACA ACG TCC ACC CAC C-3’) (D. P. Mitchell et al., 2009). Como controle
positivo para DNA celular, primers para o gene Gliceraldeído 3-Fosfato Desidrogenase
(GAPDH) foram utilizados (5’-ACC CAC TCC TCC ACC TTT GAC-3’e 5’-CTG TTG
CTG TAG CCA AAT TCG T-3’).
PCR em tempo real quantitativo.
O DNA viral foi amplificado por PCR em tempo real (qPCR) utilizando-se os
primers descritos anteriormente (UL44, UL123, UL99 e GAPDH), e também um par de
primers para a região UL83 do genoma viral (5’-CCC AGG TGT GTC GGT ACT CA3’and 5’-CCA CCT TCA CCA GCC AGT ATC-3'), desenhado utilizando-se o
programa PrimerExpress software (Applied Biosystems). As reações foram realizadas
em aparelho StepOne Plus real-time PCR system (Applied Biosystems) em um volume
final de 10 µl contendo 1 µl de DNA; SYBER Green 1x (Applied Biosystems) e 0,62
µm de cada primer. As condições do PCR utilizadas foram: 95ºC por 10 min, seguido
por 40 ciclos de 95ºC por 15 seg, 60ºC por 1 min e 72ºC por 30 seg. Os dados foram
coletados e analisados utilizando-se o programa Step One Software v. 2.2 (Applied
Biosystems).
Semi-nested PCR e caracterização dos genótipos da glicoproteína gB.
As reações de semi-nested PCR (nPCR) foram realizadas utilizando-se primers
para a região variável do gene UL55 (glicoproteína gB) previamente descrito por Wu et
20
al. 2010. As reações foram realizadas em um volume final de 50 µL contendo 2 µL de
DNA; tampão Taq Polymerase 1x; 2 mM de MgCl2; 2,5 U de Taq Polymerase (Ludwig
Biotec); 200 µM de dNTPs e 0,15 µM de cada primer. A primeira etapa de amplificação
foi realizada com os primers: 5´-TGT TCT GGC AAG GYA TCA AG-3´ e 5´-TCA
CAA GAC ATC ACC CAT GAA AC-3´ e a segunda etapa com os primers: 5´-TGT
TCT GGC AAG GYA TCA AG-3´ e 5´-GTT GTT GTA RAT GGC YGA GAG-3´. As
condições do PCR foram: 94ºC por 14 min, seguido por 35 ciclos de 95ºC por 30 seg;
56,2ºC por 30 seg; 72ºC por 45 seg; 72ºC por 10 min. Todas as reações foram repetidas
pelo menos três vezes para confirmação dos resultados e exclusão de resultados falsopositivos e negativos.
A fim de evitar contaminação, controles positivos foram somente utilizados
durante a otimização das técnicas, com exceção do qPCR, no qual uma curva padrão de
DNA viral foi analisada juntamente com as amostras. Os produtos amplificados foram
visualizados em gel de agarose corado com gel red (Uniscience), as bandas foram
cortadas e o DNA extraído foi analisado por sequenciamento (Serviço de
Sequenciamento de DNA-SSDNA IQUSP).
Determinação dos genótipos nas amostras de sangue e tumor.
A confirmação das sequências de HCMV e determinação dos genótipos de gB
nas amostras positivas por nPCR foram realizados utilizando-se a ferramenta Blast
presente no site do National Center for Biotechnology Information (NCBI-USA),
comparando-se as sequências obtidas com sequências de referência da literatura.
Determinação dos limites de detecção do DNA viral e quantificação de DNA
genômico.
Para determinação do limite de detecção do DNA viral pelas técnicas de cPCR,
qPCR e nPCR foram realizadas reações utilizando-se o HCMV FIX-BAC de
concentração conhecida em diluições seriadas de 10x adicionado a sangue sabidamente
negativo para HCMV, antes da purificação do DNA total (DNA viral mais DNA
genômico).
O cálculo do limite de detecção de DNA viral foi realizado conforme descrito
por (Cunha, Marin, Aquino, & Figueiredo, 2002). Para tanto, considerou-se o peso
médio de um par de bases 660g/mol. Sabendo-se que o tamanho do genoma do FIX
BAC é de 240 kb, o peso molecular do plasmídeo é de 158,4.106g/mol.
21
A quantidade de DNA viral nas amostras foi determinada a partir da correlação
entre curvas de amplificação dos genes pp65 e GAPDH, utilizando-se
diluições
seriadas de DNA viral e celular, respectivamente. Um fator de conversão de 6 pg por
célula diploide foi utilizado para calcular o número de células total em cada amostra.
A carga viral nos tecidos tumorais e no sangue dos pacientes foi calculada como
log da razão entre o número de células por cópia de DNA viral (log (número de
células/cópia pp65)). Já nas amostras de sangue de pacientes com GBM e
transplantados renais a carga viral nas amostras foi expressa em log cópias pp65/ml.
22
Resultados
Cálculo do limite de detecção do DNA viral da pelas técnicas de cPCR, qPCR
nPCR
A fim de avaliar o melhor método de detecção do DNA viral em amostras de
GBM três diferentes técnicas de PCR foram empregadas: PCR convencional (cPCR),
PCR qualitativo em tempo real (qPCR) e semi-nested PCR (nPCR) utilizando-se
primers para diferentes regiões do genoma viral: UL44 (DNA polimerase viral), UL123
(proteína IE1), UL99 (proteína pp28), UL83 (fosfoproteína 65) e UL55 (glicoproteína
B). Conforme mencionado previamente, a replicação do HCMV ocorre em cascata
temporal e os genes supracitados foram escolhidos de forma a contemplar cada uma das
fases da cascata; o gene UL123 é um gene imediatamente precoce, os genes UL44,
UL83 e UL55 são genes precoces e o gene UL99 é um gene tardio.
Para determinação do limite de detecção do DNA viral pelas diferentes técnicas
de PCR, foram realizadas reações contendo DNA celular extraído de uma amostra de
sangue HCMV negativo, contendo adições de diluições seriadas de 10x do genoma do
HCMV FIX-BAC em concentrações conhecidas. As maiores sensibilidades obtidas
foram: 7000 cópias/ µl em cPCR com primers para a região UL44 (cPCR-7000 cópias/
µl), 9 cópias/µl em nPCR para a região variável do gene UL55 e finalmente 2
cópias/µl e, qPCR para a região UL83 (Figura 6). As técnicas de nPCR e de qPCR para
amplificação dos genes UL55 e UL83, respectivamente, foram utilizadas para análises
posteriores de detecção do DNA viral em amostras clínicas, por apresentarem uma
melhor sensibilidade quando comparadas ao cPCR e por não existir diferença
significativa entre de sensibilidade entre ambos.
23
-4
-5
-2
-3
10-1 10 10 10 10
10-1
10
-2
10
-3
-5
-6
-7
10-4 10 10 10
10-8
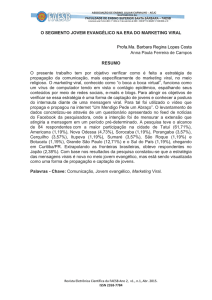
Figura 6: Limite de detecção de HCMV obtido por nPCR e qPCR. (a) Eletroforese
em gel de agarose 1,5% dos produtos de amplificação obtidos por nPCR e (b) Curvas de
amplificação dos produtos obtidos por qPCR. Em ambos os casos os limites de detecção
foram determinados por amplificação de diluições seriadas de 10x do HCMV FIXBAC de concentrações conhecidas adicionadas a DNA genômico (extraído de sangue de
paciente HCMV negativo). O gene GAPDH foi amplificado como controle da presença
de DNA celular (dados não mostrados). Os melhores limites de detecção obtidos foram
de 9 cópias/µl por nPCR (gene UL55) e 2 cópias/µl por qPCR (gene UL83).
24
Detecção do genoma viral nas amostras de tumores e sangue de pacientes com
GBM
A detecção do genoma viral nas amostras de GBM e sangue periférico dos
pacientes do Centro de Neurologia do Hospital das Clínicas de São Paulo- Brasil, foi
realizada pelas técnicas de qPCR e nPCR utilizando-se os primers UL83 e UL55
respectivamente.
A região variável do gene UL55 foi detectada em 20 das 22 (91%) amostras
tumorais (Figura 7 (a)) e 11 das 20 (55%) amostras de sangue periférico por (Figura 7
(b)) nPCR. Utilizando-se a técnica de qPCR para amplificação do gene UL83, 21 das
22 (95%) amostras de tumores (Figura 8 (a)) e 9 das 20 (45%) amostras de sangue
periférico (Figura 8 (b)) foram positivas quanto a presença viral.
25
26
Figura 7: Detecção do HCMV por nPCR em amostras de sangue e tumor de
pacientes com tumores cerebrais. Eletroforese em gel de agarose 1,5% dos produtos
obtidos a partir da amplificação do DNA extraído de amostras de tumores (A) e de
sangue (B), utilizando-se primers para a região variável do gene que codifica a proteína
gB (316 pb) do HCMV. O fragmento do gene GAPDH (203 pb) foi amplificado como
controle celular. H2O foi utilizada como controle negativo. P01 à P22 referem-se a
pacientes com GBM e OT a outros tumores que não GBMs (não incluídos neste estudo).
27
Figura 8: Detecção do HCMV por qPCR em amostras de tumor de pacientes com tumores
cerebrais. Curvas de amplificação obtidas por qPCR de amostras de tumor utilizando-se de
primers para as regiões pp65 do HCMV (a) e o gene celular GAPDH (b). Nestas curvas cada cor
representa um diferente paciente.
28
Nos casos em que foi possível obter amostras de sangue e tumor do mesmo
paciente, foi realizada uma correlação entre a presença do DNA viral em ambas as
amostras. Em um total de 19 amostras analisadas, para a região do gene UL83, que
codifica a proteína pp65, por qPCR, 9 de 19 (47%) mostraram positividade em tumor e
sangue. A presença da região UL55, que codifica a proteína gB, por nPCR foi detectada
em 11 de 18 amostras (61%) de sangue e tumor. Os resultados obtidos estão
sumarizados na tabela 1.
Tabela 1. Frequência da detecção de HCMV por qPCR (gene UL83) e nPCR (gene
UL55) e correlação da positividade nas amostras de sangue e tumor de pacientes com
GBM.
Sangue x Tumor
pp65 (qPCR)
gB (nPCR)
Tumor (+) total
21 de 22 (95%)
20 de 22 (91%)
Sangue (+) total
9 de 20 (45%)
11 de 20 (55%)
Tumor (+) / Sangue (+)
9 de 19 (47%)
11 de 18 (61%)
Determinação e correlação entre genótipos de gB em amostras de sangue periférico
e tumores de pacientes com GBM.
Com o intuito de investigar a similaridade das linhagens virais presentes no
sangue periférico e nas amostras tumorais do mesmo paciente, os produtos de
amplificação do PCR foram sequenciados e os genótipos da glicoproteína gB
determinados. As sequências obtidas foram analisadas por comparação com sequências
de referências utilizando a ferramenta BLAST presente no site do NCBI-USA.
O genótipo gB2 foi detectado em 17 do total de 20 amostras tumorais positivas
para o HCMV. As três amostras restantes possuem genótipo gB3. Todas as 11 amostras
de sangue positivas para a presença do HCMV possuem genótipo gB2. Em pacientes
positivos nos tumores e no sangue, o genótipo gB encontrado em ambas as amostras
eram coincidentes (gB2). Genótipos gB1, gB4, gB5, gB6 e gB7 não foram encontrados
(Tabela 2).
29
Tabela 2: Frequência do genótipo de gB nas amostras de tumor e sangue periférico de
pacientes com GBM.
Genótipo
Tumor
Sangue
gB 1
0 /20 (0%)
0/11 (0%)
gB 2
17/ 20 (85%)
11/11 (100%)
gB 3
3 /20 (15%)
0/11 (0%)
gB 4
0/ 20 (0%)
0/11 (0%)
gB 5
0/ 20 (0%)
0/11 (0%)
gB 6
0/ 20 (0%)
0/11 (0%)
gB 7
0/ 20 (0%)
0/11 (0%)
Carga viral nas amostras de sangue e tumor.
Para estimativa da carga de DNA viral nas amostras foi realizada uma correlação
entre a quantidade de DNA celular e viral presente nas mesmas. Conforme demonstrado
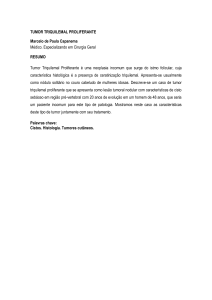
na Figura 9 (a) na maioria dos tumores analisados a quantidade de DNA celular é muito
maior do que a de DNA viral. O número de cópias virais varia de extremamente alto
(3,16.104 pp65/célula) em um paciente (P6) para muito baixo (média de 4,77.10-3
pp65/célula) em alguns pacientes (P5, P13, P15, P17, P21). Em média, 1 em cada 33
células contém o DNA viral.
A carga viral em amostras de sangue positivas para HCMV foi também
determinada e para comparação, oito amostras de pacientes transplantados renais foram
incluídas nas análises. Conforme demostrado na Figura 9 (b) não há diferença
significante na carga viral destes dois tipos de amostras. O número de cópias médio em
pacientes com GBM e transplantados renais foi de 1,3 x 105 e 3,2 x 105 cópias pp65 /ml,
respectivamente.
30
Figura 9: Quantificação de DNA viral do HCMV por qPCR em amostras de
tumores e sangue periférico de pacientes com GBM. (a) Vinte e duas amostras de
tecido tumoral foram analisadas por qPCR utilizando-se de primers para a região do
gene que codifica a proteína viral pp65 e para o gene celular GAPDH. A relação entre o
DNA celular e o DNA viral é expressa como log10. (b) Nove e oito amostras de sangue
provenientes de pacientes com GBM e transplantados renais, respectivamente foram
analisadas por qPCR para a região viral pp65. A carga viral é expressa em número de
cópias do vírus/ml.
31
Discussão
A presença do HCMV em tumores do tipo GBM tem sido questão de debate nos
últimos anos. Desde as primeiras descobertas da associação do HCMV com GBM
(Cobbs et al., 2002), vários estudos foram realizados visando à identificação da
presença do genoma do HCMV e expressão de proteínas virais neste tipo de tumor.
Entretanto, apesar de uma considerável quantidade de trabalhos neste tema, sua grande
maioria foi ou está sendo conduzida na Europa e Estados Unidos. Logo, trabalhos
adicionais da verificação da presença do vírus em amostras de diversas regiões do
mundo são de extrema relevância, particularmente para determinar a presença ou não do
HCMV em GBMs e sua frequência em diferentes populações, que podem ser
geneticamente distintas;.
O primeiro estudo da verificação da associação entre o HCMV e GBM mostrou
a presença do vírus, restrita a células tumorais, em alta frequência neste tipo de tumor,
(Cobbs et al., 2002). Entretanto, outros grupos não conseguiram reproduzir estes
resultados, gerando uma controvérsia na literatura sobre a possível presença viral neste
tipo de tumor (Lau et al., 2005; Poltermann et al., 2006). Estudos posteriores (D. a
Mitchell et al., 2008; Scheurer et al., 2010) mostraram que a ausência de detecção era
decorrente da baixa sensibilidade das técnicas utilizadas, sendo necessária assim uma
otimização das metodologias a serem utilizadas antes da detecção do vírus em amostras
clínicas.
No presente estudo três diferentes técnicas de PCR (cPCR, nPCR, qPCR) foram
inicialmente otimizadas comparando-se sua sensibilidade para detecção do genoma do
HCMV em amostras de sangue periférico e tumores do tipo GBM. Os resultados
demonstraram que a técnica de qPCR (2 cópias/µl), seguida por nPCR (9cópias/µl) são
as mais sensíveis para a detecção do HCMV, com os primers para as regiões UL83 e
UL55, respectivamente.
A maioria dos estudos que avaliaram a presença do HCMV em amostras de
GBM
utilizaram-se
das
técnicas
de
imunohistoquímica
(IHC,
do
inglês
“Immunohistochemistry”) ou hibridação in situ (ISH, do inglês “In situ hybridization”).
Embora estas técnicas sejam sensíveis e adequadas para a localização de proteínas virais
ou DNA em células únicas, elas são laboriosas e custosas. Detecção de regiões
genômicas por PCR são menos custosas e mais convenientes para triagens.
32
Conforme mencionado anteriormente, poucos estudos investigaram a presença
do DNA viral em amostras de GBM por PCR. Cobbs et al, 2002 por nested PCR
detectaram gB em 77,7% de amostras de GBM em parafina (Cobbs et al., 2002).
Entretanto, utilizando-se da mesma técnica Polterman et al, 2006 e Lau et al, 2005
falharam na detecção de gB em 22 e 8 amostras de GBM em parafina, respectivamente
(Lau et al., 2005; Poltermann et al., 2006). Mitchell et al, 2008 por qPCR detectaram gB
em 61,7% e 70% de amostras de GBM em parafina e em células primárias de GBM
respectivamente (D. a Mitchell et al., 2008). No entanto, Lau et al, 2005 por cPCR
falharam na detecção de gB em 8 amostras de GBM em parafina (Lau et al., 2005).
Ranganathan et al, 2011 foi o único grupo a detectar várias regiões do genoma viral em
amostras de GBM por cPCR (UL17, UL27, UL55, UL69, UL82, UL96, UL144, US2,
US11 e US28) (Ranganathan et al., 2012). Em nosso estudo a presença do DNA viral
nas amostras clínicas pela técnica de cPCR não foi detectada, utilizando-se três
diferentes pares de primers (UL123, UL44 e UL99). A ausência de detecção por cPCR
pode ser atribuída a diferenças na sensibilidade dos primers utilizados nos trabalhos
previamente descritos na literatura, quando comparado aos utilizados neste estudo
(Ranganathan et al., 2012). Outro fato a ser levado em consideração é a variação na
sequência alvo dos primers ou a variabilidade nas sequências genômicas do HCMV em
diferentes regiões geográficas, como descrito por Renzette et al, 2011 (Renzette,
Bhattacharjee, Jensen, Gibson, & Kowalik, 2011).
Utilizando-se das técnicas que apresentaram melhor sensibilidade durante a
otimização, as regiões UL83 e UL55 do HCMV foram detectadas, em nosso estudo, em
95% (qPCR) e 91% (nPCR) das amostras de tumores, respectivamente. Logo, os dados
obtidos confirmam a presença do genoma do HCMV na maioria das amostras de GBM
provenientes de uma população do Brasil.
Poucos trabalhos na literatura mostram ainda uma correlação entre a presença do
genoma viral nas amostras tumorais e no sangue periférico dos pacientes. Enquanto
Polterman et al, 2006 e Lehrer et al, 2011 falharam na detecção do vírus, Mitchell et al,
2008 mostraram que 50% dos pacientes com GBM eram positivos para o HCMV nos
tumores e em sangue periférico concomitantemente (Lehrer & Labombardi, 2011; D. a
Mitchell et al., 2008; Poltermann et al., 2006).
Nos casos em que foi possível a obtenção de amostras de sangue periférico e
tumor do mesmo paciente uma correlação entre a presença do HCMV foi realizada
neste estudo. Pelas técnicas de qPCR e nPCR, 9 de 19 pacientes (47%) e 18 de 11
33
pacientes (61%) mostraram-se positividade em ambas as amostras.. Estes dados
ratificam aqueles encontrados previamente na literatura (D. a Mitchell et al., 2008).
Análises dos genótipos virais da glicoproteína gB demonstraram uma
predominância do genótipo gB2, tanto em sangue periférico quanto em amostras
tumorais, sendo 100% das amostras de sangue e 85% da amostras de tumor pertencentes
a este genótipo. É possível que exista uma associação deste genótipo com GBM,
entretanto, estudos prévios encontraram uma alta frequência do genótipo gB2 em
pacientes imunodeprimidos do Brasil (Aldo Albuquerque Cunha, Vitor Hugo Aquino,
Viviane Mariguela, Maurício Lacerda Nogueira, 2011; Carraro & Granato, 2003;
Correia-Silva et al., 2011; Yamamoto et al., 2007). Portanto, é mais provável que este
achado reflita a predominância deste genótipo no Brasil.
O número de cópias de DNA viral nas amostras de tumor, determinado por
qPCR, demonstrou variações. Enquanto um paciente apresentou 3,16.104cópias
pp65/célula (P6) a maioria dos pacientes apresentaram uma baixa carga viral, com uma
média de 4,77.10-3 cópias pp65/célula (P5, P13, P15, P17, P21). Em média 1 a cada 33
células contém o DNA viral, o que corresponde a uma infecção por HCMV em baixas
MOI, conforme sugerido por Ranganathan et al., 2012. As cargas virais das amostras
de sangue de pacientes com GBM e transplantados renais também foram comparadas, e
conforme mostrado na Figura 9 (b), não há diferença significativa na carga viral destes
dois tipos de amostra, com um número de cópias médio de 1,3 x 105 e 3,2 x 105 cópias
/ml em sangue de pacientes com GBM e transplantados, respectivamente.
Apesar destes dados, ainda existem várias questões quanto à correlação do
HCMV e GBM. Por exemplo, não é conhecido se a infecção por HCMV em células
tumorais é resultante de uma reativação viral in situ ou de uma reativação do vírus no
sangue periférico que é levada para os sítios tumorais por células imunes infiltrativas.
Esta reativação viral em pacientes com GBM pode ser uma consequência da
imunossupressão relacionada ao câncer ou consequência de um tratamento relacionado
à imunossupressão. Mitchel et al, 2008 propuseram que a reativação é consequência da
imunossupressão relacionada ao câncer, uma vez que os pacientes analisados em seu
estudo sofreram tratamento com corticosteróides por menos de 2 semanas antes da
cirurgia para remoção do tumor (D. a Mitchell et al., 2008). Estudos anteriores em
pacientes transplantados demonstraram que a reativação viral, devido ao tratamento
imunossupressivo, ocorre em aproximadamente 7 semanas após o transplante (Preiser et
al., 2001; Zekri et al., 2004). Os pacientes deste estudo receberam terapia com
34
corticosteróides por 1 a 4 semanas antes da remoção tumoral, reforçando a ideia de que
a reativação é consequência da imunossupressão causada pelo câncer, ao invés do
tratamento imunossupressivo. De fato, pacientes com GBM exibem uma profunda
imunossupressão relacionada ao câncer (Gomez, Hickey, Tritz, & Kruse, 2008).
Cerca de metade dos pacientes com tumores positivos não tiveram DNA viral
detectável em seu sangue, sendo assim, é possível que ocorra uma reativação viral local
nas células tumorais. De fato, HCMV apresenta tropismo para células da glia (Fritschy
et al., 1996), e tem sido mostrado que a infecção de células malignas da glia leva a
persistência viral e a produção de vírus com mutações, características relacionadas a
ausência de efeito citopático nestas células (Ogura et al., 1986). Adicionalmente, em
células de glioma com infecção latente o estímulo inflamatório leva a reativação viral
(Poland & Costello, 1990).
Utilizando-se destes resultados ainda não está claro se a imunossupressão leva a
reativação viral no sangue periférico, nas células tumorais ou em ambos e mais estudos,
levando-se em conta o tratamento dos pacientes e suas condições imunológicas, são
necessários para responder a esta questão (D. a Mitchell et al., 2008).
35
Conclusão
Os resultados apresentados neste trabalho mostram uma alta prevalência do
HCMV em amostras de GBM de uma população do Brasil, utilizando-se de técnicas
moleculares de detecção otimizadas com alto nível de sensibilidade. Técnicas de qPCR
e nPCR mostraram uma alta sensibilidade na detecção do genoma viral em amostras de
DNA total (DNA genômico e viral). Os melhores limites de detecção obtidos foram de
9 cópias/µl por nPCR e 2 cópias/µl por qPCR, com os primers para as regiões UL55 e
UL83, respectivamente. O DNA do HCMV foi detectado nas amostras clínicas de
tumor pelas duas técnicas e primers mais sensíveis: 95% por qPCR e 91% por nPCR.
Cerca de metade dos pacientes com tumores positivos para HCMV também
apresentaram DNA viral em seu sangue (47% por qPCR e 61% by nPCR). O genótipo
gB2 foi o mais prevalente encontrado, tanto nas amostras tumorais (85%) quanto nas
amostras de sangue periférico (100%), dados estes que podem refletir uma prevalência
deste genótipo no Brasil. A carga viral nas amostras de tumor mostrou-se
extremamente alta (3,16.104 cópias pp65/célula) em um paciente (P6) até extremamente
baixa (média 4,77.10-3 cópias pp65/célula) em alguns pacientes (P5, P13, P15, P17,
P21), com uma média de 1 a cada 33 células infectadas com DNA viral, indicando
prevalência de baixa carga viral nas amostras. A comparação da carga em sangue de
pacientes com GBM e transplantados renais, não demonstrou diferença significativa na
quantidade de vírus nestes dois tipos de amostra. O um número de cópias médio obtido
foi 1,3 x 105 enas amostras de sangue de pacientes com GBM e 3,2 x 105 cópias /ml
em transplantados.
Os dados obtidos neste trabalho reforçam a possível associação entre a infecção
do HCMV e o desenvolvimento do tumor e corroboram dados similares em outras
regiões do mundo.
36
Referências
Affronti, M. Lou, Heery, C. R., Herndon, J. E., Rich, J. N., Reardon, D. a, Desjardins,
A., Vredenburgh, J. J., et al. (2009). Overall survival of newly diagnosed
glioblastoma patients receiving carmustine wafers followed by radiation and
concurrent temozolomide plus rotational multiagent chemotherapy. Cancer,
115(15), 3501–11. doi:10.1002/cncr.24398
Aldo Albuquerque Cunha, Vitor Hugo Aquino, Viviane Mariguela, Maurício Lacerda
Nogueira, L. T. M. F. (2011). EVALUATION OF GLYCOPROTEIN B
GENOTYPES AND LOAD OF CMV INFECTING BLOOD, 53(2), 83–88.
doi:10.1590/S0036-46652011000200005
Arita, N., Hayakawa, T., Izumoto, S., & Al, E. (1989). Epidermal growth factor receptor
in human glioma. J Neurosurg, 70, 916–19.
Baryawno, N., Rahbar, A., Wolmer-solberg, N., Taher, C., Odeberg, J., Darabi, A.,
Khan, Z., et al. (2011). Detection of human cytomegalovirus in medulloblastomas
reveals
a
potential
therapeutic
target,
121(10),
4043–4055.
doi:10.1172/JCI57147.colon
Bergonzini, V., Salata, C., Calistri, A., Parolin, C., & Palù, G. (2010). View and review
on viral oncology research. Infectious Agents and Cancer, 5, 1–11.
Blumberg, B. S., Larouzé, B., London, W. T., Werner, B., Hesser, J. E., Millman, I.,
Saimot, G., et al. (1975). [The relation of infection with the hepatitis B-agent to
primary hepatic carcinoma (author’s transl)]. Leber, Magen, Darm, 6(6), 309–15.
Boshartb, M., Gissmann, L., Ikenberg, H., Kleinheinzl, A., Scheurlen, W., & Hausen,
H. (1984). A new type of papillomavirus DNA, its presence in genital cancer
biopsies and in cell lines derived from cervical cancer. EMBO J, 3(5), 1151–1157.
Bresnahan, W. a, & Shenk, T. (2000). A subset of viral transcripts packaged within
human cytomegalovirus particles. Science (New York, N.Y.), 288(5475), 2373–6.
37
Britt, W. J., & Auger, D. (1986). Synthesis and Processing of the Envelope gp55-116
Complex of Human Cytomegalovirus, 58(1), 185–191.
Carraro, E., & Granato, C. F. H. (2003). Single human cytomegalovirus gB genotype
shed in multiple sites at the time of diagnosis in renal transplant recipients. Journal
of medical virology, 70(2), 240–3. doi:10.1002/jmv.10383
Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS, Liang DC, S. W., & DS, C.
(1997). H E PAT I T I S B VACCINAT ION IN TAIWAN AN D TH E INC ID
ENC E OF H EPATOC ELLUL A R CA RCINOMA IN CH ILD REN
UNIVERSAL HEPATITIS B VACCINATION IN TAIWAN AND THE
INCIDENCE OF HEPATOCELLULAR CARCINOMA IN CHILDREN. N Engl J
Med, 336, 1855–1859.
Choe, G., Horvath, S., Cloughesy, T. F., Crosby, K., Seligson, D., Palotie, A., Inge, L.,
et al. (2003). Advances in Brief Analysis of the Phosphatidylinositol 3 -Kinase
Signaling Pathway in Glioblastoma Patients in Vivo 1. Cancer Research, 63,
2742–2746.
Choo, Q., Kuo, G., Weiner, A., Overby, L., Bradley, D., & Houghton, M. (1989).
Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis
genome. Science, 244, 359–62.
Chou, S., & Dennison, K. (1991). Analysis of interstrain variation in cytomegalovirus
glycoprotein B sequences encoding neutralization-related epitopes. Journal of
Infectious Diseases, 1229–34.
Chung, R., & Seizinger, R. (1991). Tumor suppressor genes and cancer of the human
nervous system. Cancer Investigation, 9, 429–38.
Cinatl, J., Scholz, M., & Doerr, H. W. (2005). Role of tumor cell immune escape
mechanisms in cytomegalovirus-mediated oncomodulation. Medicinal research
reviews, 25(2), 167–85. doi:10.1002/med.20018
38
Cinatl Jr, J., Cinatl, J., Vogel, J., Rabenau, H., Kornhuber, B., & Doerr, H. . (1996).
Modulatory Effects of Human Cytomegalovirus Infection on Malignant Properties
of Cancer Cells. Intervirology, 39, 259–69.
Cobbs, C. S., Harkins, L., Samanta, M., Gillespie, G. Y., Bharara, S., King, P. H.,
Nabors, L. B., et al. (2002). Human cytomegalovirus infection and expression in
human malignant glioma. Cancer Research, 45(6), 2900–2906.
Colombo, M., Kuo, G., Choo, Q., Donato, M., Del Ninno, E., Tommasini, M.,
Dioguardi, N., et al. (1989). Prevalence of antibodies to hepatitis C virus in Italian
patients with hepatocellular carcinoma. Lancet, 2, 1006–8.
Compton, T, Nowlin, D. M., & Cooper, N. R. (1993). Initiation of human
cytomegalovirus infection requires initial interaction with cell surface heparan
sulfate. Virology, 193(2), 834–41. doi:10.1006/viro.1993.1192
Compton, Teresa, Nepomuceno, R. R., & Nowlin, D. M. (1992). Human
cytomegalovirus penetrates host cells by PH-independent fusion at the cell surface.
Virology, 191(1), 387–395. doi:10.1016/0042-6822(92)90200-9
Correia-Silva, J. F., Resende, R. G., Arão, T. C., Abreu, M. H. N. G., Teixeira, M. M.,
Bittencourt, H., Silva, T. a, et al. (2011). HCMV gB genotype and its association
with cytokine levels in hematopoietic stem cell transplantation. Oral diseases,
17(5), 530–7. doi:10.1111/j.1601-0825.2011.01801.x
Courcelle, C. T., Courcelle, J., Prichard, M. N., & Mocarski, E. S. (2001). Requirement
for uracil-DNA glycosylase during the transition to late-phase cytomegalovirus
DNA
replication.
Journal
of
virology,
75(16),
7592–601.
doi:10.1128/JVI.75.16.7592-7601.2001
Cunha, A. D. A., Marin, L. J., Aquino, V. H., & Figueiredo, L. T. M. (2002). Diagnosis
of cytomegalovirus infections by qualitative and quantitative PCR in HIV infected
patients. Revista do Instituto de Medicina Tropical de São Paulo, 44(3), 127–32.
39
Dal Monte, P., Bessia, C., Landini, M. P., & Michelson, S. (1996). Expression of human
cytomegalovirus ppUL83 (pp65) in a stable cell line and its association with
metaphase chromosomes. The Journal of general virology, 77 ( Pt 10, 2591–6.
Davison, a. J. (2003). The human cytomegalovirus genome revisited: comparison with
the chimpanzee cytomegalovirus genome. Journal of General Virology, 84(1), 17–
28. doi:10.1099/vir.0.18606-0
De Campos Dieamant, D., Bonon, S. H. A., Prates, L. C., Belangelo, V. M. S., Pontes,
E. R., & Costa, S. C. B. (2010). Active human cytomegalovirus infection and
glycoprotein b genotypes in brazilian pediatric renal or hematopoietic stem cell
transplantation patients. Brazilian journal of microbiology : [publication of the
Brazilian
Society
for
Microbiology],
41(1),
50–8.
doi:10.1590/S1517-
838220100001000010
Dimberg, J., Hong, T. T., Skarstedt, M., Löfgren, S., Zar, N., & Matussek, A. (2013).
Detection of cytomegalovirus DNA in colorectal tissue from Swedish and
vietnamese patients with colorectal cancer. Anticancer research, 33(11), 4947–50.
Doniger, J., Muralidhar, S., & Rosenthal, L. J. (1999). Human cytomegalovirus and
human herpesvirus 6 genes that transform and transactivate. Clinical microbiology
reviews, 12(3), 367–82.
Dos Santos, C. J., Stangherlin, L. M., Figueiredo, E. G., Corrêa, C., Teixeira, M. J., &
Da Silva, M. C. C. (2013). High prevalence of HCMV and viral load in tumor
tissues and peripheral blood of glioblastoma multiforme patients. Journal of
medical virology. doi:10.1002/jmv.23820
Dürst, M., Gissmann, L., Ikenberg, H., & Zur Hausen, H. (1983). A papillomavirus
DNA from a cervical carcinoma and its prevalence in cancer biopsy samples from
different geographic regions. Proceedings of the National Academy of Sciences of
the United States of America, 80(12), 3812–5.
Dziurzynski, K., Chang, S. M., Heimberger, A. B., Kalejta, R. F., McGregor Dallas, S.
R., Smit, M., Soroceanu, L., et al. (2012). Consensus on the role of human
40
cytomegalovirus
in
glioblastoma.
Neurooncology,
14(3),
246–255.
doi:10.1093/neuonc/nor227
El-Shinawi, M., & Mohamed, H. (2013). Human Cytomegalovirus Infection Enhances
NF-ÎoB/p65 Signaling in Inflammatory Breast Cancer Patients. PloS one, 8(2),
e55755. doi:10.1371/journal.pone.0055755
Epstein, M. A., Achong, B. G. & Barr, Y. M. (1964). Virus particles in cultured
lymphoblasts from Burkitt’s lymphoma. Lancet, 15, 702–703.
Feldkamp, M., Lala, P., Lau, N., & Al, E. (1999). Expression of activated epidermal
growth factor receptors, ras-guanosine triphosphate, and mitogen-activated protein
kinase in human glioblastoma multiforme specimens. Neurosurgery, 45(6), 1442.
Feng H, Shuda M, Chang Y, M. P. (2008). Clonal Integration of a Polyomavirus in
Human
Merkel
Cell
Carcinoma.
Science,
319(5866),
1096–1100.
doi:10.1126/science.1152586.Clonal
Fonseca, R., & Kawamura, M. (2012). The prevalence of human cytomegalovirus DNA
in gliomas of Brazilian patients. Memórias do Instituto Oswaldo Cruz, 107, 953–
954.
Frederick, L., Wang, X. Y., Eley, G., & James, C. D. (2000). Diversity and frequency of
epidermal growth factor receptor mutations in human glioblastomas. Cancer
research, 60(5), 1383–7.
Fries, B. C., Chou, S., Boeckh, M., & Torok-Storb, B. (1994). Frequency distribution of
cytomegalovirus envelope glycoprotein genotypes in bone marrow transplant
recipients. The Journal of infectious diseases, 169(4), 769–74.
Fritschy, J. M., Brandner, S., Aguzzi, a, Koedood, M., Luscher, B., & Mitchell, P. J.
(1996). Brain cell type specificity and gliosis-induced activation of the human
cytomegalovirus immediate-early promoter in transgenic mice. The Journal of
neuroscience : the official journal of the Society for Neuroscience, 16(7), 2275–82.
41
Gaytant, M. A., Steegers, E. A. P., Semmekrot, B. A., Merkus, H. M. M. W., &
Galama, J. M. D. (2002). Congenital Cytomegalovirus Infection :Review of the
Epidemology and Outcome. Obstretical and Gynecological Survey, 57(4), 245–56.
Geder, K., Lausch, R., O’Neill, F., & Rapp, F. (1976). Oncogenic transformation of
human embryo lung cells by human cytomegalovirus. Science, 192(4244), 1134–
1137. doi:10.1126/science.179143
Gilbert, C., & Boivin, G. (2005). Human Cytomegalovirus Resistance to Antiviral
Drugs MINIREVIEW Human Cytomegalovirus Resistance to Antiviral Drugs.
ANTIMICROBIAL
AGENTS
AND
CHEMOTHERAPY,
49(3),
873–883.
doi:10.1128/AAC.49.3.873
Gilbertson, D. G., Duff, M. E., West, J. W., Kelly, J. D., Sheppard, P. O., Hofstrand, P.
D., Gao, Z., et al. (2001). Platelet-derived growth factor C (PDGF-C), a novel
growth factor that binds to PDGF alpha and beta receptor. The Journal of
biological chemistry, 276(29), 27406–14. doi:10.1074/jbc.M101056200
Goldmacher, V. S., Bartle, L. M., Skaletskaya, a, Dionne, C. a, Kedersha, N. L., Vater,
C. a, Han, J. W., et al. (1999). A cytomegalovirus-encoded mitochondria-localized
inhibitor of apoptosis structurally unrelated to Bcl-2. Proceedings of the National
Academy of Sciences of the United States of America, 96(22), 12536–41.
Gomez, G. G., Hickey, M. J., Tritz, R., & Kruse, C. A. (2008). Immunoresistant human
gliomas cell clones selected with alloreactive cytotoxic T lymphocytes. Gene Ther
Mol Biol, 12(1), 101–110.
Görzer, I., Kerschner, H., Redlberger-Fritz, M., & Puchhammer-Stöckl, E. (2010).
Human cytomegalovirus (HCMV) genotype populations in immunocompetent
individuals during primary HCMV infection. Journal of clinical virology : the
official publication of the Pan American Society for Clinical Virology, 48(2), 100–
3. doi:10.1016/j.jcv.2010.03.005
Greijer, a E., Van de Crommert, J. M., Stevens, S. J., & Middeldorp, J. M. (1999).
Molecular
fine-specificity
analysis
of
antibody
responses
to
human
42
cytomegalovirus and design of novel synthetic-peptide-based serodiagnostic
assays. Journal of clinical microbiology, 37(1), 179–88.
Guha, a, Feldkamp, M. M., Lau, N., Boss, G., & Pawson, a. (1997). Proliferation of
human malignant astrocytomas is dependent on Ras activation. Oncogene, 15(23),
2755–65.
Guha, A., Dashner, K., Black, P., Wagner, J., & Stiles, C. (1995). Expression of PDGF
and PDGF receptors in human astrocytoma operation specimens supports the
existence of an autocrine loop. Int J Cancer, 60, 168–73.
Hagemeier, C., Caswell, R., Hayhurst, G., Sinclair, J., & Kouzarides, T. (1994).
Functional interaction between the HCMV IE2 transactivator and the
retinoblastoma protein. The EMBO journal, 13(12), 2897–903.
Hanahan, D., & Weinberg, R. a. (2011). Hallmarks of cancer: the next generation. Cell,
144(5), 646–674. doi:10.1016/j.cell.2011.02.013
Harkins, L., Volk, A. L., Samanta, M., Mikolaenko, I., Britt, W. J., Bland, K. I., &
Cobbs, C. S. (2002). Specific localisation of human cytomegalovirus nucleic acids
and proteins in human colorectal cancer. Zeitschrift fur Gastroenterologie,
41(9345), 881–882.
Heimberger, A. B., Wang, E., McGary, E. C., Hess, K. R., Henry, V. K., Shono, T.,
Cohen, Z., et al. (2005). Mechanisms of action of rapamycin in gliomas. Neurooncology, 7(1), 1–11. doi:10.1215/S1152851704000420
Hilleman, M. (2003). Critical overview and outlook: pathogenesis, prevention, and
treatment of hepatitis and hepatocarcinoma caused by hepatitis B virus. accine, 21,
4626–49.
Hinuma, Y., Nagata, K., Hanaoka, M., Nakai, M., Matsumoto, T., Kinoshita, K. I.,
Shirakawa, S., et al. (1981). Adult T-cell leukemia: antigen in an ATL cell line and
detection of antibodies to the antigen in human sera. Proceedings of the National
Academy of Sciences of the United States of America, 78(10), 6476–80.
43
Holland, E. C. (2000). Glioblastoma multiforme: the terminator. Proceedings of the
National Academy of Sciences of the United States of America, 97(12), 6242–4.
Hume, A. J., Finkel, J. S., Kamil, J. P., Coen, D. M., Culbertson, M. R., & Kalejta, R. F.
(2008). Phosphorylation of retinoblastoma protein by viral protein with cyclindependent kinase function. Science (New York, N.Y.), 320(5877), 797–9.
doi:10.1126/science.1152095
Isaacson, M. K., & Compton, T. (2009). Human cytomegalovirus glycoprotein B is
required for virus entry and cell-to-cell spread but not for virion attachment,
assembly, or egress. Journal of virology, 83(8), 3891–903. doi:10.1128/JVI.0125108
Jin, H., & Li, S. (2007). Genotype Correlates with Different, 110001(92), 219–223.
doi:10.1159/000100564
Kalejta, R. F., & Shenk, T. (2003). degradation of the Rb family of tumor suppressors
by the human cytomegalovirus pp71 protein. Proceedings of the National Academy
of Sciences of the United States of America, 130(6), 3263–8.
Kleihues P, Louis DN, Scheithauer BW, Rorke LB, Reifenberger G, Burger PC, C. W.
(2002). The WHO classification of tumors of the nervous system. J Neuropathol
Exp Neurol., 61, 215–25.
Kneifel, S., Cordier, D., Good, S., Ionescu, M. C. S., Ghaffari, A., Hofer, S.,
Kretzschmar, M., et al. (2006). Local targeting of malignant gliomas by the
diffusible peptidic vector 1,4,7,10-tetraazacyclododecane-1-glutaric acid-4,7,10triacetic acid-substance p. Clinical cancer research : an official journal of the
American Association for Cancer Research, 12(12), 3843–50. doi:10.1158/10780432.CCR-05-2820
Komatsu, T. E., Pikis, A., Naeger, L. K., & Harrington, P. R. (2013). Resistance of
human cytomegalovirus to ganciclovir/valganciclovir: A comprehensive review of
putative
resistance
pathways.
Antiviral
research,
101C,
12–25.
doi:10.1016/j.antiviral.2013.10.011
44
LaRochelle, W., Jeffers, M., McDonald, W., & Al, E. (2001). PDGF-D, a new proteaseactivated growth factor. Nat Cell Biol, 3, 517–21.
Lau, S. K., Chen, Y.-Y., Chen, W.-G., Diamond, D. J., Mamelak, A. N., Zaia, J. a, &
Weiss, L. M. (2005). Lack of association of cytomegalovirus with human brain
tumors. Modern pathology : an official journal of the United States and Canadian
Academy of Pathology, Inc, 18(6), 838–43. doi:10.1038/modpathol.3800352
Lehrer, S., & Labombardi, V. (2011). No circulating cytomegalovirus in five patients
with glioblastoma multiforme. Anticancer Research, 3, 959–60.
Limaye, A. P. (2002). Ganciclovir-resistant cytomegalovirus in organ transplant
recipients. Clinical infectious diseases : an official publication of the Infectious
Diseases Society of America, 35(7), 866–72. doi:10.1086/342385
Lokker, N. A., Sullivan, C. M., Hollenbach, S. J., Israel, M. A., & Giese, N. A. (2002).
Platelet-derived Growth Factor ( PDGF ) Autocrine Signaling Regulates Survival
and Mitogenic Pathways in Glioblastoma Cells : Evidence That the Novel PDGF-C
and PDGF-D Ligands May Play a Role in the Development of Brain Tumors
Platelet-derived Growth Fact.
Louis, D. N. (2006). Molecular pathology of malignant gliomas. Annual review of
pathology, 1, 97–117. doi:10.1146/annurev.pathol.1.110304.100043
Lucas, K. G., Bao, L., Bruggeman, R., Dunham, K., & Specht, C. (2011). The detection
of CMV pp65 and IE1 in glioblastoma multiforme. Journal of neurooncology,
103(2), 231–238. doi:10.1007/s11060-010-0383-6
Ma, Y., Wang, N., Li, M., Gao, S., Wang, L., Zheng, B., Qi, Y., et al. (2012). Human
CMV
transcripts:
an
overview.
Future
microbiology,
7(5),
577–93.
doi:10.2217/fmb.12.32
Madi, N., Al-Nakib, W., Pacsa, A., & Saeed, T. (2011). Cytomegalovirus genotypes
gB1 and gH1 are the most predominant genotypes among renal transplant
recipients
in
Kuwait.
Transplantation
proceedings,
43(5),
1634–7.
doi:10.1016/j.transproceed.2011.02.053
45
Maehama, T., & Dixon, J. E. (1998). The Tumor Suppressor, PTEN/MMAC1,
Dephosphorylates the Lipid Second Messenger, Phosphatidylinositol 3,4,5Trisphosphate. The Journal of Biological Chemistry, 273, 13375–13378.
Maher, E. A., Furnari, F. B., Bachoo, R. M., Rowitch, D. H., Louis, D. N., Cavenee, W.
K., & Depinho, R. A. (2001). Malignant glioma : genetics and biology of a grave
matter, 1311–1333. doi:10.1101/gad.891601.Godlee
Marumoto, T., & Saya, H. (2012). Molecular biology of glioma. Advances in
experimental medicine and biology, 746, 2–11. doi:10.1007/978-1-4614-3146-6_1
Maussang, D., Verzijl, D., Van Walsum, M., Leurs, R., Holl, J., Pleskoff, O., Michel,
D., et al. (2006). Human cytomegalovirus-encoded chemokine receptor US28
promotes tumorigenesis. Proc Natl Acad Sci U S A, 103(35), 13068–13073.
Melnick, M., Deluca, K. a, Sedghizadeh, P. P., & Jaskoll, T. (2013). Cytomegalovirusinduced salivary gland pathology: AREG, FGF8, TNF-α, and IL-6 signal
dysregulation and neoplasia. Experimental and molecular pathology, 94(2), 386–
97. doi:10.1016/j.yexmp.2013.01.005
Meyer-König, U., Vogelberg, C., Bongarts, A., Kampa, D., Delbrück, R., WolffVorbeck, G., Kirste, G., et al. (1998). Glycoprotein B genotype correlates with cell
tropism in vivo of human cytomegalovirus infection. Journal of medical virology,
55(1), 75–81.
Michaelis, M., Doerr, H. W., & Cinatl, J. (2009). Oncomodulation by human
cytomegalovirus: evidence becomes stronger. Medical microbiology and
immunology, 198(2), 79–81. doi:10.1007/s00430-009-0107-8
Mitchell, D. a, Xie, W., Schmittling, R., Learn, C., Friedman, A., McLendon, R. E., &
Sampson, J. H. (2008). Sensitive detection of human cytomegalovirus in tumors
and peripheral blood of patients diagnosed with glioblastoma. Neurooncology,
10(1), 10–18. doi:10.1215/15228517-2007-035
Mitchell, D. P., Savaryn, J. P., Moorman, N. J., Shenk, T., Terhune, S. S., Al, M. E. T.,
& Irol, J. V. (2009). Human Cytomegalovirus UL28 and UL29 Open Reading
46
Frames Encode a Spliced mRNA and Stimulate Accumulation of, 83(19), 10187–
10197. doi:10.1128/JVI.00396-09
Mocarski, E. S., Shenk, T., & Pass, R. F. (2006). Cytomegalovirus. In Bernard N Fields;
David M Knipe; Peter M Howley; et (Ed.), Fields of virology (4th ed., pp. 2702 –
2772). Philadelphia : Wolters Kluwer Health/Lippincott Williams & Wilkins.
Moore, P. S., & Chang, Y. (2010). Why do viruses cause cancer? Highlights of the first
century of human tumour virology. Nature Reviews Cancer, 10(12), 878–889.
Newton, H. B. (1994). Primary brain tumors: review of etiology, diagnosis and
treatment. Am Fam Physician., 49, 787–97.
Newton, H. B. (2006). Clinical pharmacology of brain tumor chemotherapy. In H. B.
Newton (Ed.), Handbook of brain tumor chemotherapy (Elsevier/A., pp. 21–43).
London.
Newton, H. B. (2010). Glioblastoma-Molecular Mechanisms of Pathogenesis and
Current Therapeutic Strategies. In S. K. Ray (Ed.), (pp. 1–42). doi:10.1007/978-14419-0410-2
Newton, H. B., Turowski, R., TJ, S., & Al, E. (1999). Clinical presentation, diagnosis,
and pharmacotherapy of patients with primary brain tumors. Ann Pharmacother,
33, 816–32.
Normanno, N., De Luca, A., Bianco, C., Strizzi, L., Mancino, M., Maiello, M. R.,
Carotenuto, A., et al. (2006). Epidermal growth factor receptor (EGFR) signaling
in cancer. Gene, 366(1), 2–16. doi:10.1016/j.gene.2005.10.018
Ogawa-Goto, K., Tanaka, K., Gibson, W., Moriishi, E., Miura, Y., Kurata, T., Irie, S., et
al. (2003). Microtubule Network Facilitates Nuclear Targeting of Human
Cytomegalovirus
Capsid.
Journal
of
Virology,
77(15),
8541–8547.
doi:10.1128/JVI.77.15.8541–8547.2003
Ogura, T., Tanaka, J., Kamiya, S., Sato, H., Ogura, H., & Hatano, M. (1986). Human
cytomegalovirus persistent infection in a human central nervous system cell line:
47
production of a variant virus with different growth characteristics. The Journal of
general virology, 67 ( Pt 12, 2605–16.
Ohgaki, H. (2009). Epidemiology of brain tumors. In M. Verma (Ed.), Neurologic
clinics (pp. 323–342). Humana Press.
Paradowska, E., Studzińska, M., Nowakowska, D., Wilczyński, J., Rycel, M., Suski, P.,
Gaj, Z., et al. (2012). Distribution of UL144, US28 and UL55 genotypes in Polish
newborns with congenital cytomegalovirus infections. European journal of clinical
microbiology & infectious diseases : official publication of the European Society of
Clinical Microbiology, 31(7), 1335–45. doi:10.1007/s10096-011-1447-z
Poiesz, B. J., Ruscetti, F. W., Gazdar, a F., Bunn, P. a, Minna, J. D., & Gallo, R. C.
(1980). Detection and isolation of type C retrovirus particles from fresh and
cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proceedings of
the National Academy of Sciences of the United States of America, 77(12), 7415–9.
Poland, S., & Costello, P. (1990). Cytomegalovirus in the brain: in vitro infection of
human brain-derived cells. Journal of Infectious ….
Poltermann, S., Schlehofer, B., Steindorf, K., Schnitzler, P., Geletneky, K., &
Schlehofer, J. R. (2006). Lack of association of herpesviruses with brain tumors.
Journal of NeuroVirology, 13(2), 90–99. doi:10.1080/13550280600654573
Poma, E. E., Kowalik, T. F., Zhu, L., Sinclair, J. H., & Huang, E. S. (1996). The human
cytomegalovirus IE1-72 protein interacts with the cellular p107 protein and
relieves p107-mediated transcriptional repression of an E2F-responsive promoter.
Journal of virology, 70(11), 7867–77.
Preiser, W., Bräuninger, S., Schwerdtfeger, R., Ayliffe, U., Garson, J. a, Brink, N. S.,
Franck, S., et al. (2001). Evaluation of diagnostic methods for the detection of
cytomegalovirus in recipients of allogeneic stem cell transplants. Journal of
clinical virology : the official publication of the Pan American Society for Clinical
Virology, 20(1-2), 59–70.
48
Price RL, Bingmer K, Harkins L, Iwenofu OH, Kwon CH, Cook C, Pelloski C, C. E.
(2012). Cytomegalovirus infection leads to pleomorphic rhabdomyosarcomas in
Trp53+/- mice. Cancer Res., 15(62), 5669–74.
Pytel, P., & Lukas, R. V. (2009). Update on diagnostic practice: tumors of the nervous
system. Archives of pathology & laboratory medicine, 133(7), 1062–77.
doi:10.1043/1543-2165-133.7.1062
Rahbar, A., Orrego, A., Peredo, I., Dzabic, M., Wolmer-Solberg, N., Strååt, K.,
Stragliotto, G., et al. (2013). Human cytomegalovirus infection levels in
glioblastoma multiforme are of prognostic value for survival. Journal of clinical
virology : the official publication of the Pan American Society for Clinical
Virology, 9–12. doi:10.1016/j.jcv.2012.12.018
Rahbar, A., Stragliotto, G., Orrego, A., Peredo, I., Taher, C., Willems, J., & SöderbergNaucler, C. (2012). Low levels of Human Cytomegalovirus Infection in
Glioblastoma multiforme associates with patient survival; -a case-control study.
Herpesviridae, 3(1), 3. doi:10.1186/2042-4280-3-3
Ramirez, Y. P., Weatherbee, J. L., Wheelhouse, R. T., & Ross, A. H. (2013).
Glioblastoma
Multiforme
Therapy
and
Mechanisms
of
Resistance.
Pharmaceuticals (Basel, Switzerland), 6(12), 1475–1506. doi:10.3390/ph6121475
Ranganathan, P., Clark, P. a, Kuo, J. S., Salamat, M. S., & Kalejta, R. F. (2012).
Significant association of multiple human cytomegalovirus genomic Loci with
glioblastoma multiforme samples.
Journal
of
Virology,
86(2), 854–64.
doi:10.1128/JVI.06097-11
Renzette, N., Bhattacharjee, B., Jensen, J. D., Gibson, L., & Kowalik, T. F. (2011).
Extensive genome-wide variability of human cytomegalovirus in congenitally
infected
infants.
PLoS
pathogens,
7(5),
e1001344.
doi:10.1371/journal.ppat.1001344
Rong, Y., & Brat, D. J. (2009). Vaso-occlusive Mechanisms that Intiate Hypoxia and
Necrosis in Glioblastoma: The Role of Thrombosis and Tissue Factor. In E. G.
Meir (Ed.), CNS Cancer: Models, Markers, Prognostic Factors, Targets, and
49
Therapeutic
Approaches
(pp.
507–528).
Totowa,
NJ:
Humana
Press.
doi:10.1007/978-1-60327-553-8
Roubalová, K., Strunecký, O., Zufanová, S., Procházka, B., & Vitek, A. (2010).
[Genotyping of viral glycoprotein B (gB) in hematopoietic stem cell transplant
recipients with active cytomegalovirus infection: analysis of the impact of gB
genotypes on the patients’ outcome]. Epidemiologie, mikrobiologie, imunologie :
casopis Spolecnosti pro epidemiologii a mikrobiologii Ceské lékarské spolecnosti
J.E. Purkyne, 59(2), 92–9.
Sabatier, J., Uro-Coste, E., Pommepuy, I., Labrousse, F., Allart, S., Trémoulet, M.,
Delisle, M. B., et al. (2005). Detection of human cytomegalovirus genome and
gene products in central nervous system tumours. British Journal of Cancer, 92(4),
747–750. doi:10.1038/sj.bjc.6602339
Sakata, K., Kato, S., Fox, J., & Al, E. (2002). Autocrine signaling through ras regulates
cell survival activity in human glioma cells: Potential cross-talk between ras and
the phosphotadylinositol 3-kinase-Akt pathway. J Neuropathol Exp Neurol., 61,
975–83.
Samanta, M., Harkins, L., Klemm, K., Britt, W. J., & Cobbs, C. S. (2003). High
prevalence of human cytomegalovirus in prostatic intraepithelial neoplasia and
prostatic
carcinoma.
The
Journal
of
urology,
170(3),
998–1002.
doi:10.1097/01.ju.0000080263.46164.97
Sanchez, V., Sztul, E., & Britt, W. J. (2000). Human cytomegalovirus pp28 (UL99)
localizes to a cytoplasmic compartment which overlaps the endoplasmic reticulumgolgi-intermediate compartment. Journal of virology, 74(8), 3842–51.
Sarcinella, L., Mazzulli, T., Willey, B., & Humar, A. (2002). Cytomegalovirus
glycoprotein B genotype does not correlate with outcomes in liver transplant
patients. Journal of clinical virology : the official publication of the Pan American
Society for Clinical Virology, 24(1-2), 99–105.
50
Scheurer, M. E., Bondy, M. L., Aldape, K. D., & Albrecht, T. (2010). Detection of
Human Cytomegalovirus in Different Histological Types of gliomas. Acta
Neuropathol., 116(1), 79–86. doi:10.1007/s00401-008-0359-1.Detection
Shapiro, J., & Coons, S. (1998). Genetics of adult malignant gliomas. BNI Q, 14, 27–34.
Shepp, D. H., Match, M. E., Ashraf, a B., Lipson, S. M., Millan, C., & Pergolizzi, R.
(1996). Cytomegalovirus glycoprotein B groups associated with retinitis in AIDS.
The Journal of infectious diseases, 174(1), 184–7.
Silva, M. C., Yu, Q., Enquist, L., & Shenk, T. (2003). Human Cytomegalovirus UL99Encoded pp28 Is Required for the Cytoplasmic Envelopment of TegumentAssociated Capsids, 77(19), 10594–10605. doi:10.1128/JVI.77.19.10594
Sinclair, J., & Sissons, P. (2006). Latency and reactivation of human cytomegalovirus.
The Journal of general virology, 87(Pt 7), 1763–79. doi:10.1099/vir.0.81891-0
Skaletskaya, a, Bartle, L. M., Chittenden, T., McCormick, a L., Mocarski, E. S., &
Goldmacher, V. S. (2001). A cytomegalovirus-encoded inhibitor of apoptosis that
suppresses caspase-8 activation. Proceedings of the National Academy of Sciences
of the United States of America, 98(14), 7829–34. doi:10.1073/pnas.141108798
Slinger, E., Maussang, D., Schreiber, A., Siderius, M., Rahbar, A., Fraile-Ramos, A.,
Lira, S. a, et al. (2010). HCMV-encoded chemokine receptor US28 mediates
proliferative signaling through the IL-6-STAT3 axis. Science signaling, 3(133),
ra58. doi:10.1126/scisignal.2001180
Söderberg-Nauclér, C. (2008). HCMV microinfections in inflammatory diseases and
cancer. Journal of clinical virology the official publication of the Pan American
Society for Clinical Virology, 41(3), 218–223. doi:10.1016/j.jcv.2007.11.009
Soroceanu, L., Matlaf, L., Bezrookove, V., Harkins, L., Martinez, R., Greene, M.,
Soteropoulos, P., et al. (2011). Human cytomegalovirus US28 found in
glioblastoma promotes an invasive and angiogenic phenotype. Cancer Research,
71(21), 6643–53. doi:10.1158/0008-5472.CAN-11-0744
51
Stagno, S., & Whitley, R. J. (1985). Herpesvirus infections of pregnancy. Part I:
Cytomegalovirus and Epstein-Barr virus infections. The New England journal of
medicine, 313(20), 1270–4. doi:10.1056/NEJM198511143132006
Strååt, K., Liu, C., Rahbar, A., Zhu, Q., Liu, L., Wolmer-Solberg, N., Lou, F., et al.
(2009). Activation of telomerase by human cytomegalovirus. Journal Of The
National Cancer Institute, 101(7), 488–497. doi:10.1093/jnci/djp031
Tan, A., Yeh, S.-H., Liu, C.-J., Cheung, C., & Chen, P.-J. (2008). Viral
hepatocarcinogenesis: from infection to cancer. Liver international : official
journal of the International Association for the Study of the Liver, 28(2), 175–88.
doi:10.1111/j.1478-3231.2007.01652.x
Tanaka, K., Zou, J.-P., Takeda, K., Ferrans, V. J., Sandford, G. R., Johnson, T. M.,
Finkel, T., et al. (1999). Effects of Human Cytomegalovirus Immediate-Early
Proteins on p53-mediated Apoptosis in Coronary Artery Smooth Muscle Cells.
Circulation, 99(13), 1656–1659. doi:10.1161/01.CIR.99.13.1656
Tanaka, Kaori, Numazaki, K., & Tsutsumi, H. (2005). Human cytomegalovirus genetic
variability in strains isolated from Japanese children during 1983-2003. Journal of
medical virology, 76(3), 356–60. doi:10.1002/jmv.20366
Tarrago, D., Quereda, C., & Tenorio, A. (2003). Different Cytomegalovirus
Glycoprotein B Genotype Distribution in Serum and Cerebrospinal Fluid
Specimens Determined by a Novel Multiplex Nested PCR, 41(7), 2872–2877.
doi:10.1128/JCM.41.7.2872
Terhune, S., Torigoi, E., Moorman, N., Silva, M., Qian, Z., Shenk, T., & Yu, D. (2007).
Human cytomegalovirus UL38 protein blocks apoptosis. Journal of virology,
81(7), 3109–23. doi:10.1128/JVI.02124-06
Trincado, D. E., Scott, G. M., White, P. a, Hunt, C., Rasmussen, L., & Rawlinson, W.
D. (2000). Human cytomegalovirus strains associated with congenital and perinatal
infections. Journal of medical virology, 61(4), 481–7.
52
Varnum, S., Streblow, D., & Monroe, M. (2004). Identification of proteins in human
cytomegalovirus (HCMV) particles: the HCMV proteome. Journal of …, 78(20),
10960–10966. doi:10.1128/JVI.78.20.10960
Vogel, J.-U., Otte, J., Koch, F., Gümbel, H., Doerr, H. W., & Cinatl, J. (2013). Role of
human cytomegalovirus genotype polymorphisms in AIDS patients with
cytomegalovirus retinitis. Medical microbiology and immunology, 202(1), 37–47.
doi:10.1007/s00430-012-0244-3
Von Deimling, A., Louis, D., & Wiestler, O. (1995). Molecular pathways in the
formation of gliomas. Glia, 15, 328–38.
Wang, X., Huong, S.-M., Chiu, M. L., Raab-Traub, N., & Huang, E.-S. (2003).
Epidermal growth factor receptor is a cellular receptor for human cytomegalovirus.
Nature, 424(6947), 456–61. doi:10.1038/nature01818
Westermark, B., Heldin, C., & Nister, M. (1995). Platelet-derived growth factor in
human glioma. Glia1, 15, 257–63.
Wolmer-Solberg, N., Baryawno, N., Rahbar, A., Fuchs, D., Odeberg, J., Taher, C.,
Wilhelmi, V., et al. (2013). Frequent detection of human cytomegalovirus in
neuroblastoma: a novel therapeutic target? International journal of cancer. Journal
international du cancer, 133(10), 2351–61. doi:10.1002/ijc.28265
Wu, X., Wang, Y., Xu, Y., Wu, D., Sun, A., Zhu, Z., Han, Y., et al. (2010).
Cytomegalovirus glycoprotein B genotype in hematopoietic stem cell transplant
patients from China. Biology of blood and marrow transplantation journal of the
American Society for Blood and Marrow Transplantation, 16(5), 647–652.
doi:10.1016/j.bbmt.2009.12.001
Wu, Y., Yan, J., Ojcius, D. M., Chen, L., Gu, Z., Pan, J., & Icrobiol, J. C. L. I. N. M.
(2007). Correlation between Infections with Different Genotypes of Human
Cytomegalovirus and Epstein-Barr Virus in Subgingival Samples and Periodontal
Status of Patients ᰔ, 45(11), 3665–3670. doi:10.1128/JCM.00374-07
53
Yamamoto, A. Y., Mussi-pinhata, M. M., Mara, V., Wagatsuma, D. D., Marin, L. J., &
Duarte, G. (2007). Human Cytomegalovirus Glycoprotein B Genotypes in
Brazilian Mothers and Their Congenitally Infected Infants, 1168(April), 1164–
1168. doi:10.1002/jmv
Zafiropoulos, A., Tsentelierou, E., Billiri, K., & Spandidos, D. (2003). Human herpes
viruses in non-melanoma skin cancers. Cancer letters, 198(1), 77–81.
doi:10.1016/S0304-3835(03)00269-6
Zekri, A.-R. N., Mohamed, W. S., Samra, M. a, Sherif, G. M., El-Shehaby, A. M. R., &
El-Sayed, M. H. (2004). Risk factors for cytomegalovirus, hepatitis B and C virus
reactivation after bone marrow transplantation. Transplant immunology, 13(4),
305–11. doi:10.1016/j.trim.2004.10.001
Zhao, C. X. X., & Zheng, Y. S. (2012). B Genotypes in Chinese Hematopoietic Stem
Cell Transplant Recipients, 342–348. doi:10.1159/000330303
Zur Hausen, H. (1976). Condylomata Acuminata and Human Genital Cancer
Condylomata Acuminata and Human Genital Cancer. Cancer Research, 36, 794.
Zur Hausen, H. (2002). Papillomaviruses and cancer: from basic studies to clinical
application. Nat Rev Cancer 2002, 2, 342–50.
Zur Hausen, H. (2008). Novel human polyomaviruses--re-emergence of a well known
virus family as possible human carcinogens. International journal of cancer.
Journal international du cancer, 123(2), 247–50. doi:10.1002/ijc.23620
54
Anexos
Sequências obtidas durante o trabalho
Tumor
>Paciente_1_tumor_gB3
GTGACTGGACGTTTGGCATAGCTCCGGTGTGAACTCCACGCGTAGAACCAA
GAGAAGTACGGGCAATACGACCACCCTGTCGCTTGAAAGCGAATCTGTACR
AAATGTGCTCTACGCTCAGCTGCAGTTCACCTATGATACGTTGCGCAGCTAC
ATCAATCGGGCGTTGGCGCAGATCGCCGAGGCCTGGTGTGTGGATCAACGG
CGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAATCCATCAGCCATT
CTCTCGGCCATYTACAACAACAAMMA
>Paciente_2_tumor_gB2
CWSRYTKATTSCKAASGTYTGGCATCGATCCAGTCTGAATATCACTCATAGG
ACCAGAAGAAGTACGAGTGAAAAAATACAACTCATTTGTCCAGCATGGAAT
CGGTGCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCG
CGGTTACATCAACCGGGCGCTGGCGCAAATCGCAGAAKCCTGGTGTGTGGA
TCAACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTC
AGCCATTCTCTCRGCCATYTACAACAAC
>Paciente_3_tumor_gB2
TTKCATGCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAGA
AGAAGTACGAGTGMCMWTAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTYCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCRGCCATYTACAACAACAACA
>Paciente_4_tumor_gB3
GTGACTGGACGTTTGGCATAGCTCCGGTGTGACTCCACGCGTAGAACCAAG
AGAAGTACGGGCAATMYKACCACCCTGTCGCTTGAAAGCGAATCTGTACRA
AATGTGCTCTACGCTCAGCTGCAGTTCACCTATGATACGTTGCGCAGCTACA
55
TCAATCGGGCGTTGGCGCAGATCGCCGAGGCCTGGTGTGTGGATCAACGGC
GCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATC
>Paciente_5_tumor_gB2
TGKGGATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACC
AGAAGAAGTACGAGYGACWWTAATACAACTCATTTGTCCAGCATGGAATC
GGTGCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGC
GCGGTTACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTG
GATCAACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCC
GTCAGCCATTCTCTCGGCCATYTACAACAACAACA
>Paciente_7_tumor_gB2
ATTTTTGGCGATTGCYGATGKACGTTTGGCCATCGATCCGTCTGAATATCCT
CATAGGACCAGAAGAAGTACGAGTGAAAAAATACAACTCATTTGTCCAGCA
TGGAATCGGTGCACAATTTGRTCTACGCCCAGCTGCAGTTCACCTATGACAC
GTTGCGCGGTTACATCAACCGGGCGCTGGCGCAAATCGCAGAMSCCTGGTG
TGTGGATCAACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAA
CCCGTCAGCCATTCTCTCGGCCATYTACAACAACAACA
>Paciente_8_tumor_gB3
GTGGACTGGACGTTTGGCATAGCTCCGGTGTGACTCCACGCGTAGAACCAA
GAGAAGTACGGGCMATWYKACCACCCTGTCGCTTGAAAGCGAATCTGTAC
GAAATGTGCTCTACGCTCAGCTGCAGTTCACCTATGATACGTTGCGCAGCTA
CATCAATCGGGCGTTGGCGCAGATCGCCGAGGCCTGGTGTGTGGATCAACG
GCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAATCCATCAGCCAT
TCTCTCGGCCATYTACAACAACAACM
>Paciente_10_tumor_gB2
ACTGGCTGATTGGACGTTTGGCATCGATCCAGTCTGATATCACTCATAGGAC
CAGAAGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATC
GGTGCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGC
GGTTACATCAACCGGGCGCTGGCGCAAATCGCASAASCCWGGTGTGTGGAT
CAACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCA
GCCATTCTCTCGGCCATCTACAACAACAAAAMAA
56
>Paciente_11_tumor_gB2
TGGGCATTGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCA
GAAGAAGTATGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGG
TGCACAMTCTGGTCWACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCG
GTTACATCAACCGGGCGCTGGCGCAAATCGCAGAMGCCTGGTGTGTGGATC
AACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAG
CCATTCTCTCGGCCATYTACAACAACAACA
>Paciente_12_tumor_gB2
AKGYKGTATTGGACGTTTTGGCATCGATCCAGTCTGATATCACTCATAGGAC
CAGAAGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATC
GGTGCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGC
GGTTACATCAACCGGGCGCTGGCGCAAATCGCAGAMGCCTGGTGTGTGGAT
CAACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCA
GCCATTCTCTCGGCCATYTACAACAAC
>Paciente_13_tumor_gB2
TGTGGATTGGGACGTTTGGCCATCGATCCAGTCTGAATATCACTCATAGGAC
CAGAAGAAGTACGAGTGACAWTWATRCAACTCATTTGTCCAGCATGGAAT
CGGTGCACAAYCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCG
CGGTTACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGA
TCAACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTC
AGCCATTCTCTCRGCCATYTACAACAAC
>Paciente_14_tumor_gB2
TKKGCATGGACGTTTGGCATCGATCCAGTCTGATATCACTCATAGGACCAG
AAGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCGGCCATYTACAACAACAA
57
>Paciente_15_tumor_gB2
TGGCATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCRGCCATYTACAACAACAACA
>Paciente_16_tumor_gB2
TGTCATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAGA
AGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGTG
CACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGTT
ACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAAC
GGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCCA
TTCTCTCGGCCATYTACAACAACA
>Paciente_17_tumor_gB2
TKGCATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCRGCCATYTACAACAACAACA
>Paciente_18_tumor_gB2
TGKTCATGGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCA
GAAGAAGTACGAGTGACAWTAATACAACTCATTTGTCCAGCATGGAATCGG
TGCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGG
TTACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCA
ACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGC
CATTCTCTCRGCCATYTACAACAACA
58
>Paciente_19_tumor_gB2
TTGATCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAGAAG
AAGTACGAGTGMCAATAATACAACTCATTTGTCCAGCATGGAATCGGTGCA
CAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGTTAC
ATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAACGG
CGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCCATT
CTCTCRGCCATYTACAACAACAACA
>Paciente_20_tumor_gB2
TGWKCATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCA
GAAGAAGTACGAGTGMCAWTAATACAACTCATTTGTCCAGCATGGAATCG
GTGCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCG
GTTACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATC
AACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAG
CCATTCTCTCRGCCATYTACAACAACAACACA
>Paciente_21_tumor_gB2
TGTGCATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTACGAGTGMCAWTAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCGGCCATYTACAACAACAACA
>Paciente_22_tumor_gB2
CCCTGCTGCAAACCCCCTTCCCCCCACAWCGCCCGTGTTTGAAAGAGAGTA
CCTATTGGGRGWTAATAGGGGTACGCCTGAYATCGMGWCTTMRACAWTAT
AAGGGGGTGTTCTCTGAACCTTCCCGTTCCCTCCATTGACAAAARMWWTGC
TACCCTGTCCAAGGGGTAAAAATTTTTCCGAGCCAKTGTGGGTGCACCCCCC
CCCT
59
Sangue
>Paciente_2_sangue_gB2
TGTGCATGCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCGGCCATYTACAACAACAACACA
>Paciente_3_sangue_gB2
AKGKGATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCA
GAAGAAGTACGAGTGACWWTWATACAACTCATTTGTCCAGCATGGAATCG
GTGCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCG
GTTACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATC
AACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAG
CCATTCTCTCRGCCATYTACAACAACAACA
>Paciente_5_sangue_gB2
TGTCATGCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAGA
AGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGTG
CACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGTT
ACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAAC
GGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCCA
TTCTCTCGGCCATYTACAACAACCACACA
>Paciente_7_sangue_gB2
TTGCATGGACGTTTGGCCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTACGAGTGMCAWTAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCRGCCATYTACAACAACCACACA
60
>Paciente_8_sangue_gB2
TGTGAATGGACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTACGAGTGACAWTAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCRGCCATYTACAACAACAACACA
>Paciente_10_sangue_gB2
TGTGCATGCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTACGAGTGACAWTAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCRGCCATYTACAACAACCACACA
>Paciente_12_sangue_gB2
TGTGCATGCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAG
AAGAAGTAYGAGTGACAWTAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGT
TACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAA
CGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCC
ATTCTCTCRGCCATYTACAACAACCACA
>Paciente_13_sangue_gB2
TTGATGCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAGAA
GAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGTGC
ACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGTTA
CATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAACG
GCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCCAT
TCTCTCGGCCATYTACAACAACCACACA
61
>Paciente_15_sangue_gB2
TKGACTGCACGTTTGGCCATMGMTCCAGTSTGAAYATCACKCRTAGRACCA
RAAGAAGTACGRGTGAYAMTAMTACAACTCATTTGTCCAGCATGGAATCRG
TGCACAATCTGGTCTACSCCCAGCTGCWSTTCACCTATGACACGTTGCGCGG
TTACATCAACCGGGYGCTGGMGMAAATCGMAGAAKSCTGGKGKGTGGATC
AACGGCSCACCCTAGAGGTCTTCRAGGAACTCARCAAGATCAACCCGTCAR
YYATTCTCTCGGYCATCTACAACAACAACACA
>Paciente_18_sangue_gB2
CMTGATGGGACGTTTGGCATCGATCCAGTCTGATATCACTCATAGGACCAG
AAGAAGTACGAGTGACAATAATACAACTCATTTGTCCAGCATGGAATCGGT
GCACAATCTGGTMTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGG
TTACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCA
ACGGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGC
CATTCTCTCGGCCATYTACAACAACAACA
>Paciente_19_sangue_gB2
TTGCATGCACGTTTGGCATCGATCCAGTCTGAATATCACTCATAGGACCAGA
AGAAGTACGAGTGMCAWTAATACAACTCATTTGTCCAGCATGGAATCGGTG
CACAATCTGGTCTACGCCCAGCTGCAGTTCACCTATGACACGTTGCGCGGTT
ACATCAACCGGGCGCTGGCGCAAATCGCAGAAGCCTGGTGTGTGGATCAAC
GGCGCACCCTAGAGGTCTTCAAGGAACTCAGCAAGATCAACCCGTCAGCCA
TTCTCTCGGCCATYTACAACAACAA
62
Apêndice
Resumos apresentados em Congressos
Resumo apresentado no I Workshop da Pós-Graduação em Biossistemas da
UFABC.
DETECTION OF HUMAN CYTOMEGALOVIRUS (HCMV) IN GLIOBLASTOMA
MULTIFORME (GBM)
Januário,C.S.¹; Figueiredo, E.G.2; Correa, C.2; Cabrera, H.N.3; Schimdt, M.2; Teixeira,
M.J.2 ; Silva, M.C.C. ¹
The Human Cytomegalovirus (HCMV) is an ubiquitous infectious agent, present in
almost 90% of the world's population. In healthy individuals, the infection is normally
asymptomatic, however, in cases of immunosuppression the virus can be a life
threatening agent. Recent findings suggested a relationship between HCMV and cancer.
The virus has been detected in different cancer types, especially in glioblastomas, the
most malignant kind of glial tumors. The studies of the HCMV role in tumor
progression are rapidly advancing and additional work needs to be done to confirm the
viral presence in tumors and identify possible viral proteins involved in malignity. The
aim of this work was to detect the HCMV genome in tumor biopsies obtained from
glioblastoma patients at the Hospital das Clínicas of São Paulo, Brazil. We employed
three different techniques: conventional PCR (cPCR), real time quantitative PCR (qRTPCR) and semi-nested PCR to detect HCMV in peripheral blood and lesions of
glioblastomas patients. The viral genome was only successfully detect by semi-nested
PCR using primers for the variable region of the viral glycoprotein gB. Using a HCMVBAC the detection limit of the techniques was 9 copies/µl in semi-nested PCR, 6800
copies/µl in cPCR and 20 copies/µl in qRT-PCR, indicating that semi-nested PCR is a
more sensitive technique in this case. Twenty three glioblastomas samples were tested,
and 20 (87%) were positive for variable region of the gB glycoprotein. Ten (50%) of the
20 positive tumor patients had also detectable HCMV in their peripheral blood.
Sequencing analysis of the gB demonstrated the presence of different gB genotypes in
tumors and blood of the patients. We are currently performing experiments in order to
verify the viral gene expression in the glioblastomas samples. Our results confirm the
63
presence of HCMV in glioblastomas indicating a possible relationship of the virus with
tumor malignity.
Resumo apresentado no XXIII Brazilian Congresso f Virology & VII Mercosur
Meeting of Virology (XXIII CBV).
DETECTION OF HUMAN CYTOMEGALOVIRUS (HCMV) IN GLIOBLASTOMA
MULTIFORME (GBM)
Januário,C.S.¹; Figueiredo, E.G.2; Correa, C.2; Cabrera, H.N.3; Schimdt, M.2; Teixeira,
M.J.2 ; Silva, M.C.C. ¹
¹Centro de Ciências Naturais e Humanas, Universidade Federal do ABC (UFABC).
2
Divisão de Clínica Neurocirúrgica. Hospital das Clínicas da Faculdade de Medicina da
Universidade de São Paulo.
3
Divisão de Neurocirurgia Funcional – Instituto de Psiquiatria. Hospital das Clínicas da
Faculdade de Medicina da Universidade de São Paulo.
The Human Cytomegalovirus (HCMV) is an ubiquitous infectious agent, present in
almost 90% of the world's population. In healthy individuals, the infection is normally
asymptomatic, however, in cases of immunosuppression the virus can be a life
threatening agent. Recent findings suggested a relationship between HCMV and cancer.
The virus has been detected in different cancer types, specially in glioblastomas, the most
malignant kind of glial tumors. The studies of the HCMV role in tumor progression are
rapidly advancing and additional work needs to be done to confirm the viral presence in
tumors and identify possible viral proteins involved in malignity. The aim of this work
was to detect the HCMV genome in tumor biopsies obtained from glioblastoma patients
at the Hospital das Clínicas of São Paulo, Brazil. We employed three different
techniques: conventional PCR (cPCR), real time quantitative PCR (qRT-PCR) and
semi-nested PCR to detect HCMV in peripheral blood and lesions of glioblastomas
patients. The viral genome was only successfully detect by semi-nested PCR using
primers for the variable region of the viral glycoprotein gB. Using a HCMV-BAC the
detection limit of the techniques was 9 copies/µl in semi-nested PCR, 6800 copies/µl in
cPCR and 20 copies/µl in qRT-PCR, indicating that semi-nested PCR is a more
sensitive technique in this case. At the moment 20 glioblastomas samples were tested
64
and 9(45%) were positive for the gB region. Four (44%) of the 9 positive patients had
also detectable HCMV in their peripheral blood. Sequencing analysis of the gB
demonstrated the presence of different gB genotypes in the tumors and we are analyzing
the gB genotypes in peripheral blood of the patients. We are currently performing
experiments in order to verify the viral gene expression in the glioblastomas samples.
Our results confirm the presence of HCMV in glioblastomas indicating a possible
relationship of the virus with tumor malignity.
Area: Human Virology
Financial support: Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) e
Faculdade de Medicina da Universidade de São Paulo.
65
Resumo apresentado no XXIV Brazilian Congresso f Virology & VIII Mercosur
Meeting of Virology (XXIV CBV).
HIGH PREVALENCE OF HCMV AND VIRAL LOAD IN TUMOR
TISSUES AND PERIPHERAL BLOOD OF GLIOBLASTOMA
MULTIFORME PATIENTS
Januário, C.S ¹; Stangherlin, L.M.¹; Figueiredo, E.G. 2;Corrêa, C.2; Cabrera, H. N.3;
Soares, M.S.2; Teixeira, M.J.2 ; Silva, M.C.C. ¹
¹ Centro de Ciências Naturais e Humanas, Universidade Federal do ABC (UFABC),
Santo André, SP, Brazil;
2
Divisão de Clínica Neurocirúrgica. Hospital das Clínicas da Faculdade de Medicina da
Universidade de São Paulo. São Paulo, SP, Brazil;
3
Divisão de Neurocirurgia Funcional – Instituto de Psiquiatria. Hospital das Clínicas da
Faculdade de Medicina da Universidade de São Paulo. São Paulo, SP, Brazil; E-mail:
[email protected]
Glioblastoma Multiforme (GBM) is the most prevalent and malignant tumor of the
central nervous system. In the last few years, accumulating evidence has suggested an
association between Human Cytomegalovirus (HCMV) infection and GBM. In this
study, we examined tumor tissue and peripheral blood of patients with GBM for the
presence of HCMV DNA. We also determined the viral load and gB genotypes in
HCMV-positive samples. We analyzed twenty-two fresh surgical brain specimens and
twenty peripheral blood samples of GBM patients by real-time PCR (qPCR) and heminested PCR (nPCR) for the presence of pp65 and gB genes, respectively. Viral genome
copy numbers were calculated using qPCR and gB genotype was determined by nPCR.
HCMV DNA was detected in the majority of the tumor samples analyzed (95% by
qPCR and 91% by nPCR). About half of the patients with tumors positive for HCMV
also had detectable viral DNA in their peripheral blood (47% by qPCR and 61% by
nPCR). In the majority of the tumor samples, cellular DNA outnumbers viral DNA
(average of 1 infected cell in 33 cells). gB2 was the most prevalent genotype in the
tumor and blood samples. In this study we found a high prevalence of HCMV in GBM
samples from Brazil. These data reinforce a possible association between HCMV
66
infection and tumor development by supporting similar findings in other regions of the
world.
Financial support: FAPESP
Artigo publicado em revista científica
67
Journal of Medical Virology
High Prevalence of HCMV and Viral Load in Tumor
Tissues and Peripheral Blood of Glioblastoma
Multiforme Patients
Claudia Januário dos Santos,1 Lucas Matheus Stangherlin,1 Eberval Gadelha Figueiredo,2,3
Clemar Corrêa,2,3 Manoel Jacobsen Teixeira,2,3 and Maria Cristina Carlan da Silva1*
1
Centro de Cieˆncias Naturais e Humanas, Universidade Federal do ABC (UFABC), Santo Andre´, SP, Brazil
Divisão de Clı´nica Neurocirúrgica, Hospital das Clı´nicas da Faculdade de Medicina da Universidade de São Paulo,
São Paulo, SP, Brazil
3
Divisão de Neurocirurgia Funcional, Instituto de Psiquiatria. Hospital das Clı´nicas da Faculdade de Medicina da,
Universidade de São Paulo, São Paulo, SP, Brazil
2
Glioblastoma multiforme is the most prevalent
and malignant tumor of the central nervous
system. In the last few years, accumulating
evidence has suggested an association between human cytomegalovirus (HCMV) infection and glioblastoma multiforme. In this
study, tumor tissues and peripheral blood of
patients with glioblastoma multiforme were
examined for the presence of HCMV DNA.
Twenty-two fresh surgical brain specimens and
20 peripheral blood samples were analyzed by
real-time PCR (qPCR) and hemi-nested PCR
(nPCR) for the presence of pp65 and (glycoprotein B) gB viral genomic regions, respectively.
HCMV DNA was detected in the majority of the
tumor samples analyzed (95% by qPCR and
91% by nPCR). About half of the patients with
tumors positive for HCMV also had detectable
viral DNA in their peripheral blood (47% by
qPCR and 61% by nPCR). Genome copy numbers were determined and in the majority of
the tumor samples cellular DNA outnumbers
viral DNA (average of 1 infected cell in 33
cells). The gB genotypes were determined
in HCMV-positive samples and gB2 was the
most prevalent genotype in the tumor and
blood samples. The results show a high prevalence of HCMV in glioblastoma multiforme
samples reinforcing a possible association
between HCMV infection and tumor development. J. Med. Virol.
# 2013 Wiley Periodicals, Inc.
KEY WORDS:
human cytomegalovirus; glioblastoma multiforme; detection
INTRODUCTION
The International Agency for Research on Cancer
estimates that 20% of the all cancer cases worldwide
are caused by infections, with most of them caused
by viruses, including: Epstein–Barr virus (EBV)
(Herpesviridae family, Lymphocryptovirus genus),
hepatitis B virus (HBV) (Hepadnaviridae family,
Orthohepadnavirus genus), human T-lymphotropic
virus-I (HTLV-I) (Retroviridae family, Deltaretrovirus
genus), human papillomavirus (HPV) (Papillomaviridae family, Alphapapillomavirus genus), hepatitis C
virus (HCV) (Flaviviridae family, Hepacivirus genus),
Kaposi’s sarcoma-associated herpesvirus (KSHV)
(Herpesviridae family, Rhadinovirus genus), and
Merkel cell polyomavirus (MCV) (Polyomaviridae
family, Polyomavirus genus) [Moore and Chang,
2010]. The presence of virus, with or without gene
expression, can lead to: a disruption of cell cycle,
evasion of growth suppressors, induction of angiogenesis, deregulation of cellular energetics, prevention of
apoptosis and cell immortality. All of these abnormalities are also hallmarks of cancer [Hanahan and
Weinberg, 2011]. Also, even viruses not considered as
tumor initiators can alter molecular events in the cell
and potentially contribute to tumor progression or
malignancy. One of these viruses is the human
cytomegalovirus (HCMV) (Herpesviridae family, Cytomegalovirus genus).
Grant sponsor: Fundação de Amparo a Pesquisa do Estado de
São Paulo, Brazil (FAPESP); Grant number: 2010/14830-7.
*Correspondence to: Maria Cristina Carlan da Silva, Centro de
Ciências Naturais e Humanas, Universidade Federal do ABC
(UFABC), Santo André, CEP 09210-580, SP, Brazil.
E-mail: [email protected]
Accepted 24 September 2013
DOI 10.1002/jmv.23820
Published online in Wiley Online Library
(wileyonlinelibrary.com).
C 2013 WILEY PERIODICALS, INC.
2
The b-herpesvirus HCMV is present in the majority of the population worldwide. HCMV infection is
generally asymptomatic in healthy individuals. However in immunocompromised individuals—such as
transplant recipients, AIDS, and cancer patients—the
virus can be a life-threatening agent. HCMV is also
the most common congenital infection and is associated with birth defects, mental retardation, and hearing loss [Sissons and Carmichael, 2002; Mockarsi
et al., 2006].
Of potential relevance to cancer, the HCMV genome and gene expression have been detected in
many types of tumors including colorectal carcinoma
[Harkins et al., 2002], prostate cancer [Samanta
et al., 2003], skin cancer [Zafiropoulos et al., 2003],
rhabdomyosarcomas [Price et al., 2012], breast cancer
[El-Shinawi et al., 2013], mucoepidermoid carcinoma
of salivary glands [Melnick et al., 2013], neuroblastoma [Wolmer-Solberg et al., 2013] and glioblastoma
multiforme [reviewed in Dziurzynski et al., 2012].
Several HCMV genes encode products that have the
potential to facilitate tumor growth. The viral IE1
and IE2 can inhibit apoptosis and increase cell
proliferation [Speir et al., 1994; Zhu et al., 1995;
Cobbs et al., 2008], IE1 can also induce telomerase
activity and disrupt gap junctions [Straat et al., 2009;
Khan et al., 2013], pUL82 and UL97 can inhibit the
RB protein [Kalejta et al., 2003; Hume et al., 2008],
the gB protein can activate the PDGFR-a receptor
tyrosine kinase [Soroceanu et al., 2008], pUL82 and
pUS28 can upregulate vascular endothelial growth
factor and stem cell factor, stimulating angiogenesis
[Maussang et al., 2006; Matlaf et al., 2013], pUL76
induces chromosomal aberrations [Siew et al., 2009]
and US2, US3, US6, and US11 antagonize MHC I
and MHC II expression on the cell surface [Ahn
et al., 1996; Jones et al., 1996; Wiertz et al., 1996;
Machold et al., 1997].
Glioblastoma multiforme is the most common and
malignant primary tumor of glial cells, being classified as a high-grade glioma (grade IV) [Holland,
2000]. Its etiology is unknown, however some studies
show that exposure to ionizing radiation, or electric
or magnetic fields can be risk factors [Ohgaki, 2009].
The overall median survival after diagnosis is
15 months, despite of the combined therapy of tumor
resection, radiation, and temozolomide [Affronti
et al., 2009].
Several studies have demonstrated the relationship
between HCMV and glioblastoma multiforme. In a
pioneering study, Cobbs et al. [2002] detected the
viral protein IE1 in 100% of glioblastoma multiforme
samples by immunohistochemistry (IHC), with expression restricted to the tumor cells. Subsequent
studies failed to detected HCMV in tumor samples
[Lau et al., 2005; Poltermann et al., 2006] or detected
it at low levels [Sabatier et al., 2005], leading to a
controversy in the literature regarding the presence
or not of the virus in this kind of tumor. Further
studies by Scheurer et al. [2008] and Mitchell et al.
J. Med. Virol. DOI 10.1002/jmv
dos Santos et al.
[2008] argued that the discrepancy of the results
were due to differences in the sensitivity of the
techniques used by different groups. Employing high
sensitive assays, Scheurer et al. [2008] detected the
IE1 protein in 100% of glioblastoma multiforme and
82% of low-grade glioblastoma using IHC, validating
the results initially published by Cobbs et al. [2002].
More recent studies have also confirmed the presence of the HCMV genome and viral proteins in a
high percentage of glioblastoma multiforme. Mitchell
et al. [2008] (93% by IHC assay of IE1); Slinger et al.
[2010] (100% by IHC assay of IE and US28 antigens);
Lucas et al. [2011] (51% by IHC assay of pUL83);
Soroceanu et al. [2011] (65% by IHC assay of pUS28);
Ranganathan et al. [2012] (70% by PCR assay of
multiple HCMV genome regions); Fonseca et al.
[2012] (36% by PCR assay of pUL83) Rahbar et al.
[2012] (99% by IHC against IE antigen) and Rahbar
et al. [2013] (99% by IHC assay of IE antigen).
Nowadays the consensus is that HCMV is present in
most, if not all glioblastoma multiforme tumors, and
that it likely modulates the malignant phenotype of
the tumor, being therefore considered an oncomodulatory agent [Dziurzynski et al., 2012].
Clinical studies show that glioblastoma multiforme
patients with lower HCMV viral load have better
survival rates than the ones with high viral load
[Soderberg-Naucler, 2008; Rahbar et al., 2012, 2013]
and a recent study demonstrated that patients with
glioblastoma multiforme who received valganciclovir
for anti-CMV therapy had a higher survival rate
than
untreated
patients
[Soderberg-Naucler
et al., 2013].
In this study the presence of HCMV viral genome
was analyzed in tumor tissues and peripheral blood
of patients with glioblastoma multiforme. In addition
the viral DNA was quantified and the gB genotypes
were determined in the samples. The results show
that the majority of tumor samples analyzed was
positive for the pp65 and gB genomic regions of
HCMV. Half of the patients with HCMV-positive
tumors also had detectable viral DNA in their
peripheral blood. In the majority of tumors analyzed,
the cellular DNA outnumbers viral DNA, supporting
the findings that not all cells in the tumor harbor
HCMV DNA. The gB2 genotype was the most prevalent in the tumor and blood samples.
MATERIALS AND METHODS
Clinical Samples
Twenty two fresh brain surgical specimens and
twenty samples from peripheral blood of the glioblastoma multiforme patients were obtained from the
Centro de Neurologia do Hospital das Clı́nicas de São
Paulo, in a collaboration study, with approval of the
local ethics committee (approval no 0654/10). All the
patients were informed of the procedure and signed a
consent form. The tumor samples were histopathologically confirmed as GMBs. The blood samples were
HCMV Detection in Glioblastoma Multiforme
collected in heparin tubes and the tissues in RNAlater solution (Ambion, Austin, TX) and kept at 4˚C
until processing.
DNA Extraction
Total DNA was extracted from 20 mg of tumor
tissue or 200 ml of peripheral blood, using the Pure
Link genomic DNA mini kit (Invitrogen, Carlsbad,
CA) and the ReadyAmp Genomic DNA purification
system (Promega, Madison, WI), respectively, according manufacturer’s instructions.
Determination of Limits of Detection
and Viral Load in the Samples
To determine the lower limit of detection of the
viral DNA, the PCR was performed using 10-fold
serially dilutions of HCMV FIX-BAC (HCMV FIX
genome cloned as a Bacterial Artificial Chromosomes), of known concentration. PCR was performed
directly to the reaction and in total DNA (extracted
from a HCMV negative blood, containing the
added viral dilutions). The copy number was calculated as described by Cunha et al. [2002], considering
the molecular weight of the viral genome to be
240 kb.
The amount of viral DNA in the samples was
determined by amplification of the pp65 viral gene in
real-time PCR standard curve (R2 ¼ 0.951), generated
from the 10-fold serial dilutions of known HCMV
FIX-BAC concentration, as already described. The
cellular DNA quantity for each sample was also
calculated by standard curve (R2 ¼ 0.9787), using the
GAPDH gene, obtained by amplification of 10-fold
different amounts of total DNA. A conversion factor
of 6 pg of DNA per diploid cell was used for estimating the number of total cells in each sample (considering the molecular weight of a DNA base pair 618 g/
mol and the molecular weight of DNA 1.85 1012 g/
mol in 3 billion base pairs). The HCMV viral load
in tumor tissue and blood was then calculated as the
log of the ratio of the cell number to HCMV DNA
(log10 cell number/pp65 copies).
The viral load in blood samples from glioblastoma
multiforme and renal transplant recipients were
determined using the pp65 real-time PCR standard
curve, describe above, and expressed as log10
copies/ml.
Qualitative PCR
Conventional PCR (cPCR) amplifications were performed in a 50 ml mixture containing 2 ml of DNA,
2 mM MgCl2, 200 mM dNTPs, 0.75 mM of each primer, and 5U Taq Polimerase (Ludwig Biotec, Alvorada,
Brazil). The PCR conditions were: 94˚C for 3 min,
followed by 40 cycles of 94˚C for 30 sec; 55.6˚C for
30 sec; 72˚C for 45 sec. For amplification of the viral
DNA the following primers were used: UL44 (50 -TAC
AAC AGC GTG TCG TGC TCC G-30 and 50 -GGC
3
GTG AAA AAC ATG CGT ATC AAC-30 ), UL123 (50 GCC TTC CCT AAG ACC ACC AAT-30 and 50 -ATT
TTC TGG GCA TAA GCC ATA ATC-30 ), UL99 (50 GTG TCC CAT TCC CGA CTC G-30 and 50 -TTC ACA
ACG TCC ACC CAC C-30 ) [Mitchell et al., 2009]. As a
positive control for cellular DNA, primers for the
glyceraldehyde 3-phosphate dehydrogenase gene
(GAPDH) gene were used (50 -ACC CAC TCC TCC
ACC TTT GAC-30 and 50 -CTG TTG CTG TAG CCA
AAT TCG T-30 ).
Quantitative Real-Time PCR
HCMV viral DNA was amplified by real-time PCR
(qPCR), using the primers described previously
(UL44, UL123, UL99, and GAPDH), plus a primer for
UL83 region (50 -CCC AGG TGT GTC GGT ACT CA-30
and 50 -CCA CCT TCA CCA GCC AGT ATC-30 )
designed using PrimerExpress software (Applied Biosystems, Warrington, UK). The reactions were carried out in a StepOne Plus real-time PCR system
(Applied Biosystems) in final volume of 10 ml containing 1 ml of DNA; SYBER Green 1 (Applied
Biosystems) and 0.62 mm of each primer. The PCR
conditions: 95˚C for 10 min, 40 cycles of 95˚C for
15 sec, 60˚C for 1 min and 72˚C for 30 sec. Data were
collected and analyzed by using Step One Software v.
2.2 (Applied Biosystems).
Hemi-Nested PCR and Characterization
of gB Genotypes
The hemi-nested PCR (nPCR) were performed
using primers for the variable region of the UL55
gene (gB) described previously by Zheng et al. [2002].
The reactions contained 2 ml DNA, Taq Polymerase
buffer 1, 2 mM MgCl2, 2.5U Taq Polymerase (Ludwig Biotec), 200 mM dNTPs and 0.15 mM of each
primer, in a final volume of 50 ml. The first round of
amplification was performed using primers: 50 -TGT
TCT GGC AAG GYA TCA AG-30 and 50 -TCA CAA
GAC ATC ACC CAT GAA AC-30 and the second
round primers: 50 -TGT TCT GGC AAG GYA TCA
AG-30 and 50 -GTT GTT GTA RAT GGC YGA GAG-30 .
The PCR conditions were 94˚C for 14 min, 35 cycles
at 95˚C for 30 sec; 56.2˚C for 30 sec; 72˚C for 45 sec;
72˚C for 10 min. All the reactions were repeated at
least three times for confirmation and to avoid of
false positive and negative results. Positive controls
were only used during the primer optimization, no
positive controls were used during the HCMV detection in nPCR to minimize the possibility of laboratory
contamination with HCMV DNA.
Amplified products were visualized on agarose gels
with gel red (Uniscience, Peosta, IA), bands were cut
out and DNA extracted was analyzed by sequencing
(Serviço de Sequenciamento de DNA-SSDNA IQUSP).
Confirmation of the HCMV sequences, and the determination of the gB genotypes were performed using
the National Center for Biotechnology Information
(NCBI-USA) Blast tool.
J. Med. Virol. DOI 10.1002/jmv
4
dos Santos et al.
RESULTS
HCMV Detection in Tumor Tissues
In order to evaluate the best method for detection
of the viral DNA in glioblastoma multiforme samples
different PCR techniques were employed: conventional PCR (cPCR), real-time quantitative PCR (qPCR)
and hemi-nested (nPCR) using primers for different
regions of the viral genome (UL44, UL99, UL123,
UL83, and UL55).
Using as a template DNA extracted from HCMV
negative blood in which 10-fold dilutions of a known
concentration of the HCMV-BAC genome was added,
the lower limits of detection were calculated. The
greatest sensitivities were found with primers for
the UL83 region (pp65) by qPCR (2 copies/ml) and for
the variable region of UL55 (gB) by nPCR (9 copies/
ml) (Supplementary Fig. 1). HCMV viral DNA was
not detectable by cPCR with any primer tested.
Therefore qPCR and nPCR were used to screen
glioblastoma multiforme and peripheral blood samples from patients at Centro de Neurologia do Hospital das Clı́nicas de São Paulo-Brazil, for the HCMV
viral DNA presence.
The viral gB region was detected in 20 out of 22
(91%) tumor and 11 out 20 (55%) blood samples
by nPCR (Fig. 1). Using qPCR, 21 out of 22 (95%)
tumors and 9 out of 20 (45%) blood samples were
positive.
In cases in which it was possible to obtain blood
and tumor samples from the same patient, a correlation was made between the presence of the virus in
Fig. 1. nPCR analysis of tumor and blood samples. DNA extracted from tumor (a) and blood
(b) samples were amplified using primers for the gB variable region of HCMV. Amplification
yielded a band of 316 bp. The GAPDH gene (203 bp) was amplified as a control for cellular DNA.
H2O was used as negative control. P01 to P22 are referred to glioblastoma multiforme samples
and OT (OT1 to OT5) to other types of brain tumors, such as astrocytoma and gliosarcoma, not
included in this study.
J. Med. Virol. DOI 10.1002/jmv
HCMV Detection in Glioblastoma Multiforme
5
both samples. A total of 19 samples were analyzed for
pp65 and 9 (47%) showed positivity in both tumor
and blood samples. The gB presence was analyzed in
samples from 18 patients and 11 (61%) were positive
in their blood and tumor samples. These results are
summarized in Table I.
Correlation Between gB Genotypes in Tumors
and Peripheral Blood Corresponding Samples
The HCMV genome contains genetic differences
among strains. The UL55 gene encodes the gB, one of
the major components of the viral envelope, which is
cleaved during transport through the exocytic pathway. gB is highly variable at the protease cleavage
site and according its sequence variation viral strains
are classified into genotypes gB1 to gB4 [Chou and
Dennison, 1991], gB5 [Shepp et al., 1996], and gB6
and gB7 [Trincado et al., 2000].
To investigate the similarity of viral strains present in peripheral blood and tumors from the same
patient, amplified PCR products were sequenced and
the gB genotypes were determined. Sequences were
analyzed for comparison to reference sequences using
a National Biotechnology Information BLAST.
Sequence analysis showed that of the 20 HCMVpositive tumors by nPCR, 16 belong to the gB2
genotype and 3 to the gB3 genotype. All of the 11
positive blood samples belong to the gB2 genotype.
The gB genotype found in the blood sample always
matched the genotype of the tumor sample from the
same patient. HCMV genotypes gB1, gB4, gB5, gB6,
and gB7 were not found (Table II).
Viral Load in Tumor and Blood Samples
In order to estimate the amount of viral DNA in
the samples analyzed, a correlation between viral
TABLE I. Frequency of HCMV Detection and Correlation of
Positivity in Tumor and Peripheral Blood Samples
Blood tumor
Tumor (þ) overall
Blood (þ) overall
Tumor (þ)/blood (þ)
pp65 (qPCR)
gB (nPCR)
21 of 22 (95%)
9 of 20 (45%)
9 of 19 (47%)
20 of 22 (91%)
11 of 20 (55%)
11 of 18 (61%)
TABLE II. Frequency of gB Genotypes in the Tumor and
Blood Samples
Genotype
gB
gB
gB
gB
gB
gB
gB
1
2
3
4
5
6
7
Tumor
0/20
17/20
3/20
0/20
0/20
0/20
0/20
(0%)
(85%)
(15%)
(0%)
(0%)
(0%)
(0%)
Blood
0/11
11/11
0/11
0/11
0/11
0/11
0/11
(0%)
(100%)
(0%)
(0%)
(0%)
(0%)
(0%)
DNA and cellular DNA was made. As demonstrated
in Figure 2a, for the majority of tumors analyzed,
cellular DNA outnumbers viral DNA. The viral copy
numbers varied from extremely high (3.16 104 pp65/
cells) in one patient (P6) to very low (average
4.77 103 pp65/cells) in few patients (P5, P13, P15,
P17, P21). On average, 1 in 33 cells harbor viral
DNA. This result corresponds to HCMV infection of
cells at a low MOI as described previously [Ranganathan et al., 2012].
The viral load in glioblastoma multiforme positive
blood samples was also determined. For comparison,
eight samples from renal transplant recipients were
included in the analysis. As shown in Figure 2b there
is no significant difference in viral load in the two
types of samples. The average copy number in
glioblastoma multiforme and renal transplant recipients is 1.3 105 and 3.2 105 copies/ml, respectively.
DISCUSSION
The presence of HCMV in glioblastoma multiforme
has been debated for several years. Since the first
report by Cobbs et al. [2002], many studies looked for
the presence of the HCMV genome and expression of
HCMV proteins in this type of tumors. While some
authors detected the virus, others did not. After the
demonstration that the absence of detection was
due to a lack in sensitivity of the techniques used,
a consensus was reached, and to date HCMV is
believed to be present in most, if not all glioblastoma
multiforme tumors [Dziurzynski et al., 2012].
Yet, additional work showing the presence of the
virus in a variety of samples from diverse regions of
the world, is important, particularly to determine if
HCMV is present or not in glioblastoma multiforme
and in what frequencies in different populations,
which could be due to genetic variation.
The data presented in this study confirm the
presence of the HCMV genome in the majority of
the glioblastoma multiforme samples analyzed from a
population of patients from Brazil. By comparing
three different PCR techniques our analysis show
that qPCR, followed by nPCR are more sensitive for
detection of HCMV genomic regions. Using these
techniques the UL83 and UL55 regions were detected
at 96% (qPCR) and 83% (nPCR) of the tumor
samples, respectively.
Most of the studies that evaluated the presence of
HCMV in glioblastoma multiforme samples used IHC
or in situ hybridization (ISH). Although these assays
were proven to be sensitive and suitable to demonstrate the location of viral proteins or DNA in single
cells they are laborious and costly. Detection of viral
genomic regions by PCR is less expensive and more
convenient for screening purposes.
Fewer studies have looked for the presence of viral
DNA in glioblastoma multiforme by PCR. Cobbs et al.
[2002] by nested PCR detected gB in 77.7% of
paraffin embedded samples. However, using the same
J. Med. Virol. DOI 10.1002/jmv
6
dos Santos et al.
Fig. 2. Quantitation of viral DNA by qPCR in tumor and blood samples. Twenty-two tumor
samples (a) were analyzed by quantitative PCR for the pp65 viral region and the cellular gene
GAPDH. The relationship between the cellular DNA and viral DNA is expressed as a log10.
Nine and eight blood samples from glioblastoma multiforme and renal transplant recipients,
respectively (b), were analyzed by quantitative PCR for the pp65 viral region. The viral loads
are expressed as viral copy numbers/ml.
technique, Poltermann et al. [2006] and Lau et al.
[2005] fail to detect gB in 22 and 8 paraffin samples,
respectively. Mitchell et al. [2008] by real-time PCR
detected gB in paraffin samples and primary glioblastoma multiforme cultured cells in 61.7% and 70%,
respectively [Mitchell et al., 2008]. In contrast, Lau
et al. [2005] by cPCR were not able to detect gB in
eight paraffin samples.
Ranganathan et al. [2012] was the only group to
report the detection of the viral genome by cPCR in
glioblastoma multiforme samples. In this work, multiple HCMV genomic loci were found to be present in
DNA extracted from paraffin or frozen samples at
frequencies of 55% and 70%, respectively [Ranganathan et al., 2012]. Viral DNA was not detected by
cPCR, in the present work, using three different sets
of primers (UL44, UL123, and UL99). This fact could
J. Med. Virol. DOI 10.1002/jmv
be attributed to difference in the sensitivity of the
primers used in the earlier report as compared to
this study, variations at primer binding sites or to
sequence variability in HCMV genomes, as reported
by Renzette et al. [2011].
Using nPCR a higher frequency of gB positivity
(83%) was found in glioblastoma multiforme samples
than reported previously Cobbs et al. [2002]. However, while the earlier study used DNA extracted from
paraffin samples the present work used DNA extracted from fresh tumor tissues and this fact likely
accounts for the difference.
The data show that HCMV is present at high
frequency in glioblastoma multiforme and the choice
of the PCR technique and tumor samples to be used
is important for the successful detection of the virus
at low levels.
HCMV Detection in Glioblastoma Multiforme
Quantitation of viral DNA demonstrated that in
the majority of tumors the amount of cellular DNA is
higher than viral DNA (Fig. 2a). This can be due to
the fact that not all cells in the tumor harbor HCMV
DNA as suggested by Ranganathan et al. [2012].
In a great majority of the patients the gB2
genotype was found to be present both in tumors and
blood. It is possible that there is an association of
gB2 with glioblastoma multiforme. However, previous
studies found a higher frequency of this genotype in
immunosuppressed patients from Brazil [Carraro and
Granato, 2003; Yamamoto et al., 2007; Correia-Silva
et al., 2011]. Therefore more likely our findings
reflect a predominance of gB 2 in Brazil.
Many questions remain. For instance, it is not
known if HCMV infection of tumor cells results from
viral reactivation in situ or from reactivated virus
from periphery that is brought to the tumor sites by
infiltrating immune cells. Few studies have looked
for the presence of HCMV both in tumor samples and
peripheral blood. While Poltermann et al. [2006] and
Lehrer et al. [2011] failed to detect the virus, Mitchell
et al. [2008] found that 50% of the glioblastoma
multiforme patients with HCMV in their tumors also
had the virus in their blood. The current study shows
a very similar frequency of positivity in blood samples of patients with positive tumors, whether assaying UL83 (47%) or gB (61%) (Table I).
HCMV reactivation in glioblastoma multiforme
patients can be a consequence of cancer related
immunosuppression or a consequence of treatment
related immunosuppression. Mitchell et al. [2008]
proposed that reactivation was likely due to cancer
immunosuppression, since the patients in their study
had undergone less than 2 weeks of corticosteroid
therapy prior to resection. Earlier studies in transplant recipients demonstrated that it takes several
weeks to reactivate after immunosuppressive treatment [Preiser et al., 2001; Zekri et al., 2004]. The
patients in the present study received corticosteroid
therapy for an average of 1–4 weeks before tumor
resection reinforcing the idea that reactivation was
caused by cancer related immunosuppression instead
of treatment-related immunosuppression. Glioblastoma multiforme patients exhibit a profound immunosuppression related to cancer [Gomez et al., 2008],
and the impaired cell-mediated immunity observed in
the patients is likely to be critical for HCMV
reactivation [Dix et al., 1999].
About half of the patients HCMV glioblastoma
multiforme positive also positive in the blood as
shown in the present study and by Mitchell et al.
[2008]. With these results it is not clear if immunosuppression leads to viral reactivation in the blood or
in the tumor cells or both and further studies need to
be performed to address this question.
However, since half of the patients with positive
tumors do not have detectable virus in their blood it
is possible that the virus reactivates locally in tumor
cells. HCMV is tropic for glial cells [Fritschy
7
et al., 1996], and it has been shown that infection of
malignant glial cells leads to virus persistence and
production of virus with mutations that could be
related with absence of cytophatic effect [Ogura
et al., 1986]. In addition, in latently infected glioma
cells stimuli, such as inflammation causes viral
reactivation [Poland et al., 1990].
Whether reactivation occurs locally in the tumor or
systemically, patients with glioblastoma multiforme
with HCMV in their blood have similar viral loads as
renal transplant recipients, indicating that the virus is
active in their blood and replicates at the same level.
In summary, the current study demonstrated a
high prevalence of HCMV in glioblastoma multiforme
tumors samples taken from patients in Brazil. The
data reinforce a possible association between HCMV
infection and tumor development similar to findings
in other regions of the world.
ACKNOWLEDGMENTS
We thank Thomas Shenk (Princeton University,
USA) for the HCMV FIX-BAC and Hector Navarro
Cabrera and Matheus Schmidt Soares for help with
in brain surgery.
REFERENCES
Affronti ML, Heery CR, Herndon JE II, Rich JN, Reardon DA,
Desjardins A, Vredenburgh JJ, Friedman AH, Bigner DD, Friedman HS. 2009. Overall survival of newly diagnosed glioblastoma
patients receiving carmustine wafers followed by radiation and
concurrent temozolomide plus rotational multiagent chemotherapy. Cancer 115:3501–3511.
Ahn K, Angulo A, Ghazal P, Peterson PA, Yang Y, Fruh K. 1996.
Human cytomegalovirus inhibits antigen presentation by a
sequential multistep process. Proc Natl Acad Sci 93:10990–
10995.
Carraro E, Granato CF. 2003. Single human cytomegalovirus gB
genotype shed in multiple sites at the time of diagnosis in renal
transplant recipients. J Med Virol 70:240–243.
Chou SW, Dennison KM. 1991. Analysis of interstrain variation in
cytomegalovirus glycoprotein B sequences encoding neutralization-related epitopes. J Infect Dis 163:1229–1234.
Cobbs CS, Harkins L, Samanta M, Gillespie GY, Bharara S, King
PH, Nabors LB, Cobbs CG, Britt WJ. 2002. Human cytomegalovirus infection and expression in human malignant glioma.
Cancer Res 62:3347–3350.
Cobbs CS, Soroceanu L, Denham S, Zhang W, Kraus MH. 2008.
Modulation of oncogenic phenotype in human glioma cells by
cytomegalovirus IE1-mediated mitogenicity. Cancer Res 68:724–
730.
Correia-Silva JF, Resende RG, Arao TC, Abreu MH, Teixeira MM,
Bittencourt H, Silva TA, Gomez RS. 2011. HCMV gB genotype
and its association with cytokine levels in hematopoietic stem
cell transplantation. Oral Dis 17:530–537.
Cunha AA, Marin LJ, Aquino VH, Figueiredo LT. 2002. Diagnosis
of cytomegalovirus infections by qualitative and quantitative
PCR in HIV infected patients. Rev Inst Med Trop 44:127–132.
Dix AR, Brooks WH, Roszman TL, Morford LA. 1999. Immune
defects observed in patients with primary malignant brain
tumors. J Neuroimmunol 100:216–232.
Dziurzynski K, Chang SM, Heimberger AB, Kalejta RF, McGregor
Dallas SR, Smit M, Soroceanu L, Cobbs CS; HCMV and Gliomas
Symposium. 2012. Consensus on the role of human cytomegalovirus in glioblastoma. Neuro-Oncology 14:246–255.
El-Shinawi M, Mohamed HT, El-Ghonaimy EA, Tantawy M, Younis
A, Schneider RJ, Mohamed MM. 2013. Human cytomegalovirusinfection enhances NF-kappaB/p65 signaling in inflammatory
breast cancer patients. PLoS ONE 8:e55755.
J. Med. Virol. DOI 10.1002/jmv
8
Fonseca RF, Kawamura MT, Oliveira JA, Teixeira A, Alves G,
Carvalho Mda G. 2012. The prevalence of human cytomegalovirusDNA in gliomas of Brazilian patients. Mem Inst Oswaldo
Cruz 107:953–954.
Fritschy JM, Brandner S, Aguzzi A, Koedood M, Luscher B,
Mitchell PJ. 1996. Brain cell type specificity and gliosis-induced
activation of the human cytomegalovirusimmediate-early promoter in transgenic mice. J Neurosci 16:2275–2282.
Gomez GG, Hickey MJ, Tritz R, Kruse CA. 2008. Immunoresistant
human glioma cell clones selected with alloreactive cytotoxic T
lymphocytes: Downregulation of multiple proapoptotic factors.
Gene Ther Mol Biol 12:101–110.
Hanahan D, Weinberg RA. 2011. Hallmarks of cancer: The next
generation. Cell 144:646–674.
Harkins L, Volk AL, Samanta M, Mikolaenko I, Britt WJ, Bland
KI, Cobbs CS. 2002. Specific localisation of human cytomegalovirusnucleic acids and proteins in human colorectal cancer.
Lancet 360:1557–1563.
Holland EC. 2000. Glioblastoma multiforme: The terminator. Proc
Natl Acad Sci 97:6242–6244.
Hume AJ, Finkel JS, Kamil JP, Coen DM, Culbertson MR, Kalejta
RF. 2008. Phosphorylation of retinoblastoma protein by viral
protein with cyclin-dependent kinase function. Science 320:797–
799.
Jones TR, Wiertz EJ, Sun L, Fish KN, Nelson JA, Ploegh HL. 1996.
Human cytomegalovirusUS3 impairs transport and maturation
of major histocompatibility complex class I heavy chains. Proc
Natl Acad Sci 93:11327–11333.
Kalejta RF, Bechtel JT, Shenk T. 2003. Human cytomegaloviruspp71 stimulates cell cycle progression by inducing the proteasome-dependent degradation of the retinoblastoma family of
tumor suppressors. Mol Cell Biol 23:1885–1895.
Khan Z, Yaiw KC, Wilhelmi V, Lam H, Rahbar A, Stragliotto G,
Soderberg-Naucler C. 2013. Human cytomegalovirus immediateearly proteins promote degradation of connexin 43 and disrupt
gap junction communication: Implications for a role in gliomagenesis. Carcinogenesis doi: 10.1093/carcin/bgt292
Lau SK, Chen YY, Chen WG, Diamond DJ, Mamelak AN, Zaia JA,
Weiss LM. 2005. Lack of association of cytomegalovirus with
human brain tumors. Mod Pathol 18:838–843.
Lehrer S, Labombardi V, Green S, Pessin-Minsley MS, Germano
IM, Rosenzweig KE. 2011. No circulating cytomegalovirus in five
patients with glioblastoma multiforme. Anticancer Res 31:959–
960.
Lucas KG, Bao L, Bruggeman R, Dunham K, Specht C. 2011. The
detection of CMV pp65 and IE1 in glioblastoma multiforme. J
Neuro-Oncol 103:231–238.
Machold RP, Wiertz EJ, Jones TR, Ploegh HL. 1997. The HCMV
gene products US11 and US2 differ in their ability to attack
allelic forms of murine major histocompatibility complex (MHC)
class I heavy chains. J Exp Med 185:363–366.
Matlaf LA, Harkins LE, Bezrookove V, Cobbs CS, Soroceanu L.
2013. Cytomegalovirus pp71 protein is expressed in human
glioblastoma and promotes pro-angiogenic signaling by activation of stem cell factor. PLoS ONE 8:e68176.
Maussang D, Verzijl D, van Walsum M, Leurs R, Holl J, Pleskoff O,
Michel D, van Dongen GA, Smit MJ. 2006. Human cytomegalovirus-encoded chemokine receptor US28 promotes tumorigenesis. Proc Natl Acad Sci 103:13068–13073.
Melnick M, Deluca KA, Sedghizadeh PP, Jaskoll T. 2013. Cytomegalovirus-induced salivary gland pathology: AREG, FGF8, TNFalpha, and IL-6 signal dysregulation and neoplasia. Exp Mol
Pathol 94:386–397.
Mitchell DA, Xie W, Schmittling R, Learn C, Friedman A, McLendon RE, Sampson JH. 2008. Sensitive detection of human
cytomegalovirusin tumors and peripheral blood of patients
diagnosed with glioblastoma. Neuro-oncology 10:10–18.
Mitchell DP, Savaryn JP, Moorman NJ, Shenk T, Terhune SS.
2009. Human cytomegalovirusUL28 and UL29 open reading
frames encode a spliced mRNA and stimulate accumulation of
immediate-early RNAs. J Virol 83:10187–10197.
Mockarsi EJ, Shenk T, Pass RP. 2006. Cytomegalovirus. In: Knipe
DM, Howley PM, editors. Fields virology, 5th edition. Philadelphia, PA: Lippincott- Raven.
Moore PS, Chang Y. 2010. Why do viruses cause cancer? Highlights
of the first century of human tumour virology. Nat Rev Cancer
10:878–889.
J. Med. Virol. DOI 10.1002/jmv
dos Santos et al.
Ogura T, Tanaka J, Kamiya S, Sato H, Ogura H, Hatano M. 1986.
Human cytomegaloviruspersistent infection in a human central
nervous system cell line: Production of a variant virus with
different growth characteristics. J Gen Virol 67:2605–2616.
Ohgaki H. 2009. Epidemiology of brain tumors. Methods Mol Biol
472:323–342.
Poland SD, Costello P, Dekaban GA, Rice GP. 1990. Cytomegalovirus in the brain: In vitro infection of human brain-derived cells.
J Infect Dis 162:1252–1262.
Poltermann S, Schlehofer B, Steindorf K, Schnitzler P, Geletneky
K, Schlehofer JR. 2006. Lack of association of herpesviruses
with brain tumors. J Neurovirol 12:90–99.
Preiser W, Brauninger S, Schwerdtfeger R, Ayliffe U, Garson JA,
Brink NS, Franck S, Doerr HW, Rabenau HF. 2001. Evaluation
of diagnostic methods for the detection of cytomegalovirus in
recipients of allogeneic stem cell transplants. J Clin Virol 20:59–
70.
Price RL, Bingmer K, Harkins L, Iwenofu OH, Kwon CH, Cook C,
Pelloski C, Chiocca EA. 2012. Cytomegalovirus infection leads to
pleomorphic rhabdomyosarcomas in Trp53þ/ mice. Cancer Res
72:5669–5674.
Rahbar A, Orrego A, Peredo I, Dzabic M, Wolmer-Solberg N, Straat
K, Stragliotto G, Soderberg-Naucler C. 2013. Human cytomegalovirus infection levels in glioblastoma multiforme are of prognostic value for survival. J Clin Virol 57:36–42.
Rahbar A, Stragliotto G, Orrego A, Peredo I, Taher C, Willems J,
Soderberg-Naucler C. 2012. Low levels of human cytomegalovirus infection in glioblastoma multiforme associates with patient
survival; a case-control study. Herpesviridae 3:3.
Ranganathan P, Clark PA, Kuo JS, Salamat MS, Kalejta RF. 2012.
Significant association of multiple human cytomegalovirus genomic loci with glioblastoma multiforme samples. J Virol 86:854–
864.
Renzette N, Bhattacharjee B, Jensen JD, Gibson L, Kowalik TF.
2011. Extensive genome-wide variability of human cytomegalovirus in congenitally infected infants. PLoS Pathog 7:e1001344.
Sabatier J, Uro-Coste E, Pommepuy I, Labrousse F, Allart S,
Tremoulet M, Delisle MB, Brousset P. 2005. Detection of human
cytomegalovirusgenome and gene products in central nervous
system tumours. Br J Cancer 92:747–750.
Samanta M, Harkins L, Klemm K, Britt WJ, Cobbs CS. 2003. High
prevalence of human cytomegalovirus in prostatic intraepithelial
neoplasia and prostatic carcinoma. J Urol 170:998–1002.
Scheurer ME, Bondy ML, Aldape KD, Albrecht T, El-Zein R. 2008.
Detection of human cytomegalovirus in different histological
types of gliomas. Acta Neuropathol 116:79–86.
Shepp DH, Match ME, Ashraf AB, Lipson SM, Millan C, Pergolizzi
R. 1996. Cytomegalovirus glycoprotein B groups associated with
retinitis in AIDS. J Infect Dis 174:184–187.
Siew VK, Duh CY, Wang SK. 2009. Human cytomegalovirus UL76
induces chromosome aberrations. J Biomed Sci 16:107.
Sissons JG, Carmichael AJ. 2002. Clinical aspects and management
of cytomegalovirus infection. J Infect 44:78–783.
Slinger E, Maussang D, Schreiber A, Siderius M, Rahbar A, FraileRamos A, Lira SA, Soderberg-Naucler C, Smit MJ. 2010.
HCMV-encoded chemokine receptor US28 mediates proliferative
signaling through the IL-6-STAT3 axis. Sci Signal 3:ra58.
Soderberg-Naucler C. 2008. HCMV microinfections in inflammatory
diseases and cancer. J Clin Virol 41:218–223.
Soderberg-Naucler C, Rahbar A, Stragliotto G. 2013. Survival in
patients with glioblastoma receiving valganciclovir. N Engl J
Med 369:985–986.
Soroceanu L, Akhavan A, Cobbs CS. 2008. Platelet-derived growth
factor-alpha receptor activation is required for human cytomegalovirus infection. Nature 455:391–395.
Soroceanu L, Matlaf L, Bezrookove V, Harkins L, Martinez R,
Greene M, Soteropoulos P, Cobbs CS. 2011. Human cytomegalovirusUS28 found in glioblastoma promotes an invasive and
angiogenic phenotype. Cancer Res 71:6643–6653.
Speir E, Modali R, Huang ES, Leon MB, Shawl F, Finkel T, Epstein
SE. 1994. Potential role of human cytomegalovirus and p53
interaction in coronary restenosis. Science 265:391–394.
Straat K, Liu C, Rahbar A, Zhu Q, Liu L, Wolmer-Solberg N, Lou
F, Liu Z, Shen J, Jia J, Kyo S, Bjorkholm M, Sjoberg J,
Soderberg-Naucler C, Xu D. 2009. Activation of telomerase by
human cytomegalovirus. J Natl Cancer Inst 101:488–497.
HCMV Detection in Glioblastoma Multiforme
Trincado DE, Scott GM, White PA, Hunt C, Rasmussen L,
Rawlinson WD. 2000. Human cytomegalovirus strains associated
with congenital and perinatal infections. J Med Virol 61:481–
487.
Wiertz EJ, Jones TR, Sun L, Bogyo M, Geuze HJ, Ploegh HL. 1996.
The human cytomegalovirus US11 gene product dislocates MHC
class I heavy chains from the endoplasmic reticulum to the
cytosol. Cell 84:769–779.
Wolmer-Solberg N, Baryawno N, Rahbar A, Fuchs D, Odeberg J,
Taher C, Wilhelmi V, Milosevic J, Mohammad AA, Martinsson
T, Sveinbjörnsson B, Johnsen JI, Kogner P, Söderberg-Nauclér
C. 2013. Frequent detection of human cytomegalovirus in
neuroblastoma: A novel therapeutic target? Int J Cancer 133:
2351–2361. doi: 10.1002/ijc.28265
Yamamoto AY, Mussi-Pinhata MM, de Deus Wagatsuma
VM, Marin LJ, Duarte G, Figueiredo LT. 2007. Human cytomegalovirusglycoprotein B genotypes in Brazilian mothers
and their congenitally infected infants. J Med Virol 79:1164–
1168.
9
Zafiropoulos A, Tsentelierou E, Billiri K, Spandidos DA. 2003.
Human herpes viruses in non-melanoma skin cancers. Cancer
Lett 198:77–81.
Zekri AR, Mohamed WS, Samra MA, Sherif GM, El-Shehaby AM,
El-Sayed MH. 2004. Risk factors for cytomegalovirus, hepatitis
B and C virus reactivation after bone marrow transplantation.
Transpl Immunol 13:305–311.
Zheng SS ZL, Qian J, Cai T, Fan J, Ma WH. 2002. Cytomegalovirus
glycoprotein B sequence variation in Chinese liver transplant
recipients. Hepatobiliary Pancreat Dis Int 1:26–29.
Zhu H, Shen Y, Shenk T. 1995. Human cytomegalovirus IE1 and
IE2 proteins block apoptosis. J Virol 69:7960–7970.
SUPPORTING INFORMATION
Additional supporting information may be found in
the online version of this article at the publisher’s
web-site.
J. Med. Virol. DOI 10.1002/jmv