a
UNIVERSIDADE FEDERAL DE GOIÁS
PROGRAMA DE PÓS-GRADUAÇÃO EM MEDICINA TROPICAL
E SAÚDE PÚBLICA
MARINA PEDROSO DE OLIVEIRA
Rastreamento sorológico e molecular do vírus da hepatite B em homens que fazem
sexo com homens em Goiânia-Goiás, utilizando o método respondent-driven
sampling (RDS)
Goiânia
2017
MARINA PEDROSO DE OLIVEIRA
Rastreamento sorológico e molecular do vírus da hepatite B em homens que fazem
sexo com homens em Goiânia-Goiás, utilizando o método respondent-driven
sampling (RDS)
Tese de Doutorado apresentada ao
Programa de Pós-Graduação em Medicina
Tropical e Saúde Pública da Universidade
Federal de Goiás para obtenção do
Título de Doutor em Medicina Tropical
e Saúde Pública.
Orientadora: Profa. Dra. Regina Maria Bringel Martins
Coorientadora: Profa. Dra. Márcia Alves Dias de Matos
Este trabalho foi realizado com o auxílio financeiro do Ministério da Saúde/Secretaria de
Vigilância em Saúde/Departamento de DST, Aids e Hepatites Virais, através do Projeto
de Cooperação Técnica Internacional BRAK57 entre o Governo Brasileiro e o Escritório
das Nações Unidas sobre Drogas e Crime - UNODC.
Goiânia
2017
i
Ficha de identificação da obra elaborada pelo autor, através do
Programa de Geração Automática do Sistema de Bibliotecas da UFG.
Oliveira, Marina Pedroso de
Rastreamento sorológico e molecular do vírus da hepatite B em
homens que fazem sexo com homens em Goiânia-Goiás, utilizando o
método respondent-driven sampling (RDS) [manuscrito] / Marina
Pedroso de Oliveira. - 2017.
xv, 118 f.: il.
Orientador: Profa. Dra. Regina Maria Bringel Martins; co
orientadora Dra. Márcia Alves Dias de Matos.
Tese (Doutorado) - Universidade Federal de Goiás, Instituto de
Patologia Tropical e Saúde Pública (IPTSP), Programa de Pós
Graduação em Medicina Tropical e Saúde Pública, Goiânia, 2017.
Bibliografia. Anexos.
Inclui siglas, abreviaturas, símbolos, gráfico, tabelas, lista de
figuras, lista de tabelas.
1. Hepatite B. 2. HSH. 3. epidemiologia. 4. genótipos. 5. mutações. I.
Martins, Regina Maria Bringel , orient. II. Título.
CDU 579
DEDICATÓRIA
Aos homens que fazem sexo com homens que contribuíram
para realização deste estudo e me permitiram um
crescimento acadêmico e pessoal singular.
iii
AGRADECIMENTOS
Na vida estamos em constante evolução e aprendizado. A cada etapa cumprida
percebemos o quanto temos a agradecer. Assim, minha gratidão àqueles que
contribuíram direta ou indiretamente para realização deste sonho:
Primeiramente, agradeço a Deus por tantas bênçãos concedidas, por sempre me guiar
nas minhas escolhas e me dar forças para continuar e seguir em frente. Por ter colocado
nessa trajetória pessoas especiais que foram essenciais para cumprir mais essa etapa.
À minha orientadora, Professora Regina Maria Bringel Martins, exemplo de
pesquisadora, dedicação profissional e competência, que me guiou com sabedoria nessa
trajetória. Meus sinceros agradecimentos por compartilhar seus conhecimentos e pela
oportunidade de realizar o mestrado e doutorado sob sua orientação.
À minha coorientadora, Professora Márcia Alves Dias de Matos, por compartilhar
experiências, pela cumplicidade, paciência e pelas palavras de incentivo que me deram
força durante essa caminhada.
À Professora Carmen Luci Rodrigues Lopes pelo carinho, cuidado e contribuição ao
longo deste estudo. Obrigada por não medir esforços para nos auxiliar na implantação
e execução deste trabalho, sempre tão disposta e generosa.
À Professora Sheila Araújo Teles e ao Professor Marcos André Matos exemplos de
dedicação a pesquisa e humanismo. Obrigada por nos auxiliar na implantação deste
estudo e pelo apoio durante a realização do mesmo. A colaboração de vocês nos
enriquece bastante.
À Professora Megmar Aparecida dos Santos Carneiro pelos ensinamentos constantes
desde a graduação, a convivência com você contribui muito para meu crescimento
pessoal e profissional.
Aos alunos e ex-alunos do laboratório de virologia do IPTSP-UFG que tanto
contribuíram para meu crescimento acadêmico e me mostraram o quanto é enriquecedor
o trabalho em equipe. Ágabo Macedo, Andreia Andrade, Edna Santana, Nara Rúbia,
Nativa Helena, Lyriane Apolinário, Kamilla Nogueira, Juliana Menara, Lorena Santana,
Jerusa Marrielli, Gabryella Teixeira, Brunna Rodrigues, Raphael Brandão, Matheus
Aires, Mariana Oliveira, Nadia Rubia, Aline Kozlowski, Tamíris Marinho, Thais
Marinho e Tassia Marinho obrigada pelo companheirismo, pelos ombros amigos, pelas
palavras de incentivo e por tornarem essa trajetória mais leve. Vocês foram essenciais
para que eu chegasse até aqui.
Aos amigos e parceiros de projeto, Andreia Alves de Andrade, Edna Braz Rocha de
Santana e Ágabo Macedo Costa e Silva, o entusiasmo, compromisso e boa vontade de
vocês fez com que este trabalho fosse prazeroso de ser realizado.
À equipe do laboratório de virologia molecular do IOC/FIOCRUZ, em especial Dra.
Natalia Araujo, Natalia Spitz e Dra. Bárbara Lago, pela colaboração na realização dos
testes moleculares e pela gentileza de terem me recebido tão bem no laboratório e
compartilhado seus conhecimentos.
iv
Às colegas, Sueli Meira e Jildamáris Meira, pela disposição e auxílio prestado durante
as coletas de dados.
À Dra. Rosa Maria Salani Mota pela realização da análise estatística dos dados desta
tese.
Aos HSH participantes e às parcerias que estabelecemos para o desenvolvimento deste
estudo, em especial à Beth Fernandes e Edson Santana, vocês foram essenciais nesse
trajeto.
À banca de qualificação, Profa. Sheila Araújo Teles, Profa. Marília Dalva Turchi e Prof.
Marcos André Matos, pelas valiosas contribuições no aperfeiçoamento desta tese.
À Universidade Federal de Goiás que permitiu meu crescimento e amadurecimento
acadêmico desde a graduação até o doutorado. Tenho orgulho de ser UFG!
Aos docentes e funcionários do Programa de Pós-Graduação em Medicina Tropical e
Saúde Pública do Instituto de Patologia Tropical e Saúde Pública/UFG, pelos
ensinamentos e auxílio prestado ao longo desses anos.
Ao CNPq pela bolsa de incentivo a pesquisa que me permitiu dedicar integralmente ao
doutorado durante três anos.
Ao Ministério da Saúde e Escritório das Nações Unidas sobre Drogas e Crime (UNODC)
pelo financiamento do estudo.
Aos meu pais, Antônio Luiz e Maria Tereza, que apoiaram minhas escolhas e confiaram
em mim quando mais precisei. Vocês são meu porto seguro! Obrigada pelos exemplos de
vida e por tantos ensinamentos, dentre eles o valor do trabalho e do estudo.
Ao meu irmão, ao meu namorado, familiares e amigos, obrigada pelo carinho, paciência,
incentivo, amizade e pelos bons momentos que sempre me renovaram me dando forças
para continuar.
v
SUMÁRIO
LISTA DE FIGURAS ................................................................................................ viii
LISTA DE QUADROS ................................................................................................ ix
LISTA DE ANEXOS .................................................................................................... x
SÍMBOLOS, SIGLAS E ABREVIATURAS................................................................ xi
RESUMO .................................................................................................................. xiv
ABSTRACT ............................................................................................................... xv
1 INTRODUÇÃO ......................................................................................................... 1
1.1 Considerações iniciais.......................................................................................... 1
1.2 Classificação e características do vírus da hepatite B ........................................... 2
1.2.1 Estrutura do genoma...................................................................................... 4
1.3 Replicação do vírus da hepatite B ........................................................................ 6
1.4 Variabilidade do HBV ......................................................................................... 9
1.4.1 Subtipos sorológicos ..................................................................................... 9
1.4.2 Genótipos .................................................................................................... 10
1.4.3 Subgenótipos ............................................................................................... 12
1.4.4 Mutações no genoma ................................................................................... 13
1.5 Aspectos clínicos da hepatite B .......................................................................... 16
1.6 Patogenia da infecção pelo HBV ........................................................................ 19
1.7 Diagnóstico laboratorial da infecção pelo HBV ................................................. 20
1.8 Tratamento da hepatite B ................................................................................... 23
1.9 Epidemiologia da infecção pelo HBV ................................................................ 24
1.9.1 Transmissão ................................................................................................ 24
1.9.2 Distribuição da infecção pelo HBV ............................................................. 26
1.9.3 Distribuição dos genótipos e subgenótipos .................................................. 29
1.10 Prevenção e controle da infecção pelo HBV..................................................... 30
1.11 Hepatite B em homens que fazem sexo com homens........................................ 32
1.12 Métodos de amostragem em populações de difícil acesso ................................. 36
2 JUSTIFICATIVA .................................................................................................... 39
3 OBJETIVOS ............................................................................................................ 41
3.1 Objetivo geral .................................................................................................... 41
3.2 Objetivos específicos ......................................................................................... 41
4 RESULTADOS ....................................................................................................... 42
vi
4.1 Artigo 1 ............................................................................................................. 43
4.2 Artigo 2 ............................................................................................................. 70
5 DISCUSSÃO ........................................................................................................... 85
6 CONCLUSÕES ....................................................................................................... 91
7 REFERÊNCIAS....................................................................................................... 92
ANEXOS .................................................................................................................. 117
vii
LISTA DE FIGURAS
Figura 1 - Representação esquemática do vírus da hepatite B ........................................ 3
Figura 2 - Microscopia eletrônica do vírion e partículas subvirais do HBV .................... 3
Figura 3 - Organização genômica do HBV .................................................................... 4
Figura 4 - Ciclo replicativo do HBV.............................................................................. 8
Figura 5 - Algoritmo para determinar os subtipos do HBV a partir da estrutura primária
do gene S .................................................................................................................... 10
Figura 6 - Árvore filogenética com os genótipos do HBV, incluindo os propostos I e J 12
Figura 7 - Curso típico da hepatite B aguda ................................................................. 22
Figura 8 - Curso típico da infecção crônica pelo HBV ................................................. 22
Figura 9 - Prevalência do HBsAg no mundo, 1957-2013 ............................................ 27
Figura 10 - Representação gráfica de um recrutamento por RDS ................................ 38
viii
LISTA DE QUADROS
Quadro 1 - Mutações no genoma do HBV e suas implicações clínicas ......................... 16
Quadro 2 - Prevalência da infecção pelo HBV em diferentes grupos populacionais no
estado de Goiás ........................................................................................................... 28
Quadro 3 - Estudos de prevalência da infecção pelo vírus da hepatite B em homens que
fazem sexo com homens ............................................................................................. 35
ix
LISTA DE ANEXOS
Anexo 1 - Parecer do Comitê de Ética em Pesquisa ................................................... 117
Anexo 2 - Artigo 1: Prevalence, Risk Behaviors, and Virological Characteristics of
Hepatitis B Virus Infection in a Group of Men Who Have Sex with Men in Brazil: Results
from a Respondent-Driven Sampling Survey (artigo publicado) ................................. 118
x
SÍMBOLOS, SIGLAS E ABREVIATURAS
A
Alanina
Aa
Aminoácidos
ADF
Adefovir
ALT
Alanina Aminotransferase
Anti-HBc
Anticorpo Contra o Antígeno do Core do Vírus da Hepatite B
Anti-HBe
Anticorpo Contra o Antígeno “E” do Vírus da Hepatite B
Anti-HBs
Anticorpo Contra o Antígeno de Superfície do Vírus da Hepatite B
BCP
Promotora Basal do Core
cccDNA
DNA Circular Covalentemente Fechado
CDC
Centers for Disease Control and Prevention
CHC
Carcinoma Hepatocelular
DNA
Ácido Desoxirribonucleico
DR
Direct Repeats
DST
Doença Sexualmente Transmissível
ELISA
Enzyme Linked Immuno Sorbent Assay / Ensaio Imunoenzimático
Enh
Enhancers
ETV
Entecavir
HAV
Vírus da Hepatite A
HBV
Vírus da Hepatite B
HBcAg
Antígeno do Core do Vírus da Hepatite B
HBIG
Imunoglobulina Humana Anti-hepatite B
HBeAg
Antígeno “E” do Vírus da Hepatite B
HBsAg
Antígeno de Superfície do Vírus da Hepatite B
xi
HBxAg
Antígeno X do Vírus da Hepatite B
HCV
Vírus da Hepatite C
HDV
Vírus da Hepatite D
HEV
Vírus da Hepatite E
HIV
Vírus da Imunodeficiência
HLA
Antígeno Leucocitário Humano
HSH
Homens que Fazem Sexo com Homens
I
Isoleucina
ICTV
Comitê Internacional de Taxomonia do Vírus
Ig
Imunoglobulina
INF
Interferon
INF-α
Interferon Alfa
IST
Infecção Sexualmente Transmissível
Kb
Kilobases
LAM
Lamivudina
LdT
Telbivudina
LGBT
Lésbicas, Gays, Bissexuais e Transgêneros
M
Metionina
N
Asparagina
NK
Natural Killer
NTCP
Sodium-taurocholate co-transporting polypeptide
OMS
Organização Mundial da Saúde
ORF
Open Reading Frame / Região aberta de leitura
Pb
Pares de Bases
xii
PCR
Reação em Cadeia pela Polimerase
PEG-INF-α Interferon Alfa Peguilado
pgRNA
RNA pré-genômico
PNI
Programa Nacional de Imunização
R
Arginina
RNA
Ácido Ribonucleico
RNAm
RNA Mensageiro
RNAse H
Ribonuclease H
RT
Transcriptase Reversa
SUS
Sistema Único de Saúde
T
Treonina
TDF
Tenofovir
TGG
Triptofano
TNF
Fator de Necrose Tumoral
TP
Proteína Terminal
V
Valina
xiii
RESUMO
Homens que fazem sexo com homens (HSH) apresentam maior vulnerabilidade para
infecção pelo vírus da hepatite B (HBV) quando comparados à população em geral. No
Brasil, o perfil epidemiológico da hepatite B em HSH ainda é pouco conhecido. Este
estudo teve como objetivos estimar a prevalência da infecção pelo HBV em HSH em
Goiânia-Goiás e analisar os fatores associados, realizar a caracterização molecular dos
isolados virais, bem como investigar a situação vacinal contra hepatite B e fatores
associados. Estudo transversal conduzido em HSH na região metropolitana de GoiâniaGO. De março a novembro de 2014, um total de 522 participantes foi recrutado utilizando
o método respondent-driven sampling (RDS). Após assinatura do termo de
consentimento livre e esclarecido, os HSH foram entrevistados e amostras sanguíneas
coletadas. Todas as amostras foram testadas por ensaio imunoenzimático (ELISA) para
detecção dos marcadores sorológicos da hepatite B e submetidas à extração e
amplificação do HBV DNA. Os isolados do HBV foram sequenciados para determinação
dos genótipos e subgenótipos do vírus por análise filogenética e para identificação de
mutações no genoma viral. Os dados foram analisados utilizando os programas RDSAT
e SPSS. A prevalência global da infecção pelo HBV (anti-HBc) foi de 15,4% (IC 95%:
8,7-25,8) e do HBsAg de 0,6% (IC 95%: 0,2-1,6). Idade acima de 25 anos, sexo anal
receptivo, relação sexual com mulheres e história de infecções sexualmente
transmissíveis (IST) foram fatores associados à infecção pelo HBV. O DNA viral foi
detectado apenas nos indivíduos HBsAg positivos, não sendo observada infecção oculta
na população estudada. Os isolados do HBV foram classificados como pertencentes ao
genótipo A (subgenótipos A1 e A2) do HBV. Mutações nas regiões S (T131N), promotora
basal do core (BCP) (A1762T/G1764A) e Pré-C/C (G1862T/G1888A e G1862T) do
genoma viral foram identificadas. Cerca de 40% (IC 95%: 32,3-48,8) dos participantes
tinham evidência sorológica de vacinação contra hepatite B (anti-HBs isolado), enquanto
que 76,2% relataram ter recebido a vacina previamente. Além disso, 44,3% (IC 95%:
36,1-52,9) dos HSH eram suscetíveis à infecção pelo HBV. Observou-se uma maior
positividade para anti-HBs isolado entre os HSH com até 25 anos de idade, seguido de
seu declínio com o aumento da idade e, por outro lado, verificou-se aumento da infecção
pelo HBV. A vacinação contra a hepatite B foi associada ao sexo anal desprotegido e
marginalmente à história de IST. Neste estudo, notou-se, ainda, uma baixa concordância
entre evidência sorológica e auto relato de vacinação (k = 0,17). Estes resultados revelam
uma prevalência global elevada da infecção pelo HBV na população estudada e sua
associação com comportamentos sexuais de risco e, em contraste, uma frequência baixa
de vacinação contra hepatite B, evidenciando a necessidade de políticas públicas
contínuas de saúde voltadas para os HSH, incluindo estratégias para aumentar a cobertura
vacinal, além do monitoramento dos indivíduos portadores do HBV.
Palavras-chave: Hepatite B, HSH, epidemiologia, vacinação, genótipos, mutações.
xiv
ABSTRACT
Men who have sex with men (MSM) are more vulnerable to hepatitis B virus (HBV)
infection when compared to the general population. In Brazil, the epidemiological profile
of hepatitis B in MSM is still poorly understood. This study aimed to estimate the
prevalence of HBV infection in MSM in Goiânia-Goiás and to analyze the associated
factors, perform a molecular characterization of the viral isolates, as well as to investigate
the vaccine situation against hepatitis B in this population. A cross-sectional study was
conducted among MSM in the City of Goiânia, Central Brazil. From March to November
2014, a total of 522 participants were recruited using respondent-driven sampling (RDS).
After signing the consent form, MSM were interviewed and a blood sample was collected.
All samples were tested for HBV serological markers and HBV DNA. HBV isolates were
sequenced for the determination of HBV genotypes and subgenotypes by phylogenetic
analysis and for identification of mutations in viral genome. Data were analyzed using
the RDSAT and SPSS programs. The overall prevalence of HBV infection (presence of
anti-HBc marker) was 15.4% (95% CI: 8.7-25.8) and the rate of HBsAg carriers was 0.6%
(95% CI: 0.2-1.6). Age over 25 years old, receptive anal intercourse, previous sex with
women, and history of sexually transmitted infection (STI) were factors associated with
HBV infection. Viral DNA was detected only in HBsAg-positive individuals, and occult
HBV infection was not observed in the study population. HBV isolates were classified
into genotype A (subgenotypes A1 and A2). Mutations in the S (T131N), basal core
promoter (BCP) (A1762T/G1764A) and Pre-C/C (G1862T/G1888A and G1862T)
regions of the HBV genome were identified. About 40% (95% CI: 32.3-48.8) of the
participants had serological evidence of previous HBV vaccination (reactive for isolated
anti-HBs), while 76.2% reported having previously received the vaccine. In addition,
44.3% (95% CI: 36.1-52.9) of MSM were susceptible to HBV infection. A greater
frequency of positivity for anti-HBs alone was observed among MSM up to 25 years old,
followed by declining vaccination with increasing age. By contrast, an increase in HBV
infection with increasing age was found. HBV vaccination was associated with
unprotected anal intercourse and history of STI (with a borderline p-value). In this study,
we observed a poor agreement when comparing the self-reported and serologic evidence
of HBV vaccination (k = 0.17). These results reveal a high overall prevalence of HBV
infection in the study population associated with sexual risk behaviors, and in contrast, a
low frequency of hepatitis B vaccination, evidencing a need for public health strategies
to increase vaccine coverage in MSM, in addition to monitoring HBV carriers.
Key words: Hepatitis B, MSM, epidemiology, vaccination, genotypes, mutations.
xv
1 INTRODUÇÃO
1.1 Considerações iniciais
Hepatites virais são infecções provocadas por diferentes vírus hepatotrópicos
que, embora classificados em diferentes famílias, compartilham a capacidade comum de
se replicar no fígado (THOMAS; YONEDA; SCHIFF, 2015). Os principais agentes
etiológicos que causam hepatites virais descritos até o momento são: vírus da hepatite A
(HAV) (FEINSTONE; KAPIKIAN; PURCELI, 1973), vírus da hepatite B (HBV)
(DANE; CAMERON; BRIGGS, 1970), vírus da hepatite C (HCV) (CHOO et al., 1989),
vírus da hepatite delta (HDV) (RIZZETO et al., 1977) e vírus da hepatite E (HEV)
(BALAYAN et al., 1983).
Em relação à descoberta do HBV, vale destacar que, no ano de 1965,
Blumberg e colaboradores descobriram, em uma amostra de soro de aborígine
australiano, um antígeno que reagia especificamente com um anticorpo presente no soro
de pacientes hemofílicos politransfundidos, denominando-o de antígeno Austrália (Au)
(BLUMBERG; ALTEN; VISNICH, 1965). Posteriormente, Dane, Cameron, Briggs
(1970) identificaram, por microscopia eletrônica, a partícula completa do vírus da
hepatite B a partir do soro de portadores do antígeno Austrália, sendo atualmente
conhecido como antígeno de superfície do HBV (HBsAg).
A hepatite B representa um importante problema de saúde pública com
distribuição global. Cerca de 240 milhões de pessoas no mundo são portadores crônicos
do HBV, sendo que a forma crônica dessa infecção está associada a uma variedade de
manifestações clínicas, que vão desde um estado de portador assintomático a
complicações hepáticas graves, incluindo cirrose e carcinoma hepatocelular (CHC)
(WHO, 2015a).
A prevalência da hepatite B no mundo é variável, sendo a África subsaariana
e parte da Ásia consideradas regiões de alta endemicidade, com prevalência para o
HBsAg maior ou igual a 8%. Países do leste e sul da Europa, regiões das Américas do
Sul e Central, Oriente Médio e África apresentam taxas intermediárias para o HBV (27%). Já prevalências baixas, com positividade para o HBsAg menor que 2% são
encontradas em parte das Américas, Europa Ocidental, Austrália e Japão (LOCARNINI
et al., 2015; SCHWEITZER et al., 2015). O Brasil é considerado um país com
endemicidade baixa para o HBV, segundo o estudo de prevalência de base populacional
1
realizado nas capitais brasileiras, no qual a prevalência estimada para o HBsAg foi de
0,37% na população geral (BRASIL, 2010a; PEREIRA et al., 2009).
O HBV é transmitido de forma eficiente pelas vias vertical, sexual e
parenteral/percutânea (HOU; LIU; GU, 2005; KWON; LEE, 2011; LOCARNINI et al.,
2015). No Brasil, a transmissão do vírus ocorre pela via parenteral e, sobretudo, pela via
sexual, a qual é uma das principais causas de infecção pelo vírus da hepatite B (BRASIL,
2008; PEREIRA et al., 2009).
Estratégias de prevenção e controle da infecção pelo HBV incluem mudanças
comportamentais sexuais e condutas que evitem a exposição ao sangue e outros fluidos
corporais, diagnóstico precoce, tratamento dos portadores crônicos e a vacinação contra
o HBV, a qual é a medida preventiva mais segura e eficaz (BRASIL, 2009; FRANCO et
al., 2012; KWON; LEE, 2011; LOCARNINI et al., 2015; WHO, 2012; 2015a).
Nota-se que alguns grupos populacionais, como os homens que fazem sexo
com homens (HSH), apresentam taxas de prevalência de hepatite B superiores às
encontradas na população em geral (CHOW et al., 2014; SOARES et al., 2014; TSENG
et al., 2012). A maior vulnerabilidade desse grupo está relacionada especialmente à
transmissão associada ao sexo anal desprotegido, múltiplos parceiros sexuais, histórico
de infecção sexualmente transmissível (IST), estigma social, violência e a dificuldade de
acesso aos serviços de saúde (CDC, 2015a; DE VRIES, 2014; RISHER et al., 2013;
SABIDÓ et al., 2015).
1.2 Classificação e características do vírus da hepatite B
O vírus da hepatite B é classificado na família Hepadnaviridae, gênero
Orthohepadnavirus (ICTV, 2015). A partícula completa do HBV (vírion), também
denominada partícula de Dane, mede aproximadamente 42 nm de diâmetro. O vírion
apresenta, externamente, um envelope lipoproteico constituído pelo HBsAg e,
internamente, um nucleocapsídeo icosaédrico formado pela proteína ou antígeno do core
(HBcAg), onde se encontra o material genético (DNA) associado a enzima DNA
polimerase/transcriptase reversa (Figura 1) (DOO; GHANY, 2010; LIANG, 2009;
SEEGER; MASON, 2015).
2
Figura 1 - Representação esquemática do vírus da hepatite B (modificada)
Fonte: http://pt.dreamstime.com/imagem-de-stock-royalty-free-v%C3%ADrus-dahepatite-b-image22144156
Além do vírion, partículas subvirais ou incompletas são observadas, por
microscopia eletrônica, no soro de pacientes infectados pelo HBV, nas formas esféricas
e tubulares (Figura 2). Essas partículas não infecciosas medem cerca de 20-22 nm de
diâmetro, sendo constituídas principalmente pelo HBsAg e desprovidas do genoma do
vírus (DOO; GHANY, 2010; GERBER et al., 1974; GLEBE; BREMER, 2013; LIANG,
2009).
Figura 2 - Microscopia eletrônica do vírion e partículas subvirais do HBV (modificada)
Fonte: http://www.hepb.org/hepb/hepatitis_b_virus.htm
3
1.2.1 Estrutura do genoma
O genoma do vírus da hepatite B é um dos menores dentre os vírus que
infectam humanos. É formado por uma molécula de DNA circular de fita parcialmente
dupla, com cerca de 3.200 pares de bases (pb). A fita maior tem polaridade negativa,
sendo complementar ao RNA mensageiro (RNAm). A extremidade 5’ dessa fita está
covalentemente ligada à polimerase viral. Já a fita incompleta possui polaridade positiva
e comprimento variável (DOO; GHANY, 2010; NASSAL, 2015).
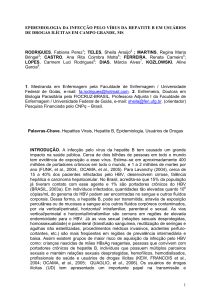
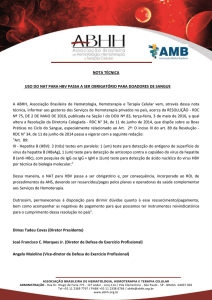
O genoma do HBV é organizado em quatro fases abertas de leitura (Open
Reading Frame - ORF) parcialmente sobrepostas, denominadas Pré-S/S, Pré-C/C, P e X
(Figura 3). Para regulação da atividade gênica há dois elementos potencializadores da
transcrição (enhancers) Enh I e Enh II e, próxima a extremidade de ambas as fitas,
observa-se duas pequenas sequências de nucleotídeos denominadas DR1 e DR2 (Direct
Repeats), importantes na iniciação da replicação do HBV (GANEM; VARMUS, 1987;
LIANG, 2009; NASSAL, 2015; SEEGER; MASON, 2015).
Figura 3 - Organização genômica do HBV. O esquema mostra as quatro fases de leitura
aberta (ORF) do genoma: Pré-S/S, Pré-C/C, P e X. As linhas externas representam os
transcritos virais, enquanto que as pontas das setas indicam os inícios de transcrição; ε
simboliza o sinal de encapsidação no RNA pré-genômico (pg). A organização é compacta
com sobreposição das ORFs e elementos regulatórios, em que as setas verdes indicam os
promotores, Enh I e Enh II são os potencializadores de transcrição, DR1 e DR2 são
repetições diretas.
Fonte: Nassal (2015)
4
Fase de leitura aberta Pré-S/S
A região Pré-S/S codifica as proteínas de superfície denominadas L (large),
M (middle) e S (small), as quais constituem o HBsAg (SEEGER; MASON, 2015). A
leitura a partir do códon de iniciação Pré-S1, seguido do Pré-S2 e S, codifica a proteína
L, com 389 aminoácidos (aa). Essa proteína contém sítios de ligação do HBV aos
receptores específicos nos hepatócitos, além de epítopos que induzem a produção de
anticorpos neutralizantes para o vírus (CHEN et al., 2013; NEURATH et al., 1986;
SEEGER; MASON, 2000). A síntese da proteína M (281 aa) é codificada a partir do
códon de iniciação da região Pré-S2, seguida pela S. A referida proteína possui uma
região que mimetiza a albumina sérica humana, a qual tem importância na adsorção do
vírus (DASH et al., 1991; THUNG; GERBER, 1984). A proteína S (226 aa), principal
componente do envelope, é sintetizada pela região S, sendo capaz de induzir a formação
de anticorpos específicos com atividade neutralizante e protetora, independente do
subtipo viral. Por essa razão, esse antígeno é utilizado na produção de vacinas contra a
hepatite B (HOLLINGER, 2007; SEEGER; MASON, 2000, 2015).
Fase de leitura aberta Pré-C/C
A região Pré-C/C possui dois códons de iniciação na mesma ORF. A região
C codifica o HBcAg, uma proteína com 183 aa que compõe o nucleocapsídeo viral
(LIANG, 2009; NASSAL; SCHALLER, 1996; YANO; AZUMA; HAYASHI, 2015). O
HBcAg não é detectado no soro de pacientes infectados pelo HBV, uma vez que está
presente nos hepatócitos do hospedeiro. Essa proteína é capaz de interagir com o genoma
humano em células do fígado infectadas, podendo ligar-se a vários promotores de genes
e, assim, pode ter implicações na patogenicidade da infecção pelo HBV. Por outro lado,
o HBcAg induz a produção de anticorpos (anti-HBc), detectáveis no soro nas frações de
imunoglobulinas (Ig) M ou IgG (KAY; ZOLIUM, 2007; MILICH; MCLACHALAM,
1986; OZKAL-BAYDIN, 2014).
A transcrição iniciada na região Pré-C dá origem ao antígeno “e” do HBV
(HBeAg), um peptídeo de 29 aa, solúvel, secretado pelos hepatócitos e liberado na
corrente sanguínea, o qual é considerado um importante marcador de replicação viral
ativa (KAY; ZOLIUM, 2007; SEEGER; MASON, 2015; YANO; AZUMA; HAYASHI,
2015).
5
Fase de leitura aberta P
A ORF P, também denominada região da polimerase, se sobrepõe às demais
regiões do genoma do HBV, sendo a mais extensa delas. Essa região codifica uma
proteína de 843 aminoácidos, que possui quatro domínios funcionais. O primeiro é o
domínio aminoterminal, que atua como proteína terminal (TP) ou iniciador, responsável
pelo início da síntese da fita de DNA de polaridade negativa. O segundo, chamado de
região espaçadora, atua como uma conexão entre os domínios. O terceiro, denominado
domínio da transcriptase reversa (RT), codifica a DNA-polimerase RNA-dependente. O
último é o domínio carboxiterminal, o qual codifica a ribonuclease H (RNAse H),
responsável por degradar o RNA pré-genômico e facilitar a replicação (CHEN et al.,
2013; LIANG, 2009; SEEGER; MASON, 2015).
Fase de leitura aberta X
A menor região do genoma viral, ORF X, codifica HBx, uma proteína
regulatória com aproximadamente 154 aa, que está presente no citoplasma e, em menor
quantidade, no núcleo dos hepatócitos de pacientes infectados pelo HBV. Essa proteína
possui papel crucial na infecção e replicação viral, além de ter implicação na patogênese
do carcinoma hepatocelular (CROSS; WEN; RUTTER, 1993; OZKAL-BAYDIN, 2014;
ZHANG; WANG; YE, 2014). Os mecanismos moleculares envolvendo HBx como
mediador da hepatocarcinogênese ainda precisam ser melhor elucidados. Entretanto,
quatro mecanismos têm sido descritos para explicar o potencial oncogênico dessa
proteína, que incluem a transativação ou repressão de genes ligados à proliferação celular,
interação com proteínas relacionadas à resposta celular para o processo oncogênico,
ativação de células pelas vias de sinalização e ainda mudanças epigenéticas, tais como:
metilação de DNA, modificação de histonas e expressão de micro-RNA (RAJPUT;
SHUKLA; KUMAR, 2015; SHLOMAI; DE JONG; RICE, 2014; ZHANG et al., 2015;
ZHU et al., 2015).
1.3 Replicação do vírus da hepatite B
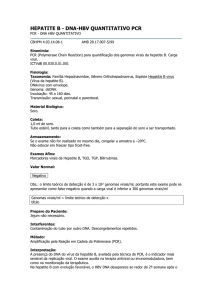
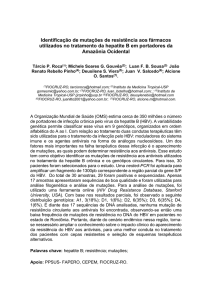
A Figura 4 apresenta as principais etapas do ciclo replicativo do HBV.
Inicialmente, há uma interação de alta afinidade entre a região aminoterminal da proteína
6
de superfície L do vírus com o receptor NTCP (sodium-taurocholate co-transporting
polypeptide), um transportador transmembrana múltiplo, predominantemente expresso
nos hepatócitos. Recentemente, foi demonstrado que o NTCP é o receptor para adsorção
do HBV, sendo responsável pela penetração do vírus para o interior da célula,
provavelmente por endocitose (BAUMERT et al., 2014; NASSAL, 2015; NI et al., 2014;
YAN et al., 2012).
Após a penetração, a partícula viral sofre o desnudamento, uma série de
transformações que envolvem a desmontagem da bicamada lipídica e a dissolução do
nucleocapsídeo. No núcleo da célula hospedeira, o DNA viral é convertido a uma forma
circular covalentemente fechada (cccDNA) por ação da DNA polimerase, sendo esse de
grande importância na persistência da infecção (DOO; GHANY, 2010; LOCARNINI;
ZOULIM, 2010; NASSAL, 2015; TUTTLEMAN; POURCEL; SUMMERS, 1986). O
genoma do HBV possui a capacidade de integrar ao DNA celular do hospedeiro. Essa
integração pode induzir vários tipos de alterações genéticas secundárias incluindo
deleções, translocações e instabilidade genômica, as quais estão relacionadas ao
desenvolvimento de CHC (DOO; GHANY, 2010; LOCARNINI; ZOULIM, 2010;
YANO; AZUMA; HAYASHI, 2015).
Pela ação da enzima celular RNA polimerase II, o cccDNA é transcrito em
quatro RNAs virais de tamanhos distintos (3,5; 2,4; 2,1 e 0,7 Kb), os quais são
transportados para o citoplasma. O RNA maior (3,5 Kb) é bifuncional, servindo como
mensageiro para tradução das proteínas do core, “e” e da polimerase viral, bem como
molde para transcrição reversa da fita negativa do DNA viral (nesse caso, denominado de
RNA pré-genômico ou pgRNA). A proteína L do HBsAg é traduzida a partir do RNAm
de 2,4 Kb, enquanto as proteínas M e S pelo de 2,1 Kb, e o HBxAg é resultado da tradução
do RNAm de 0,7 Kb (BECK; NASSAL, 2007; GAO; DUAN; COFFIN, 2015; LIANG,
2009; LOCARNINI; ZOULIM, 2010).
Após a tradução das proteínas o pgRNA é encapsidado juntamente com a
polimerase viral. Esse processo é iniciado pela ligação coordenada da polimerase viral
com a estrutura secundária stem-loop, chamada épsilon (ε), no pgRNA, o que desencadeia
a encapsidação pela proteína do core para formar o nucleocapsídeo viral. Após essa
ligação, a polimerase serve como uma proteína inicializadora para a síntese da fita
negativa do DNA. Em seguida, o pgRNA é degradado pela ribonuclease viral e a fita
positiva de DNA é sintetizada utilizando a fita negativa recém-sintetizada como molde.
Por fim, o genoma circulariza formando um DNA circular de fita parcialmente dupla
7
dentro do nucleocapsídeo (BECK; NASSAL, 2007; GAO; DUAN; COFFIN, 2015;
SEEGER; MASON, 2015).
O nucleocapsídeo interage com a proteína do envelope no retículo
endoplasmático para formar as partículas completas, que são liberadas para o meio
extracelular. Em alternativa, as partículas de nucleocapsídeo contendo o genoma viral
podem também ser recicladas para o núcleo celular, onde seus DNAs genômicos podem
ser convertidos em cccDNA, mantendo um estoque intranuclear estável de moldes
transcricionais na célula sem a necessidade de múltiplos ciclos de reinfecção (BECK;
NASSAL, 2007; DOO; GHANY, 2010; GISH et al., 2015; SEEGER; MASON, 2015).
Figura 4 - Ciclo replicativo do HBV (modificada)
Fonte: Jayalakshmi, Kalyanaraman e Pitchappan (2013)
8
1.4 Variabilidade do HBV
1.4.1 Subtipos sorológicos
Após a descoberta do HBV, verificou-se a heterogeneidade do HBsAg, o que
permitiu classificar esse vírus em subtipos com base nos determinantes antigênicos.
Existe uma região comum que consiste no domínio principal antigênico denominado
determinante “a”, cujos aminoácidos estão localizados na posição 124 a 147 do genoma
do HBV. Essa região é altamente conservada e representa o epítopo principal para induzir
resposta imunológica protetora. O determinante “a” está localizado na região hidrofílica
principal (MHR) da proteína S (aa 103 e 173) (GAO; DUAN; COFFIN, 2015; YANO;
AZUMA; HAYASHI, 2015).
Em relação aos demais determinantes antigênicos, Le Bouvier, em 1971,
descreveu dois desses determinantes, d e y, os quais são mutualmente exclusivos (LE
BOUVIER, 1971). No ano de 1972, Bancroft, Mundon e Russell (1972) identificaram
dois determinantes adicionais, w e r. A partir de então, observaram que cada amostra de
HBV poderia ser classificada em quatro subtipos: adw, adr, ayw ou ayr.
Posteriormente, nove subtipos foram descritos por Couroucé-Pauty, Plançon
e Soulier (1983), denominados adw2, adw4, ayw1, ayw2, ayw3, ayw4, adrq+, adrq- e ayr.
Mais tarde, Arauz-Ruiz et al. (2002) sugeriram o décimo subtipo, adw3. Com a utilização
de técnicas moleculares, tornou-se claro que os determinantes dos subtipos eram
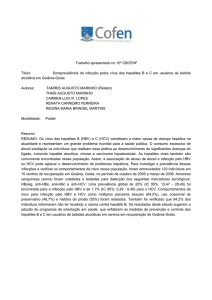
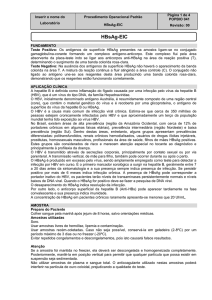
resultados de mutações na região S. Como apresentado na Figura 5, as substituições de
aminoácidos na posição 122 do gene S estão associadas às variações alélicas d, quando
nessa posição encontra-se uma lisina, ou y, quando o aa é uma arginina. Já as alterações
lisina/arginina na posição 160 determinam as variantes w/r, respectivamente. As
mutações na posição 127 estão relacionadas às subespecificidades do subdeterminante w,
sendo prolina w1/w2, treonina w3 ou leucina w4. Os demais determinantes têm sido
relacionados a mudanças em aminoácidos nas posições 134, 144, 145, 158, 159, 177 e
178 (KAY; ZOULIM, 2007; KIDD-LJUNGGREN; MIYAKAWA; KIDD, 2002;
NORDER; COUROUCE; MAGNIUS, 1992; OKAMOTO et al., 1988; YANO;
AZUMA; HAYASHI, 2015).
Na literatura, foi demonstrada associação entre os subtipos sorológicos e os
genótipos do HBV. Assim, a subtipagem/genotipagem dos isolados é útil para mapear a
distribuição geográfica do vírus e sua disseminação em determinados grupos
9
populacionais (KRAMVIS, 2014; LOCARNINI et al., 2013; YANO; AZUMA;
HAYASHI, 2015).
Figura 5 - Algoritmo para determinar os subtipos do HBV a partir da estrutura primária
do gene S (modificada)
Fonte: Yano, Azuma e Hayashi (2015)
1.4.2 Genótipos
A classificação do HBV em genótipos é baseada na divergência superior a
7,5% na sequência de nucleotídeos do genoma completo do vírus (KRAMVIS, 2014).
Inicialmente, Okamoto et al. (1988) verificaram a existência de quatro grupos,
denominados de A a D. Em seguida, Norder et al. (1992) descreveram outros dois
genótipos (E e F), após análises comparativas da região S. Posteriormente, o genótipo G
foi identificado por Stuyver et al. (2000), num estudo em doadores de sangue na França
e Estados Unidos. O genótipo H foi descrito na América Central por Arauz-Ruiz et al.
(2002).
Dois novos genótipos foram propostos: I, identificado no Vietnã (TRAN;
TRINH; ABE, 2008), e J, no Japão (TATEMATSU et al., 2009). Estudos apontam que o
genótipo I é a recombinação dos genótipos A/C/G com um genótipo indeterminado,
enquanto que o genótipo J é recombinante do genótipo C com um isolado de macaco
gibão (KRAMVIS, 2014; LOCARNINI et al., 2013). Assim, mais estudos são necessários
10
para elucidar a classificação desses genótipos (KURBANOV; TANAKA; MIZOKAMI,
2010; POURKARIM et al., 2014). A Figura 6 apresenta a árvore filogenética incluindo
os isolados I e J.
A variabilidade genética do HBV pode ser responsável por diferenças na
história natural da infecção, apresentando, portanto, implicações nas manifestações
clínicas e na resposta à terapia antiviral (KRAMVIS, 2014; LOCARNINI et al., 2013;
YANO; AZUMA; HAYASHI, 2015). Pacientes infectados com o genótipo A ou B
respondem melhor ao tratamento com interferon em relação aqueles com o genótipo C ou
D. Portadores dos genótipos A, B, D ou F apresentam soroconversão do HBeAg
precocemente e com maior frequência quando comparados aos indivíduos com o genótipo
C. Adicionalmente, o genótipo B está associado à progressão para cirrose hepática e CHC
em idade precoce, podendo ainda levar à hepatite fulminante. Infecções com o genótipo
C mostram maior risco de inflamação e fibrose hepática, cirrose e CHC do que às
observadas com outros genótipos. O genótipo D está relacionado à doença hepática menos
grave, comparativamente ao A e F. Pacientes infectados com o genótipo E têm uma maior
frequência de positividade para o HBeAg e cargas virais mais elevadas em relação aos
portadores do genótipo D. O genótipo F está associado ao desenvolvimento de CHC em
pacientes jovens e hepatite fulminante em coinfectados com o HDV, enquanto o G parece
acelerar a fibrose hepática. Quanto aos genótipos H, I e J, ainda não há relatos a respeito
de suas implicações clínicas (ARAÚJO; WAIZBORT; KAY, 2011; CROAGH;
DESMOND; BELL, 2015; KRAMVIS, 2014; LIN; KAO, 2011; MCMAHON, 2009;
NABUCO et al., 2012; OZASA et al., 2006).
11
Figura 6 - Árvore filogenética com os genótipos do HBV, incluindo os propostos I e J
(modificada)
Fonte: Araújo, Waizbort e Kay (2011)
1.4.3 Subgenótipos
Subgenótipos são grupos dentro do mesmo genótipo que apresentam
divergências na sequência nucleotídica do genoma superior a 4% e inferior a 7,5%.
Diferenças menores que 4% são chamadas de clados (KRAMVIS, 2014; POURKARIM
et a., 2014).
Com exceção dos genótipos E, G, H e J, os demais são subdivididos em
subgenótipos: A (A1 - A7), B (B1 - B9), C (C1 - C16), D (D1 - D9), F (F1 - F4) e I (I1 I2) (HÜBSCHEN et al., 2011; HUY et al., 2006; KRAMVIS, 2014; MULYANTO et al.
2012; OZARAS et al., 2015; POURKARIM et al., 2014; THEDJA et al., 2011).
12
Alguns desses subgenótipos propostos ainda são considerados provisórios por
apresentarem uma divergência nucleotídica muito pequena em relação a outros descritos.
Um dos erros mais comuns na caracterização inadequada de subgenótipos é a realização
da análise filogenética de uma sequência genômica parcial ao invés da análise do genoma
completo. Novas investigações neste campo requerem critérios padronizados para melhor
caracterização
e
subtipagem
(KURBANOV;
TANAKA;
MIZOKAMI,
2010;
POURKARIM et al., 2014).
1.4.4 Mutações no genoma
O genoma do HBV evolui rapidamente ao longo do tempo. As elevadas taxas
de replicação (1012 vírions produzidos por dia) e de erros da transcriptase reversa resultam
em uma significativa variabilidade viral. A enzima RT não possui atividade de revisão
para reparar nucleotídeos incorporados incorretamente, gerando, assim, uma taxa
estimada de substituições de 1,4 - 3,2 x 10-5 por sítio/ano. Essa estratégia de replicação
está relacionada a maioria das mutações pontuais, deleções e inserções observadas no
genoma do HBV. Além disso, tais variações podem ocorrer naturalmente por pressão da
resposta imune do hospedeiro, patogênese da doença hepática e uso de terapia antiviral
(GAO; DUAN; COFFIN, 2015; LAZAREVIC, 2014; OKAMOTO et al., 1987; YANO;
AZUMA; HAYASHI, 2015; WARNER; LOCARNINI, 2014).
Mutações na região Pré-S/S
O HBsAg é a principal proteína do envelope viral, apresentando as regiões
envolvidas na ligação do vírus ao hepatócito e também os principais epítopos
reconhecidos pelos anticorpos neutralizantes. Variações no determinante “a” dessa
proteína podem afetar a antigenicidade do HBsAg levando ao escape vacinal e diminuição
da expressão do HBsAg, o que impede a detecção desse antígeno por testes sorológicos
(infecção oculta), além de afetar a resposta à terapia utilizando imunoglobulinas contra
hepatite B (Quadro 1) (GAO; DUAN; COFFIN, 2015; JARAMILLO; NAVAS, 2015;
LAZAREVIC, 2014; POLLICINO et al., 2014; YANO; AZUMA; HAYASHI, 2015). A
primeira mutação de escape vacinal descrita na literatura foi a troca de uma glicina (G)
por arginina (R) na posição 145 (G145R) (CARMAN et al., 1990). Após essa descoberta,
outras mutações vêm sendo relatadas na região Pré-S/S, como é o caso da substituição de
13
uma treonina (T) por uma asparagina (N) ou por uma isoleucina (I) no aminoácido 131
(T131N/I). Essa mutação tem sido sugerida como um polimorfismo natural dos genótipos
A e G, estando associada à persistência do HBV mesmo após a perda do HBsAg e
soroconversão para anti-HBs, bem como ao escape vacinal. Além disso, um N na posição
131 pode também gerar um novo sítio de glicosilação, principalmente na presença da
mutação M133T/S, propiciando a secreção do vírus (DATTA et al., 2006; ITO et al.,
2010; SONG et al., 2009; SVICHER et al., 2011). Ainda, deleções na região pré-S têm
sido relacionadas à ocorrência de CHC (CROAGH; DESMOND; BELL, 2015; LIU et
al., 2009; ZHANG; DING, 2015).
Mutações na região Pré-C/C
Mutações nas regiões Pré-C e promotora basal do core (BCP) estão
relacionadas à diminuição da expressão do HBeAg, bem como à evolução para doença
hepática grave, incluindo hepatite aguda fulminante ou CHC (Quadro 1). Ainda, alguns
estudos sugerem que alterações nessas regiões podem afetar a resposta ao tratamento com
interferon (CROAGH; DESMOND; BELL, 2015; GAO; DUAN; COFFIN, 2015;
LAZAREVIC, 2014; YANG et al., 2013).
A mutação mais frequente relatada na região Pré-C caracteriza-se pela
substituição de uma guanina (G) por adenina (A) na posição 1896 (G1896A), o que resulta
na conversão do códon 28 (triptofano: TGG) a outro de finalização prematuro (TAG),
impedindo, assim, a tradução do precursor do HBeAg, e consequentemente esse antígeno
não é expresso (HUNT et al., 2000; KAMIJO et al., 2015; LAZAREVIC, 2014; LIAO et
al., 2012; ZHAND et al., 2015). Outras mutações nessa região têm sido descritas na
literatura, tais como: a variação G1862T, encontrada em casos de hepatite fulminante e
de forma predominante em isolados do subgenótipo A1 (CHANDRA et al., 2007;
LAZAREVIC, 2014), e a substituição G1888A, que também é uma característica do
subgenótipo A1, relacionada a alteração do códon de iniciação da proteína do core,
diminuindo a sua tradução (KIMBI; KEW; KRAMVIS, 2012).
Mutações na região BCP modulam a secreção do HBeAg, diminuindo a
expressão desse marcador por mecanismos transcricionais e, em contrapartida, podem
favorecer o aumento da replicação viral (HU et al., 2015; KAMIJO et al., 2015;
LAZAREVIC, 2014). A dupla mutação frequentemente relatada na região BCP, A1762T
e G1764A, reduz a síntese do RNAm Pré-C, resultando na diminuição da expressão do
14
HBeAg e tem sido relacionada ao desenvolvimento de CHC (GAO; DUAN; COFFIN,
2015; LAZAREVIC, 2014).
Mutações na região P
O domínio da transcriptase reversa, localizado na região da polimerase do
HBV, representa um alvo para a terapia antiviral utilizando análogos núcleos(t)ídeos.
Mutações primárias nessa região estão frequentemente relacionadas à resistência aos
antivirais lamivudina (LAM), telbivudina (LdT), adefovir (ADF), entecavir (ETV) e
tenofovir (TDF), enquanto que as mutações secundárias/compensatórias são responsáveis
por melhorar a eficiência da replicação viral (Quadro 1) (LAZAREVIC, 2014; LOK et
al., 2007; WARNER; LOCARNINI, 2014). A mutação mais comumente descrita ocorre
no motivo YMDD (tirosina-metionina-aspartato-aspartato) da RT, com a substituição de
um resíduo de metionina (M) por uma valina (V) ou isoleucina (I) na posição 204
(M204V/I) (LOK et al., 2007; TAN et al., 2015). Frequentemente essas alterações são
selecionadas durante a terapia com LAM. No entanto, mutações de resistência aos
antivirais já foram identificadas em indivíduos virgens de tratamento, o que sugere que
tais alterações podem ocorrer naturalmente, ou devido a transmissão do vírus mutante a
partir de um paciente tratado (DEVI; LOCARNINI, 2013; GOMES-GOUVÊA et al.,
2015; MIRANDOLA et al., 2011).
Mutações na região X
Mutações no gene X têm sido relacionadas à hepatocarcinogênese (Quadro
1). Estudos mostram que a extremidade 3’ da proteína HBx está frequentemente
suprimida em células de carcinoma hepatocelular, o que leva à deleção de 30 a 40
aminoácidos na região carboxiterminal. Essa alteração na proteína HBx pode
desempenhar um papel importante no desenvolvimento de CHC, pela promoção do
estresse oxidativo e indução de dano do DNA mitocondrial (JUNG; KIM, 2013;
LAZAREVIC, 2014; LIU et al., 2014; MA et al., 2008; OZKAL-BAYDIN, 2014;
ZHANG et al., 2015).
15
Quadro 1 - Mutações no genoma do HBV e suas implicações clínicas (modificado)
Região
Mutação
Implicação clínica
T116N, P120S/E, I/T126A/N/I/S, Q129H/R,
T131N/I, M133L, K141E, P142S, D144A/E,
Escape vacinal
G145R/A.
Y100S, Q101R, P105R, T115N, T116N,
G119R, P120L, R122P, T123N, C124R/Y,
Pré-S/S
T126I/S, P127H/L, Q129P/R, T131N/I,
M133T, Y134C, S136P, C139R, T140I,
Infecção oculta pelo HBV
K141E, S143L, D144A, G145R/A, S167L,
R169H, S174N, L175S, V177A,
Q181STOP.
T1753C, A1762T, G1764A, C1766T,
HBeAg negativo
T1768A, G1896A, G1899A.
Pré-C/C
C1653T, T1753C, A1762T, G1764A,
CHC
G1896A, G1899A.
A1762T, G1764A, G1862T, G1896A.
Hepatite fulminante
rtL80V/I, rtI169T, rtV173L, rtL180M,
rtA181T/V, rtT184S/G, rtS202I, rtM204V/I,
Resistência a LAM/ LdT
rtQ215S.
rtA181T/V, rtI233V, rtN236T.
Resistência ao ADF
P
rtL180M, rtT184G/S, rtS202I/G, rtM204V,
Resistência ao ETV
rtM250V.
rtP177G, rtA194T, rtF249A.
Resistência a TDF
X
Deleções na extremidade 3’-HBx.
CHC
Legenda: HBV: vírus da hepatite B; CHC: carcinoma hepatocelular; LAM: lamivudina;
LdT: telbivudina; ADF: adefovir; ETV: entecavir; TDF: tenofovir.
Fonte: Lazarevic (2014)
1.5 Aspectos clínicos da hepatite B
O curso natural da infecção pelo vírus da hepatite B é determinado pela
interação entre o vírus e a resposta imune do hospedeiro. Após a exposição ao HBV, a
maioria (cerca de 95%) dos indivíduos adultos desenvolve a infecção aguda seguida pela
eliminação completa do vírus e imunidade ao longo da vida. Por outro lado, em
aproximadamente 5-10% dos casos, há persistência do vírus no organismo, sendo o
HBsAg detectável por mais de seis meses, o que caracteriza a hepatite B crônica. Em
casos raros (0,1 a 0,5%), ocorre uma resposta imune exacerbada, ocasionando hepatite
fulminante (ELGOUHARI; TAMIMI; CAREY, 2008; JINDAL; KUMAR; SARIN,
2013).
16
A hepatite B aguda inclui o período de incubação, fase prodrômica, ictérica e
de convalescência. O período médio de incubação do vírus é de 75 dias, podendo variar
de um a seis meses. A fase prodrômica caracteriza-se por sintomas inespecíficos, tais
como: mal-estar, falta de apetite, náuseas, vômitos e dores abdominais, com uma duração
de um a cinco dias. Na fase ictérica, há um aumento dos níveis séricos de bilirrubina e
transaminases, indicando lesão hepatocelular. Essa fase dura normalmente de duas a três
semanas, sendo caracterizada pelo aparecimento de icterícia, leve hepatomegalia, colúria
e hipocolia fecal. A ocorrência desses sintomas depende da idade no momento da
infecção, sendo bebês e crianças em sua maioria assintomática, enquanto que cerca de
30% dos adultos apresentam icterícia. A fase final da infecção aguda é a convalescência,
que está associada à eliminação do vírus, normalização dos níveis de transaminases,
resolução dos sintomas e surgimento do marcador anti-HBs, o qual confere imunidade ao
longo da vida (JINDAL; KUMAR; SARIN, 2013; LIANG, 2009; SHIFFMAN, 2010;
TRÉPO; CHAN; LOK, 2014).
A progressão para cronicidade está intimamente relacionada à idade do
indivíduo no momento da infecção. A infecção persiste em cerca de 90% dos recémnascidos e em aproximadamente 20% das crianças infectadas entre um e cinco anos de
idade. A partir de cinco anos, o risco de desenvolver infecção crônica é menor que 10%
(ASPINALL et al., 2011; CROAGH; LUBEL, 2014; LIAW; CHU, 2009; LOCARNINI
et al., 2015).
A infecção crônica pelo HBV está associada a uma variedade de
manifestações clínicas resultantes da interação entre o vírus, hepatócitos e resposta imune
do hospedeiro. Sendo assim, o espectro dessa infecção pode variar desde um estado de
portador assintomático a cirrose e/ou CHC (EASL, 2012; LOCARNINI et al., 2015; SHI;
SHI, 2009). O curso natural da doença consiste em cinco fases distintas: imunotolerância,
imunoreativa, de portador inativo, reativação e infecção oculta pelo HBV (ou HBsAg
negativa). No entanto, nem todos pacientes passam por todas as fases, e a duração de cada
uma pode ser variável (EASL, 2012).
A fase de imunotolerância é caracterizada pela positividade ao HBeAg, alta
carga viral (níveis de HBV DNA no soro geralmente superiores a 2 x 106 UI/mL) e níveis
normais de alanina aminotransferase (ALT). Nessa fase a replicação viral é tolerada pelo
sistema imunológico do hospedeiro, havendo discreta inflamação com baixa produção de
interleucina (IL) 10, citocinas pró-inflamatórias: IL-6, IL-8 e fator de necrose tumoral
(TNF) alfa. Nesse estágio, a infecciosidade é elevada, porém não há dano hepático
17
significativo. A sua duração é extremamente variável, sendo mais longa em pacientes
infectados pelo HBV no período perinatal (CROAGH; LUBEL, 2014; EASL, 2012;
GISH et al., 2015; LOCARNINI et al., 2015).
A fase imunorreativa está associada à presença do marcador HBeAg,
diminuição da carga viral, aumento nos níveis de transaminases e doença hepática ativa.
Nesse período, a resposta imunológica contra o vírus pode levar à danos hepáticos,
aumentando, assim, o risco de evolução para cirrose e carcinoma hepatocelular
(CROAGH; LUBEL, 2014; EASL, 2012; KUO; GISH, 2012; TRÉPO; CHAN; LOK,
2014).
O estágio de portador inativo do HBV ocorre após a soroconversão do HBeAg
para o anti-HBe, com níveis de HBV DNA baixos ou indetectáveis no soro e
normalização nos níveis de transaminases. Com o resultado do controle imunológico da
infecção, esse estado confere um prognóstico favorável a longo prazo, com um risco baixo
de desenvolvimento de cirrose ou CHC. No entanto, os pacientes nessa fase devem ser
seguidos com testes periódicos uma vez que pode haver reativação espontânea da hepatite
B (CROAGH; LUBEL, 2014; EASL, 2012; GISH et al., 2015).
A reativação ocorre em alguns pacientes infectados após a fase de portador
inativo. É caracterizada pela flutuação dos níveis de HBV DNA e aminotransferases. Os
pacientes são HBeAg negativos e podem estar infectados por vírus com mutações nas
regiões pré-C ou BCP, as quais diminuem a expressão do antígeno “e”. Acredita-se que
a soroconversão do HBeAg para anti-HBe indica diminuição da replicação do HBV e
remissão da doença hepática. No entanto, a ocorrência de mutantes HBeAg negativos
durante a infecção crônica pelo HBV, especialmente na presença de uma carga viral alta,
está associada com exacerbação da lesão hepática e um pior prognóstico (EASL, 2012;
LOCARNINI et al., 2015; PURI, 2013; SHI; SHI, 2009).
A fase HBsAg negativa, conhecida como infecção oculta pelo HBV, é
caracterizada pela presença do HBV DNA no fígado e/ou soro de indivíduos HBsAg
negativos. Diferentes mecanismos podem ser responsáveis pela ausência do HBsAg.
Dentre eles, se destacam a resposta imune do hospedeiro com a formação de
imunocomplexos HBsAg e anti-HBs reduzindo a circulação do antígeno livre, a
integração do genoma viral ao do hospedeiro, a coinfecção com outros agentes
infecciosos, como HCV e HIV, além do consumo crônico de etanol. Quanto aos fatores
virais, mutações na região Pré-S/S do genoma do HBV estão relacionadas à alteração na
antigenicidade ou expressão do HBsAg (FUENTE et al., 2011; RAIMONDO et al. 2013;
18
ROMERO et al., 2011; SAMAL; KANDPAL; VIVEKANANDAN, 2012). As principais
implicações clínicas da infecção oculta pelo HBV incluem a reativação da doença em
pacientes imunossuprimidos, progressão para doença hepática e desenvolvimento de
CHC, além do risco potencial de transmissão do HBV por transfusão sanguínea,
transplante de órgãos, hemodiálise e por via vertical (FUENTE et al., 2011; HOFFMANN
et al., 2014; KWAK; KIM, 2014; POLLICINTO; RAIMONDO, 2014; PONDÉ, 2015;
SQUADRITO; SPINELLA; RAIMONDO, 2014).
1.6 Patogenia da infecção pelo HBV
O vírus da hepatite B pode replicar dentro dos hepatócitos sem causar dano
celular direto. A resposta imune do hospedeiro é responsável pelo controle da infecção
viral, bem como pelos mecanismos de lesão das células hepáticas, podendo progredir para
cirrose e CHC (FERRARI, 2015; GISH et al., 2015; TAN; KOH; BERTOLETTI, 2015).
A eliminação do HBV envolve a participação de células das respostas imunes
inata e adaptativa. A limitação da propagação inicial do vírus se dá por mecanismos não
citolíticos, incluindo a produção de citocinas antivirais, tais como interferon do tipo I
(IFN-α/β) e TNF, em conjunto com a ativação de células natural killers (NK), natural
killers T (NKT) e dendríticas. Após o declínio da carga viral, segue uma resposta imune
citolítica com apoptose dos hepatócitos e necrose, o que coincide com o aumento das
transaminases no soro. A apresentação dos hepatócitos infectados é realizada via antígeno
leucocitário humano classe I (HLA-I) para os linfócitos T citotóxicos CD8+. Após o
reconhecimento, essas células atuam eliminando os hepatócitos infectados e iniciam uma
cascata de eventos imunológicos levando a proliferação de linfócitos e a inflamação
(BAUMERT; THIMME; VON WEIZSÄCKER, 2007; FERRARI, 2015; LIAW; CHU,
2009; TAN; KOH; BERTOLETTI, 2015).
A recuperação total com eliminação do vírus está associada a resposta
multiespecífica dos linfócitos CD4+ e CD8+. Indivíduos com infecção aguda autolimitada
apresentam resposta específica mais vigorosa quando comparados aos pacientes que se
tornam cronicamente infectadas. Portanto, quando a resposta imune celular é deficiente,
o HBV pode replicar em níveis elevados na ausência de anormalidades citológicas ou
inflamação hepática, o que sustenta a hipótese de que a lise de células do fígado ocorre,
principalmente, por linfócitos CD8+, os quais são considerados os principais responsáveis
pela depuração viral em virtude da sua capacidade de destruir os hepatócitos infectados
19
(GUIDOTTI; ISOGAWA; CHISARI, 2015; RAPICETTA; FERRARI; LEVRERO,
2002; SAID; ABDELWAHAB, 2015).
1.7 Diagnóstico laboratorial da infecção pelo HBV
O diagnóstico laboratorial da infecção pelo HBV é realizado pela detecção de
marcadores sorológicos incluindo antígenos virais (HBsAg e HBeAg) e anticorpos (antiHBs, anti-HBe e anti-HBc - fração IgM e Total), que podem ser detectados no soro por
ensaios imunoenzimáticos (ELISA - Enzyme Linked Immuno Sorbent Assay). Testes
bioquímicos tais como: dosagem das transaminases, bilirrubina, valores de albumina e
tempo de protrombina também são utilizados para avaliar o prognóstico da hepatite B,
uma vez que são essenciais para medir o grau de lesão hepática e determinar a gravidade
da doença (LIAW; CHU, 2009; TRÉPO; CHAN; LOK, 2014; WHO, 2015a).
Adicionalmente, técnicas moleculares para detecção do HBV DNA são
importantes para avaliar o nível de replicação, progressão da doença, necessidade de
terapia antiviral, bem como o monitoramento do tratamento. Assim, testes qualitativos e
quantitativos, como a reação em cadeia pela polimerase (PCR) e a PCR em tempo real,
respectivamente, têm sido cada vez mais empregados no diagnóstico da infecção pelo
HBV
por
apresentarem
alta
sensibilidade
e
especificidade
(CHEVALIEZ;
PAWLOTSKY, 2009; DATTA; CHATTERJEE; VEER, 2014; DÉNY; ZOULIM, 2010;
LIANG, 2009).
O primeiro marcador sorológico encontrado na infecção pelo HBV é o
HBsAg, indicando infecção presente. Surge no soro durante a fase de incubação, cerca de
duas a seis semanas antes do início dos sintomas. Na hepatite B aguda, ele declina a níveis
indetectáveis em até seis meses (Figura 7). Testes moleculares altamente sensíveis podem
detectar o HBV DNA no soro cerca de 10 a 20 dias antes do aparecimento do HBsAg. O
HBeAg, também presente no início da infecção, está relacionado com altos níveis de
replicação do HBV e, geralmente, com a elevação das transaminases e início das
manifestações clínicas. Sua positividade indica alta infecciosidade (BRASIL, 2008;
LIANG, 2009; SHIFFMAN, 2010; TRÉPO; CHAN; LOK, 2014; WHO, 2015a).
Anticorpos contra o antígeno do core (anti-HBc) normalmente aparecem um
pouco antes do início dos sintomas. Inicialmente, surgem os anticorpos da classe IgM,
que permanecem detectáveis por aproximadamente seis meses após a exposição. Embora
o anti-HBc IgM possa estar presente em alguns pacientes com exacerbações graves da
20
infecção crônica pelo HBV, os títulos do anticorpo nesses casos são menores do que na
infecção aguda. Após o declínio do marcador anti-HBc IgM, surge o anti-HBc IgG, o
qual é detectável ao longo da vida (como marcador anti-HBc total), indicando exposição
ao vírus (LIANG, 2009; TRÉPO; CHAN; LOK, 2014).
Após o declínio do HBeAg, surge o seu anticorpo correspondente (anti-HBe),
o qual é um marcador sorológico de prognóstico favorável durante a hepatite B aguda,
indicando início da recuperação. O marcador anti-HBs surge mais tardiamente durante a
infecção, sendo detectado semanas após o desaparecimento do HBsAg. Sua presença está
associada à imunidade contra o HBV. Pacientes com a resolução completa da infecção
apresentam positividade para os marcadores anti-HBs e anti-HBc total. No entanto,
alguns que se recuperam da hepatite B não apresentam anti-HBs detectável, pois esse
marcador pode declinar a níveis indetectáveis com o passar dos anos. Por esta razão, o
marcador anti-HBc total é mais confiável na avaliação da infecção prévia pelo HBV,
enquanto que o anti-HBs é utilizado para avaliar a imunidade e a resposta vacinal contra
hepatite B (LIANG, 2009; SHIFFMAN, 2010; TRÉPO; CHAN; LOK, 2014).
A persistência do HBsAg por mais de seis meses indica progressão para
infecção crônica. O curso típico da hepatite B crônica está demonstrado na Figura 8. Esses
pacientes apresentam replicação viral persistente e os marcadores HBsAg, HBeAg e HBV
DNA continuam sendo detectados no soro (muitas vezes em títulos elevados) (CROAGH;
LUBEL, 2014; GISH et al., 2015; LIAW; CHU, 2009).
Alguns indivíduos com infecção crônica pelo HBV podem apresentar perfil
sorológico atípico, caracterizado pela persistência do HBV DNA na ausência do HBsAg.
Essa forma peculiar da hepatite B crônica, denominada infecção oculta pelo HBV, pode
ser caracterizada graças ao desenvolvimento de técnicas de biologia molecular altamente
sensíveis, permitindo a detecção de baixos níveis de HBV DNA. Nesses pacientes, o
DNA pode ser detectado na presença do anti-HBc e/ou anti-HBs, ou até mesmo na
ausência de ambos marcadores sorológicos (KWAK; KIM, 2014; PONDÉ, 2015;
RAIMONDO et al., 2013; ROMERO et al., 2011).
Embora não faça parte da rotina de diagnóstico da hepatite B, estudos
apontam a relevância da genotipagem do HBV para escolha do tratamento antiviral, uma
vez que a resposta à terapia difere dentre indivíduos infectados por diferentes genótipos.
Além disso, a genotipagem é importante para monitorar a progressão da doença hepática,
visto que manifestações clínicas distintas foram associadas a diferentes genótipos. O
sequenciamento de nucleotídeos do DNA viral é a técnica padrão-ouro para genotipagem,
21
permitindo, inclusive, a identificação de genótipos recombinantes e mutações no genoma
(DATTA; CHATTERJEE; VEER, 2014; VILLAR et al., 2015; YANO; AZUMA;
HAYASHI, 2015).
Figura 7 - Curso típico da hepatite B aguda (modificada)
Fonte: CDC (2015b)
Figura 8 - Curso típico da infecção crônica pelo HBV (modificada)
Fonte: CDC (2015b)
22
1.8 Tratamento da hepatite B
A terapia antiviral para a infecção crônica pelo HBV visa suprimir a
replicação viral e, consequentemente, reduzir o risco de progressão para cirrose,
descompensação hepática e desenvolvimento de CHC. O resultado ideal desejado após o
tratamento é a negativação sustentada do HBsAg, associada a soroconversão para antiHBs, porém esse desfecho é raramente alcançado devido à persistência de cccDNA no
núcleo dos hepatócitos infectados. Nessas condições, a resposta ao tratamento é avaliada
de acordo com a diminuição dos níveis de HBV DNA no soro, ausência dos marcadores
HBeAg (soroconversão para seu respectivo anticorpo) e HBsAg, normalização dos níveis
séricos de ALT e resposta histológica com redução da atividade inflamatória hepática
(GISH et al., 2015; HALEGOUA-DE MARZIO; HANN, 2014; KUO; GISH, 2012;
WHO, 2015b; YOU et al., 2014)
De acordo com a Organização Mundial de Saúde (OMS), o tratamento é
recomendado para adultos, adolescentes e crianças com hepatite B crônica que
apresentam evidência clínica de cirrose, independente dos níveis de alanina
aminotransferase (ALT), HBeAg e HBV DNA. Também é indicado nos casos de adultos
com hepatite B crônica, com idade superior a 30 anos, mesmo que sem evidência de
cirrose, mas que apresentam níveis de ALT elevados e HBV DNA superior a 20.000
UI/mL, independente da positividade para o marcador HBeAg. Nos demais pacientes com
infecção crônica pelo HBV, deve-se fazer o monitoramento contínuo para avaliar o
estágio da doença hepática e a elegibilidade para o tratamento (WHO, 2015b). Pacientes
com hepatite B aguda normalmente não necessitam de tratamento antiviral, o uso da
terapia é indicado apenas nos casos da doença grave, com sinais de insuficiência hepática
significativa. Para os que desenvolvem hepatite B fulminante, o uso de antiviral é
recomendado para reduzir o risco de reinfecção após o transplante hepático (LIAW; CHU,
2009; RAJBHANDARI; CHUNG, 2016; TILLMANN; PATEL, 2014).
As opções de agentes aprovados pelo FDA (Food and Drug Administration)
para o tratamento da hepatite B crônica incluem os imunomoduladores interferon-alfa
(IFN-) convencional e interferons-alfa peguilados (PEG-IFN-) 2a e 2b, os análogos
nucleosídeos lamivudina, telbivudina e entecavir, além dos análogos nucleotídeos
adefovir e tenofovir (FDA, 2015; WHO, 2015b).
No Brasil, o Ministério da Saúde, por meio do Protocolo Clínico e Diretrizes
Terapêuticas para Hepatite B e Coinfecções, estabelece os critérios nacionais para início
23
do tratamento de portadores crônicos do HBV. Assim, a terapia é indicada para pacientes
HBeAg reagentes e com nível de ALT superior a duas vezes o limite normal; adultos
maiores de 30 anos HBeAg positivos; paciente HBeAg não reagentes, que apresentam
HBV DNA superior a 2.000 UI/mL e nível de ALT maior que duas vezes o limite da
normalidade. Além desses, outros critérios de indicação de tratamento e recomendações
terapêuticas são descritos no manual, conforme cada situação clínica e laboratorial.
Visando a efetividade do tratamento, o Sistema Único de Saúde (SUS) disponibiliza
gratuitamente os seguintes fármacos para o tratamento da infecção crônica pelo HBV:
PEG-IFN- (2a e 2b), entecavir e tenofovir (BRASIL, 2016).
A resposta terapêutica difere em relação aos genótipos do HBV. A resposta
sustentada com soroconversão do HBeAg e normalização dos níveis de ALT, após o
tratamento com IFN- ou PEG-IFN-, é consideravelmente melhor nos indivíduos
infectados com os genótipos A e B quando comparados aos portadores do genótipos C e
D. Em relação à terapia utilizando antivirais análogos nucleos(t)ídeos, o genótipo B está
associado a uma melhor resposta ao tratamento com lamivudina do que genótipo C, e
ambos apresentam um risco semelhante de desenvolvimento de resistência. Por outro
lado, indivíduos infectados pelo genótipo A tendem a apresentar mutações de resistência
à lamivudina mais precocemente em relação aqueles portadores do genótipo D
(KRAMVIS; KEW, 2005; POURKARIM et al., 2014; SHI, 2012; RAJBHANDARI;
CHUNG, 2016; YANO; AZUMA; HAYASHI, 2015).
1.9 Epidemiologia da infecção pelo HBV
1.9.1 Transmissão
O HBsAg e HBV DNA podem ser detectados em diversos fluidos corporais
(sangue, sêmen, secreção vaginal e menstrual, saliva, lágrima, secreção nasofaríngea,
leite materno, urina e fezes), tornando-os potenciais fontes de infecção pelo HBV
(BURNS; THOMPSON, 2014; ELGOUHARI; TAMIMI; CAREY, 2008; GORGOS,
2013; HOU; LIU; GU, 2005; LAVANCHY, 2004; SCOTT et al., 1980). O sangue é o
veículo mais importante para a transmissão viral, seguido dos fluidos seminal, vaginal e
menstrual, dentre outros. Dessa forma, as principais vias de transmissão do vírus incluem
a vertical, sexual e parenteral/percutânea (GORGOS, 2013; LAVANCHY, 2004; WHO,
2015a). O risco de transmissão está diretamente relacionado ao nível do HBV DNA no
24
soro, e esse normalmente é maior em pacientes HBeAg positivos. Porém, os isolados
virais que apresentam mutações que impedem a expressão do HBeAg também têm sido
associados à transmissão (ALTER, 2003; SHIFFMAN, 2010; TIIT, 1997). Além disso, o
HBV pode permanecer infeccioso por mais de uma semana em superfícies a temperatura
ambiente (BOND et al., 1981).
A transmissão vertical do HBV, da mãe infectada para o filho, pode ocorrer
por via transplacentária, ou no momento do parto. Em áreas de alta endemicidade para
hepatite B, a transmissão do vírus ocorre principalmente nos primeiros anos de vida,
resultante da transmissão vertical, ou ainda da horizontal intrafamiliar, a qual está
associada ao compartilhamento de objetos pessoais e/ou contato com lesões de pele e
mucosas de familiares infectados (BURNS; THOMPSON, 2014; KWON; LEE, 2011; LI;
HOU; CAO, 2015; ORDÖG et al., 2003; WHO, 2015a).
A hepatite B é considerada uma infecção sexualmente transmissível. A
transmissão sexual é a principal via de disseminação do HBV entre adolescentes e adultos
em países de baixa e média endemicidade. Essa infecção ocorre sobretudo entre HSH e
heterossexuais com múltiplos parceiros sexuais, principalmente dentre aqueles que são
profissionais do sexo e seus clientes. Em geral, os principais fatores de risco associados
à infecção pelo HBV incluem: múltiplos parceiros sexuais, duração (anos) de atividade
sexual, sexo desprotegido e histórico de IST (ALTER et al., 1986; GORGOS, 2013;
HOU; LIU; GU, 2005; LAVANCHY, 2004; TRÉPO; CHAN; LOK, 2014; WHO, 2015a).
Além da presença do vírus em diversos fluidos corporais, o HBsAg foi detectado na
superfície das mucosas lesionadas do reto e ânus de indivíduos infectados, corroborando
as práticas de sexo anal e oro-anal como potenciais fontes de transmissão do HBV
(GORGOS, 2013; REINER et al., 1982; SCHREEDER et al., 1982).
A transmissão parenteral ou percutânea envolve a exposição a sangue e
fluidos corporais contaminados pelo HBV. Práticas e comportamentos relacionados a
essa forma de transmissão incluem o uso de drogas injetáveis, acupuntura, tatuagem,
compartilhamento de lâminas de barbear e outros objetos perfurocortantes, uso de
materiais médico/odontológicos esterilizados inadequadamente, transfusão de sangue,
diálise, transplante de órgãos e exposição ocupacional de profissionais da saúde. Embora
a triagem de hemoderivados tenha reduzido a transmissão associada a transfusão
sanguínea, essa forma de infecção ainda ocorre em alguns países em desenvolvimento
(HOU; LIU; GU, 2005; LOCARNINI et al., 2015; TRÉPO; CHAN; LOK, 2014).
25
1.9.2 Distribuição da infecção pelo HBV
A infecção pelo vírus da hepatite B apresenta uma ampla distribuição global.
Segundo a OMS, no mundo há mais de 240 milhões de pessoas cronicamente infectadas.
Além disso, estimativas sugerem que aproximadamente 780 mil pessoas morrem a cada
ano por complicações relacionadas ao HBV, cerca de 650 mil devido à infecção crônica
e 130 mil pela forma aguda da doença (LOZANO et al., 2012; WHO, 2015a).
A distribuição da infecção pelo HBV é classificada de acordo com a
prevalência para o marcador HBsAg e varia com a área geográfica, idade e o grupo
populacional. Assim, regiões de endemicidade alta são aquelas em que mais de 8% da
população é HBsAg positiva, com taxa elevada de infecção durante a infância e, em geral,
são regiões em desenvolvimento como países da África subsaariana e parte da Ásia.
Regiões com endemicidade intermediária são aquelas em que os índices de positividade
para o HBsAg variam entre 2 e 7%, sendo que alguns autores ainda reclassificam essas
áreas em intermediária baixa (2 a 4%) e alta (5 a 7%). Países situados no leste e sul da
Europa, parte das Américas do Sul e Central, Oriente Médio e África são considerados
com prevalência intermediária. Nessas regiões, os padrões de transmissão do HBV são
mistos, ocorrendo na infância, adolescência e fase adulta. Áreas de endemicidade baixa
são aquelas em que menos de 2% da população apresenta hepatite B crônica. Esse perfil
é encontrado na Europa Ocidental, Austrália, Japão e parte das Américas, sendo que a
maioria das infecções ocorre em adolescentes e adultos pelas vias sexual e parenteral
(LOCARNINI et al., 2015; MACLACHLAN; COWIE, 2015; OTT et al., 2012; TRÉPO;
CHAN; LOK, 2014).
Schweitzer et al. (2015) publicaram uma revisão sistemática da literatura com
dados sobre a prevalência da infecção crônica pelo HBV no mundo. Foram incluídos
estudos que relataram o HBsAg como marcador sorológico de infecção crônica pelo
HBV, excluindo os grupos de alto risco. Em nível global, estimou-se uma prevalência de
3,61% para o HBsAg, sendo que variou de 0,1%, na Noruega e Reino Unido, a maior que
20% em países como o Sudão do Sul e Kiribati. O número maior de pessoas com hepatite
B crônica foi encontrado nas regiões do Pacífico Ocidental e África. Já o continente
americano apresentou o menor número de indivíduos infectados. O estudo ainda sugere
uma diminuição da prevalência do HBV em países do Sudeste Asiático, Pacífico
Ocidental e nas regiões do Mediterrâneo Oriental entre os períodos de 1957-1989 e 19902013. Em contrapartida, foi observada uma tendência de aumento na prevalência em
26
alguns países africanos e da Europa Oriental nesses intervalos de tempo. A Figura 9 ilustra
a endemicidade do HBV no mundo, de acordo com a prevalência do HBsAg.
Figura 9 - Prevalência do HBsAg no mundo (modificada)
Fonte: Schweitzer et al. (2015)
No Brasil, segundo o inquérito de base populacional das infecções pelos vírus
das hepatites A, B e C, realizado entre os anos de 2005 e 2009, nas 26 capitais e no Distrito
Federal, a prevalência global para o marcador de exposição ao HBV (anti-HBc) foi de
7,4% (IC 95%: 6,8-8,0). A prevalência para o HBsAg foi de 0,37% (IC 95%: 0,25-0,50),
classificando o conjunto das capitais brasileiras como de endemicidade baixa (BRASIL,
2010a; 2012).
Na Região Centro-Oeste, exceto Brasília, a prevalência global encontrada
para o HBV na população em geral foi de 5,3% (IC 95%: 4,6-6,1) (PEREIRA et al., 2009).
No estado de Goiás, investigações realizadas em diferentes grupos populacionais (Quadro
2) estimaram taxas de prevalência global variando de 5,6% em gestantes (FERNANDES
C. N. et al., 2014) a 63,4% em pacientes em diálise (BORGES et al., 1997). A prevalência
para o HBsAg variou de 0% em pacientes com doenças falciformes, anestesiologistas,
dentistas e portadores de diabetes mellitus tipo 2 (BASTOS, 2000; CARNEIRO;
DAHER, 2003; DE PAIVA et al., 2008; MARQUES, 2015) a 14,5% em indivíduos com
suspeita clínica de hepatite (SILVA et al., 2002).
27
Quadro 2 - Prevalência da infecção pelo HBV em diferentes grupos populacionais no
estado de Goiás
Referência
Cardoso et al. (1990)
Martelli et al. (1990)
Rosa et al. (1992)
Azevedo et al. (1994)
Porto et al. (1994)
Cardoso et al. (1996)
Borges et al. (1997)
Teles et al. (1998)
Bastos (2000)
Lopes et al. (2001)
Silva et al. (2002)
Teles et al. (2002)
Carneiro e Daher (2003)
Costa (2004)
De Souza et al. (2004)
Tavares et al. (2004)
Silva et al. (2005)
Ferreira et al. (2006)
Oliveira et al. (2006)
De Paiva et al. (2008)
Matos et al. (2008)
Ferreira (2008)
Matos et al. (2009)
Dos Anjos et al. (2011)
Aires et al. (2012)
Barros et al. (2013)
Caetano (2014)
Marinho et al. (2014)
Fernandes C. N. et al.
(2014)
Matos (2014)
Silva (2014)
Brandão et al. (2015)
Marques (2015)
Moraes et al. (2015)
Oliveira et al. (2016a)
Carvalho (2016)
População
N
Feminina de área urbana
Prisioneiros;
Primodoadores
Pacientes com hanseníase em
tratamento ambulatorial;
institucionalizados
Profissionais da área da saúde
Meninos de/na rua
Gestantes/parturientes
Pacientes em diálise
Pacientes em hemodiálise
Pacientes com doenças falciformes
Profissionais de hemodiálise
Indivíduos com suspeita clínica de
hepatite
Pacientes em hemodiálise
(1995; 1999)
Anestesiologistas
Idosos residentes em asilos
Portadores de doença mental
Hemofílicos
Profissionais de laboratório
Pacientes em hemodiálise
Adolescentes de baixa renda
Dentistas
Caminhoneiros que trafegam pela
BR-153
UDNI;
UDI
Comunidade de afrodescendentes
Primodoadores de sangue
Pacientes com tuberculose
Reeducandas
Assentados rurais
Catadores de materiais recicláveis
475
201;
1033
Prevalência
(%)
HBsAg Global*
6,1
26,4;
12,8
83;
171
4,8;
8,8
16,9;
50,5
625
496
1459
175
282
63
152
2,3
2
0,5
13,7
12
0
0,7
23,4
13,5
7,5
63,4
56,7
12,7
24,3
1396
14,5
50,7
282;
536
90
195
433
102
648
664
680
12,0;
5,8
0
0,5
1,6
1,1
0,7
2,4
0,6
0
8,9
32,3
22,4
43,7
24,1
5,9
6,0
641
2,5
18,9
852;
150
878
984
402
148
467
431
0,2;
0,6
1,8
0,3
3,2
0,7
0,8
0,7
13,5;
20,9
35,4
6,9
25,6
18,9
10,9
12,8
Gestantes
1.303
0,6
5,6
Mulheres profissionais do sexo
Usuários de crack institucionalizados
Pacientes infectados pelo HIV
Pacientes com diabetes mellitus tipo 2
Pacientes com doença mental
institucionalizados
Pacientes infectados pelo HIV, virgens
de tratamento
População em situação de rua abrigada
402
600
495
605
0,7
0,5
3,8
0
17,1
7,0
33,5
17,8
333
0,9
12,9
505
4,9
25,1
353
0,5
21,8
-
*Presença de qualquer marcador de infecção pelo HBV. UNDI: usuários de drogas não injetáveis, UDI:
usuários de drogas injetáveis, HIV: vírus da imunodeficiência humana.
28
1.9.3 Distribuição dos genótipos e subgenótipos
A distribuição geográfica dos genótipos e subgenótipos do HBV é variável
nas diferentes regiões do mundo. O genótipo A encontra-se amplamente distribuído,
sendo que o subgenótipo A1 é frequentemente detectado na África subsaariana, Ásia e
em regiões com história de comércio de escravos, como a América do Sul. O subgenótipo
A2 é prevalente principalmente no norte da Europa, A3 na África central e ocidental,
enquanto A4, A5, A6 e A7 circulam em outras regiões da África. Os genótipos B e C são
comumente identificados na Ásia. O subgenótipo B1 é mais encontrado no Japão, B2-B5
no leste asiático, B6 em populações indígenas do Ártico e B7-B9 na Indonésia. Os
subgenótipos C1-C16 apresentam maior circulação nas regiões leste e sudeste da Ásia. O
genótipo D é cosmopolita, sendo dominante na região mediterrânea, norte e leste da
Europa e norte da África. O subgenótipo D1 é frequente na Grécia, Turquia e norte da
África, D2 no leste Europeu, D3 na Itália, Sérvia, África do Sul e Alasca e D4 na Oceania
e Somália, enquanto que D5-D9 foram detectados na Índia, Indonésia, Nigéria e Tunísia.
A presença do genótipo E foi evidenciada principalmente na África central e ocidental. O
genótipo F, com os quatro subgenótipos (F1-F4) e diferentes clados (F1a, F1b, F2a, F2b),
está distribuído predominantemente nas Américas Central e do Sul. O genótipo G circula
em países da Europa e nos Estados Unidos da América. O genótipo H tem sido descrito
no México, América Central, Estados Unidos e Japão. Recentemente, o genótipo I (I1-I2)
foi identificado no Vietnã e Laos, e o genótipo J isolado em um único indivíduo no Japão
(ALVARADO-MORA; PINHO, 2013; KRAMVIS, 2014; LIN; KAO, 2011;
POURKARIM et al., 2014; SUNBUL, 2014; ZEHENDER et al., 2014).
No Brasil, embora já tenha sido relatada a presença de distintos genótipos do
HBV (A, B, C, D, E, F, G e H), reflexo da mistura étnica do País e constante
movimentação populacional devido a globalização, os genótipos A, D e F são os mais
prevalentes, havendo maior proporção do subgenótipo A1 (ARAUJO et al., 2004;
ARAUJO et al., 2014; ASSIS et al., 2015; BERTOLINI et al., 2012; DIAS et al., 2012;
MARINHO et al., 2014; MELLO et al., 2007; MOTTA-CASTRO et al., 2008; NABUCO
et al., 2012; PEREIRA et al., 2009).
29
1.10 Prevenção e controle da infecção pelo HBV
Estratégias para reduzir a propagação da infecção pelo HBV incluem a
imunização dos indivíduos susceptíveis, rastreamento sorológico, tratamento dos
portadores crônicos, além de mudanças comportamentais e condutas que evitem a
exposição ao sangue e outros fluidos corporais, tais como: uso de preservativo durante as
relações sexuais, triagem sorológica nos bancos de sangue/órgão/sêmen, rastreamento de
gestantes para o HBV, não compartilhamento de agulhas e objetos pessoais
perfurocortantes, inativação dos hemoderivados, política de redução de danos, práticas
adequadas de biossegurança em estabelecimentos de saúde e profilaxia pós-exposição.
Dentre as estratégias de prevenção contra o HBV, a vacinação é a forma mais segura,
eficaz e com melhor custo-benefício (FRANCO et al., 2012; LOCARNINI et al., 2015;
MEIRELES; MARINHO; VAN DAMME, 2015; WHO, 2012; 2015a).
A vacina contra hepatite B foi disponibilizada comercialmente a partir do ano
de 1982, sendo a primeira derivada de plasma de portadores do HBV. Posteriormente, a
mesma foi substituída pela chamada vacina de segunda geração, desenvolvida pela
técnica do DNA recombinante expressando o HBsAg em leveduras. Já a vacina de
terceira geração, também recombinante, apresenta epítopos neutralizantes das regiões
Pré-S/S do HBV. Em ensaios controlados, essa vacina tem demonstrado ser mais
imunogênica quando comparada a de segunda geração, porém ainda não está amplamente
distribuída (FRANCO et al., 2012; GERLICH, 2015; LOCARNINI et al., 2015; TAJIRI;
SHIMIZU, 2015).
Além da vacina contra hepatite B monovalente, vacinas combinadas também
estão disponíveis e têm sido introduzidas no calendário de vacinação de muitos países,
como a vacina combinada contra hepatites A e B, bem como a vacina pentavalente que
protege contra difteria, tétano, coqueluche, Haemophilus influenzae tipo B e hepatite B
(TREPÓ; CHAN; LOK, 2014).
O esquema de vacinação mais utilizado é a administração de três doses (0, 1
e 6 meses) da vacina monovalente por via intramuscular, embora cronogramas acelerados
e/ou com maior número de doses têm sido considerados em grupos populacionais
específicos (CDC, 2015a; FRANCO et al., 2012). A vacina pode ser administrada em
qualquer idade, porém recomenda-se iniciar o esquema nas primeiras 24 horas de vida,
uma vez que a eficácia é maior em recém-nascidos, crianças e jovens. O esquema vacinal
completo induz níveis de anticorpos protetores (título de anti-HBs ≥ 10 mUI/mL) em
30
aproximadamente 95% dos indivíduos saudáveis. Entretanto, idade avançada, obesidade,
tabagismo, uso abusivo de álcool, hemodiálise, diabetes mellitus tipo 1 e imunossupressão
são fatores relacionados à menor resposta ou até mesmo a não resposta à vacina contra o
HBV. Embora a duração da proteção conferida pela vacina seja controversa, estudos
mostram que, mesmo após os títulos de anti-HBs diminuírem a níveis indetectáveis, a
proteção contra o HBV persiste devido a memória imunológica. Assim, até o momento,
não é recomendado o reforço para indivíduos saudáveis que completaram o esquema
(CDC, 2015a; FRANCO et al., 2012; KOMATSU, 2014; ORLANDO et al., 2015; WHO,
2015a; 2015b).
Em 1992, a OMS recomendou que a vacinação contra o HBV deveria ser
incluída no sistema de imunização infantil de todos os países. Essa estratégia resultou em
uma diminuição considerável da infecção crônica pelo HBV e da transmissão desse vírus
em várias regiões do mundo (CHANG, 2014; MEIRELES; MARINHO; VAN DAMME,
2015; ORLANDO et al., 2015; WHO, 2009; 2015b).
No Brasil, a implementação da vacina contra hepatite B ocorreu
gradativamente pelo Programa Nacional de Imunização (PNI). A partir do ano de 1989,
a vacina foi introduzida em algumas regiões devido à prevalência elevada, como na
Amazônia. Posteriormente, foi estendida a grupos populacionais considerados em risco.
Somente em 1998, a vacina passou a ser disponibilizada para todos os recém-nascidos até
um ano de idade em todo o País. Em 2001, a vacinação foi ampliada para menores de 20
anos. No ano de 2011, contemplou-se a faixa etária de 20 a 24 anos. Em 2012, a vacina
foi disponibilizada para a população até 29 anos de idade. No ano de 2013, a mesma foi
recomendada para os indivíduos até 49 anos de idade (BRASIL, 2013). Por fim, o
Ministério da Saúde ampliou a oferta da vacina contra a hepatite B para toda população
independentemente da idade e ou condições de vulnerabilidade (BRASIL, 2015).
Além disso, vale destacar a disponibilidade gratuita da vacina contra hepatite
B, ao longo dos últimos anos, para grupos populacionais considerados com maior
vulnerabilidade, tais como: gestantes, profissionais da saúde, bombeiros, policiais
militares/civis/rodoviários, carcereiros, reclusos, caminhoneiros, coletadores de lixo,
manicures, assentados, politransfundidos, doadores de sangue, vítimas de abuso sexual,
lésbicas, gays, bissexuais e transgêneros (LGBT), profissionais do sexo, portadores de
IST e usuários de drogas injetáveis/inaláveis (BRASIL, 2008; 2010b; 2013).
A vacina contra o HBV, em sua apresentação monovalente, é disponibilizada
pelo SUS para indivíduos acima de cinco anos de idade, sendo administrada no esquema
31
tradicional de três doses (0, 1 e 6 meses). Adicionalmente, a vacina monovalente é
recomendada para crianças ao nascer (preferencialmente nas primeiras 12 horas de vida),
seguida de três doses, com intervalo de 60 dias, da vacina pentavalente (difteria, tétano,
coqueluche, hepatite B e Haemophilus influenzae tipo B) (BRASIL, 2012; 2015).
A vacina nacional contra a hepatite B (VrHB-IB) tem sido produzida pelo
Instituto Butantan, utilizando tecnologia de DNA recombinante. Essa vacina contém o
HBsAg expresso pela levedura Hansenula polymorpha e, inicialmente, foi produzida com
o antígeno na concentração de 20 µg/mL. Entretanto, após estudos de equivalência,
verificou-se que a vacina era menos imunogênica em adultos, quando comparada à vacina
de referência Engerix B, da Glaxo Smith Kline (20 µg/mL). Diante disso, a concentração
do antígeno na VrHB-IB foi aumentada para 25 µg/mL para adultos. A metade dessa dose
(12,5 µg/mL) é administrada em crianças e adolescentes. Assim, a vacina brasileira
VrHB-IB modificada foi considerada equivalente à vacina de referência e seu uso
recomendado para todas as faixas etárias (LUNA et al., 2009; MORAES; LUNA;
GRIMALDI, 2010).
Outra forma de prevenir a infecção pelo HBV é a imunização passiva, baseada
na administração de imunoglobulina humana anti-hepatite B (HBIG), contendo um título
elevado de anticorpos específicos. A HBIG é normalmente administrada junto com a
vacina, sendo indicada para prevenir a transmissão vertical em neonatos e para pessoas
não vacinadas após a exposição a uma situação de risco (profilaxia pós-exposição), por
exemplo: vítimas de abuso sexual, comunicantes sexuais de caso agudo de hepatite B,
vítimas de acidentes com material biológico HBsAg positivo, ou fortemente suspeito de
infecção por HBV, e imunodeprimidos após exposição de risco. Além dessas exposições,
a imunoglobulina também é utilizada em indivíduos infectados pelo HBV que tenham
sido submetidos a transplante de fígado, de modo a evitar a reinfecção (ASPINALL et
al., 2011; BRASIL, 2010b; ORLANDO et al., 2015).
1.11 Hepatite B em homens que fazem sexo com homens
A expressão HSH (homens que fazem sexo com homens), amplamente
utilizada na área de saúde pública, refere-se a homens que têm relações sexuais com
outros homens, independente da motivação para a prática sexual ou identificação em
alguma “comunidade” específica (BRASIL, 2004; DE VRIES, 2014; WHO, 2011).
Assim sendo, o termo HSH abrange homossexuais e bissexuais do sexo masculino, bem
32
como homens que se consideram heterossexuais e fazem sexo com outros homens por
diversas razões. No âmbito da epidemiologia, pessoas transgêneras (travestis e
transexuais) têm sido incluídas nessa população, embora exista uma tendência para
desvincular esse grupo dos HSH (WHO, 2011).
Por ser uma IST, alguns grupos populacionais são considerados de maior
vulnerabilidade para a infecção pelo HBV. Dentre eles, se destacam os homens que fazem
sexo com homens, por apresentarem taxas de prevalência de IST superiores às
encontradas na população em geral (BRASIL, 2007; CHOW et al., 2014; SOARES et al.,
2014; TSENG et al., 2012; URBANUS et al., 2009).
Tendo em vista os estudos conduzidos na população de HSH (Quadro 3),
verifica-se que a prevalência global da infecção pelo HBV variou de 0,9% no Líbano
(KASSAK et al., 2011) a 52,9% em Taiwan (em HIV soropositivos) (TSENG et al.,
2012), enquanto que a do HBsAg variou de 0% na cidade de Colon no Panamá (HAKRE
et al., 2014) a 16,4% em HSH infectados pelo HIV em Taiwan (TSENG et al., 2012). No
Brasil, duas coortes realizadas no Rio de Janeiro, para determinar a incidência do HIV
em homens homossexuais e bissexuais, mostraram uma prevalência global para o HBV
de 47,9% (SUTMOLLER et al., 1997) e de 37,2% (SUTMOLLER et al., 2002) nos
indivíduos inicialmente recrutados. Mais recentemente, um estudo conduzido na
população de HSH em Campinas-São Paulo (SP) apresentou uma prevalência de 11,4%
e 2,3% para os marcadores anti-HBc e HBsAg, respectivamente (SOARES et al., 2014).
A prevalência elevada da infecção pelo HBV em conjunto com a transmissão
associada ao sexo anal desprotegido, múltiplos parceiros sexuais e histórico de IST
tornam os HSH propensos a se infectarem com esse vírus (DE VRIES, 2014; PANDO et
al., 2006; REMIS et al., 2000; URBANUS et al., 2009). Além disso, o estigma social e a
homofobia também colocam essa população em maior risco de depressão, uso de
substâncias ilícitas e comportamentos sexuais de risco (DE VRIES, 2014; RISHER et al.,
2013; SABIDÓ et al., 2015).
Segundo dados do CDC (2013), cerca de 20% dos casos novos de infecção
pelo vírus da hepatite B, em adultos, ocorrem entre gays e homens bissexuais. Ainda, van
Houdt et al. (2012) verificaram que 23% dos HSH, que se infectaram na idade adulta, se
tornaram portadores crônicos do HBV. Índice esse superior ao observado na população
em geral (5%) (WHO, 2015a), o que pode indicar um pior prognóstico da doença em
HSH. Contudo, nesse estudo, não foi possível elucidar o determinante para a cronificação
da hepatite B em HSH adultos. Assim, mais estudos são necessários para confirmar esse
33
achado, bem como para avaliar os mecanismos envolvidos no desenvolvimento da
infecção crônica.
Estudos moleculares evidenciam a circulação de isolados idênticos do
genótipo A do HBV em HSH em países da Europa e Japão (FUJISAKI et al., 2011;
KOIBUCHI et al., 2001; VAN HOUDT et al., 2010). Na Argentina, Trinks et al. (2008)
verificaram a predominância do genótipo F em HSH. Pesquisas realizadas no Canadá e
na Holanda sugerem que o genótipo G está circulando, principalmente, entre HSH
(OSIOWY et al., 2008; VAN DER KUYL et al., 2013). No Brasil, foi identificado em
um paciente HSH a cocirculação dos genótipos G e F, bem como a recombinação dos
mesmos (ARAUJO et al., 2013).
Quanto a detecção de mutações no genoma do HBV em HSH, Fujisaki et al.
(2011) observaram mutações na região da polimerase do HBV (rtV173L, rtL180M,
rtM204V) relacionadas à resistência a lamivudina em um caso de HSH, virgem de
tratamento, no Japão. Ainda, mutação de escape vacinal (sS143L) também foi relatada
em HSH na Alemanha (INGILIZ et al., 2012).
Apesar da vacina contra hepatite B estar disponível desde 1982, e a
Organização Mundial de Saúde recomendar que os HSH sejam incluídos nos grupos
estratégicos para imunização, nota-se que a cobertura vacinal nessa população permanece
abaixo do ideal em vários países (CHOI et al., 2005; CHOW et al., 2014; KASSAK et al.,
2011; LINKINS et al., 2013; PITASI et al., 2014; WHO, 2011).
No Brasil, apenas 29% dos HSH estudados em Campinas-SP apresentaram o
marcador anti-HBs isolado, indicando vacinação prévia, e mais de 50% dos participantes
foram negativos para qualquer marcador sorológico do HBV, sendo assim suscetíveis à
infecção (SOARES et al., 2014).
34
Quadro 3 - Estudos de prevalência da infecção pelo vírus da hepatite B em homens que fazem
sexo com homens
Referência
Bleeker et al. (1981)
Local
População
Amsterdã,
Holanda
Boston, EUA
Rio de Janeiro,
Brasil
Carachi,
Paquistão
HSH em sauna
diurna; noturna
Gays e bissexuais
HSH
N
Prevalência (%)
HBsAg
Globala
134; 184
3,0; 8,7
-
508
318
-
12,9
47,9
Travestis
208
3,4
-
Montreal, Canadá
HSH
HIV negativos
328
4,3
41,0
EUA
HSH
3.432
-
11,0
Rio de Janeiro,
Brasil
Washington, EUA
HSH
1165
4,0
37,2
HSH
Travestis
profissionais do
sexo
HSH
HIV negativos
833
1,0
13,3
200
3,0
50,5
903
-
19,0
HSH
489
8,2
28,0
HSH
3.334
1,0
12,0
HSH
681
-
37,7
Pequim, China
HSH
(ano: 2004; 2005;
2006)
325; 427;
540
7,5; 8,0;
10,3
-
Zagreb, Croácia
HSH
360
0,9
9,2
Pequim, China
Zanzibar,
Tanzânia
Paquistão
Peru
Líbano
HSH
HSH UDI; não
UDI
HSH
HSH
HSH
541
6,5
-
66; 443
-
3,8; 4,5
396
2.703
101
8,1
2,8
0,9
20,2
0,9
Porto Rico
HSH
41
-
4,9
Dos Ramos Farías et
al. (2011)
Argentina
Homens
profissionais do
sexo; transexuais
profissionais do
sexo
82; 264
1,2; 1,9
22,0; 40,2
Pando et al. (2012)b
Buenos Aires,
Argentina
HSH
496
-
22,9
Tseng et al. (2012)
Taiwan
HSH
HIV positivos;
HIV negativos
438; 690
16,4; 6,2
52,9; 20,3
Seage et al. (1997)
Sutmoller et al. (1997)
Baqi et al. (1999)
Remis et al. (2000)
MacKellar et al.
(2001)
Sutmoller et al. (2002)
Diamond et al. (2003)
Russi et al. (2003)
Jin et al. (2004)
Sydney, Austrália
Choi et al. (2005)
McMillan (2006)
Pando et al. (2006)
Ma et al. (2007)
Montevideo,
Uruguai
b, c
Bozicevic et al.
(2009)b, c
Ruan et al. (2009)
Johnston et al.
(2010)b,c
Khanani et al. (2010)b
Lama et al. (2010)
Kassak et al. (2011)b
Cólon-López et al.
(2011)
São Francisco,
EUA
Edimburgo,
Escócia
Buenos Aires,
Argentina
35
Quadro 3 (continuação) - Estudos de prevalência da infecção pelo vírus da hepatite B em homens
que fazem sexo com homens
Referência
Local
Van Houdt et al.
(2012)
Wang et al. (2012)
Linkins et al. (2013)
Amsterdã,
Holanda
Pequim, China
Bancoque,
Tailândia
Soares et al. (2014)b, c
1.862
12,0
44,0
HSH
1.111
6,1
26,5
HSH
1.117
9,2
39,6
-
52,4
Trípoli, Líbia
China
227
35.203
2,9
8,9
-
Vitória, Austrália
HSH
10.031
3,7
10,6
HSH
204; 306;
93 c
2,2; 3,4;
0
10,0;
29,4;
40,6
HSH
345
1,5
19,4
143
9,8
-
558
2,3
11,4
1.843
1,7
28,8
Valadez et al. (2013)b, c
Chow et al. (2014)
Gamagedara et al.
(2014)
Prasetyo et al. (2014)b
HSH
267
Hollywood, EUA
Pitasi et al. (2014)
N
Gays e bissexuais
desabrigados
HSH
HSH
Nyamathi et al. (2013)
Hakre et al. (2014)b, c
Prevalência (%)
HBsAg
Globala
População
David; Cidade do
Panamá; Colon,
Panamá
Los Angeles,
EUA
Surakarta,
Indonésia
Campinas, Brasil
HSH
HSH
HSH
HIV positivos
Jansen et al. (2015)
Alemanha
Nielsen et al. (2015)
Aarhus,
Dinamarca
HSH
141
1,4
7,0
Remis et al. (2016)
Toronto, Canadá
HSH
HIV positivos;
HIV negativos
294; 148
2,7; 0,7
49,4; 19,1
HSH: homens que fazem sexo com homens; EUA: Estados Unidos da América; HIV: vírus da imunodeficiência
humana; UDI: usuários de drogas injetáveis.
a
Presença de qualquer marcador de infecção pelo HBV; b Recrutamento da população utilizando RDS; c Prevalência
ponderada pelo RDSAT
1.12 Métodos de amostragem em populações de difícil acesso
Um grande desafio para estudos epidemiológicos em grupos populacionais
com maior vulnerabilidade para infecção pelo HIV e outras IST é a obtenção de amostras
representativas. Uma vez que muitos desses grupos, como usuários de drogas,
profissionais do sexo e HSH, são considerados ocultos ou de difícil acesso por estarem
vinculados a comportamentos estigmatizados ou atividades ilegais (KENDALL et al.,
2008; MAGNANI et al., 2005; PENROD et al., 2003).
Para lidar com tal dificuldade, diferentes métodos de amostragem foram
propostos para aumentar a eficiência de recrutamento desses grupos populacionais. A
técnica de amostragem denominada bola de neve (snowball) foi utilizada, aumentando a
36
identificação e inclusão de participantes de populações de difícil acesso, uma vez que
membros da população-alvo eram responsáveis por recrutar novos membros, formando
cadeias de recrutamento (BIERNACKI; WALDORF, 1981; MAGNANI et al., 2005).
A amostragem por bola de neve aumenta o acesso e a eficiência no
recrutamento de populações ocultas, porém não permite uma amostragem probabilística
(HECKATHORN, 2011). Assim, a partir da década de 90, outras metodologias de
amostragem probabilística foram propostas para permitir uma estimativa estatística das
variáveis de interesse. Nesse contexto, pode-se destacar as técnicas de amostragem
tempo-local (Time-Location Sampling - TLS) (STUEVE et al., 2001) e a dirigida pelo
entrevistado (Respondent-Driven Sampling - RDS) (HECKATHORN, 1997).
O método TLS é baseado na ideia de que as populações de difícil acesso
tendem a se reunir em locais específicos (discotecas, bares, saunas ou parques). Após
mapear os locais onde a população-alvo pode ser encontrada, seleciona-se o dia, hora e
local do recrutamento, havendo uma seleção sistemática dos participantes. No entanto, o
TLS inclui apenas aqueles que frequentam os locais selecionados, podendo excluir uma
parcela da população que frequenta ambientes diferentes (KENDALL et al., 2008;
MAGNANI et al., 2005).
A metodologia RDS, proposta em 1997, por Heckathorn, é uma variante da
amostragem por bola de neve e, como tal, o recrutamento é feito pelos membros da
população-alvo. Esses devem estar conectados por uma rede social e a indicação dos
participantes ocorre pelos pares. A seleção dos participantes iniciais, também chamados
“sementes”, é realizada a partir de uma pesquisa formativa que auxilia o pesquisador a
decidir detalhes sobre a implementação do estudo (HECKATHORN, 1997; JOHNSTON
et al., 2010; MCCREESH et al., 2013). Após participar do estudo, as sementes recebem
um número definido de cupons referenciados para recrutar novos membros da populaçãoalvo (onda 1). Esses, por sua vez, também recebem cupons para recrutar novos
participantes (onda 2), de forma que a cadeia de recrutamento se expande com a formação
de novas ondas até atingir o tamanho da amostra desejada (Figura 10). Para garantir a
participação e contínuo recrutamento, são fornecidos incentivos pela participação e por
membro recrutado (JOHNSTON et al., 2016; SALGANIK; HECKATHORN, 2004;
SALGANIK, 2006; WHITE et al. 2015). Adicionalmente, o método RDS permite o
cálculo das probabilidades de seleção por meio de um modelo matemático que pondera a
amostra para compensar possíveis vieses de recrutamento, sendo, assim, classificado
entre os métodos de amostragem probabilística (HECKATHORN, 1997). Para gerar tais
37
estimativas, a análise estatística dos dados é realizada utilizando um programa
computacional denominado RDSAT (RDS Analysis Tool) (VOLZ; HECKATHORN,
2008; WHITE et al., 2012).
Estudos comparativos entre as metodologias de amostragem utilizadas para
recrutamento de HSH destacam as vantagens da utilização do RDS. Esse é o método
sugerido para vigilância do HIV em HSH, podendo ser aplicado em outras IST, devido à
diversidade da amostra produzida, a sua capacidade para limitar a influência de seleção
do investigador e as suas vantagens logísticas (KENDALL et al., 2008; WEI et al., 2012).
Desde que foi proposto, o RDS tem sido amplamente utilizado para vigilância
do HIV e outras IST em grupos populacionais de difícil acesso em todo o mundo
(FORREST et al., 2016; JOHNSTON et al., 2013; LANE et al., 2011; MEDHI et al.,
2012; MONTEALEGRE et al., 2013). No Brasil, essa metodologia vem sendo utilizada
para recrutar mulheres profissionais do sexo (DAMACENA; SZWARCWALD;
BARBOSA JÚNIOR, 2011; FERNANDES F. R. et al., 2014), usuários de drogas
(GUIMARÃES et al., 2015) e homens que fazem sexo com homens (BRIGNOL et al.,
2015; KERR et al., 2013; SOARES et al., 2014).
Figura 10 - Representação gráfica de um recrutamento por RDS (modificada)
Fonte: HHS-CDC (2008)
38
2 JUSTIFICATIVA
Após quase 50 anos da descoberta do HBV e da disponibilidade da vacina por
mais de 30 anos, a hepatite B continua sendo um problema de saúde pública mundial,
estando ainda associada a muitos casos de cirrose, carcinoma hepatocelular e alta taxa de
mortalidade (BRASIL, 2003; BURNS; THOMPSON, 2014; LOZANO et al., 2012; SHI;
SHI, 2009; WHO, 2015a). Tais dados evidenciam a importância de estudos que visam
investigar a infecção pelo HBV em populações específicas, podendo contribuir para
elaboração de estratégias efetivas de prevenção e controle dessa infecção.
A exposição ao vírus da hepatite B ocorre em número considerável de homens
que fazem sexo com homens. A OMS reconhece que essa população apresenta um risco
maior para IST quando comparada à população geral (WHO, 2011). Essa maior
vulnerabilidade envolve o contexto de violência, tipo de prática sexual, acesso limitado
aos serviços de saúde e inserção social, o que reflete na precariedade de adoção de práticas
sexuais seguras, vacinação, testagem e adesão ao tratamento (BRASIL, 2007; DE VRIES,
2014; RISHER et al., 2013). Além disso, de acordo com estudo realizado por van Houdt
et al. (2012), o risco aumentado para o desenvolvimento de hepatite B crônica é um fator
preocupante nessa população. Diante do exposto, estudos epidemiológicos da infecção
pelo HBV em HSH são importantes para auxiliar no direcionamento das políticas públicas
de saúde dirigidas à essa população.
Na tentativa de reduzir os casos de infecção entre homens que fazem sexo
com homens, o Departamento de DST, Aids e Hepatites Virais lançou o Plano Nacional
de Enfrentamento da Epidemia de Aids e das DST entre Gays, HSH e Travestis (BRASIL,
2007). No entanto, as informações epidemiológicas e moleculares da infecção pelo HBV
em HSH no Brasil permanecem escassas. Além disso, os poucos dados disponíveis no
País se restringem à Região Sudeste e não abordam os aspectos moleculares da infecção
(SOARES et al., 2014; SUTMOLLER et al., 1997; 2002).
Diante disso, este é o primeiro estudo realizado na Região Centro-Oeste do
Brasil, com o intuito de investigar o perfil soroepidemiológico e molecular da infecção
pelo vírus da hepatite B em homens que fazem sexo com homens em Goiânia-GO,
utilizando o método RDS. Essa metodologia de recrutamento permite a obtenção de uma
amostragem representativa de grupos populacionais de difícil acesso, como é o caso dos
HSH. Nesta tese, foi investigada a prevalência, os fatores de risco associados à infecção
e a situação vacinal contra hepatite B na população estudada, além da pesquisa de
39
infecção oculta pelo HBV e a caracterização molecular dos isolados virais. Assim, este
estudo poderá subsidiar a elaboração e/ou reestruturação de estratégias específicas para
diagnóstico, prevenção e controle da hepatite B em HSH, visando melhorias na qualidade
de vida e de assistência a este grupo de indivíduos.
40
3 OBJETIVOS
3.1 Objetivo geral
Estudar o perfil soroepidemiológico e molecular da infecção pelo vírus da
hepatite B em homens que fazem sexo com homens em Goiânia-Goiás.
3.2 Objetivos específicos
- Estimar a prevalência dos marcadores sorológicos de exposição ao HBV (anti-HBc) e
de infecção (HBsAg) nos HSH estudados;
- Analisar os fatores associados à infecção pelo HBV nesta população;
- Investigar a ocorrência de infecção oculta pelo vírus da hepatite B nos HSH;
- Identificar os genótipos e subgenótipos do HBV circulantes;
- Verificar a presença de mutações no genoma do HBV;
- Comparar a presença do marcador sorológico anti-HBs com a frequência do auto relato
de vacinação prévia contra a hepatite B na população estudada;
- Analisar os fatores associados à imunização contra o HBV entre os HSH.
41
4 RESULTADOS
Artigo 1: Prevalence, Risk Behaviors, and Virological Characteristics of Hepatitis B
Virus Infection in a Group of Men Who Have Sex with Men in Brazil: Results from a
Respondent-Driven Sampling Survey.
Autores: Marina P. Oliveira, Márcia A. D. Matos, Ágabo M. C. Silva, Carmen L. R.
Lopes, Sheila A. Teles, Marcos A. Matos, Natália Spitz, Natalia M. Araujo, Rosa M. S.
Mota, Ligia R. F. S. Kerr, Regina M. B. Martins.
Revista: PLoS One, v. 11, n. 8, 2016. doi:10.1371/journal.pone.0160916
Artigo 2: Hepatitis B vaccination and associated factors among men who have sex with
men in Brazil.
Autores: Marina P. Oliveira, Ágabo M. C. Silva, Andreia A. Andrade, Edna B. R.
Santana, Nara R. Freitas, Carmen L. R. Lopes, Rosa M. S. Mota, Márcia A. D. Matos,
Regina M. B. Martins.
Revista: Journal of Infection and Public Health (submetido)
42
4.1 Artigo 1
Prevalence, Risk Behaviors, and Virological
Characteristics of Hepatitis B Virus Infection in a
Group of Men Who Have Sex with Men in Brazil:
Results from a Respondent-Driven Sampling Survey
Marina P Oliveira1, Márcia A D Matos1, Ágabo M C Silva1, Carmen L R Lopes2, Sheila
A Teles2, Marcos A Matos2, Natália Spitz3, Natalia M Araujo3, Rosa M S Mota4, Ligia R
F S Kerr4, Regina M B Martins1*
1
Institute of Tropical Pathology and Public Health, Federal University of Goiás, Goiânia,
Goiás, Brazil
2
Faculty of Nursing, Federal University of Goiás, Goiânia, Goiás, Brazil
3
Oswaldo Cruz Institute, Oswaldo Cruz Foundation, Rio de Janeiro, Rio de Janeiro, Brazil
4
Department of Community Health, Federal University of Ceará, Fortaleza, Ceará, Brazil
*Corresponding author
E-mail: [email protected] (RMBM)
Short title: HBV Infection in Brazilian MSM
43
Abstract
Background: Men who have sex with men (MSM) are at increased risk of exposure to
hepatitis B virus (HBV) compared with the general population. This study aims to assess
the epidemiological and virological characteristics of HBV infection in a sample of MSM
in Brazil, where data are scarce.
Methods: A cross-sectional study was conducted among MSM in the City of Goiânia,
Central Brazil, from March to November 2014, using Respondent-Driven Sampling
(RDS). After signing the consent form, participants were interviewed and a blood sample
collected. All samples were tested for HBV serological markers and HBV DNA. HBV
nucleotide sequence analysis was also performed.
Results: A total of 522 MSM were recruited in the study. The prevalence of HBV
infection [current or past (presence of anti-HBc marker)] was 15.4% (95% CI: 8.7-25.8)
and the rate of HBsAg carriers was 0.6% (95% CI: 0.2-1.6). About 40% (95% CI: 32.348.8) of the participants had serological evidence of previous HBV vaccination (reactive
for isolated anti-HBs). In addition, 44.3% (95% CI: 36.1-52.9) were seronegative for all
HBV markers. Age over 25 years old, receptive anal intercourse, previous sex with
women, and history of sexually transmitted infections (STIs) were factors associated with
HBV infection. HBV DNA was detected only in HBsAg-positive individuals. HBV
isolates were classified into genotype A (subgenotypes A1 and A2), and some mutations
were identified throughout the genome. Therefore, occult HBV infection was not
observed in the study population.
Conclusions: Public health strategies should be improved for the MSM population in
order to prevent HBV and other STIs, as well as to provide appropriate management of
patients with active infections.
44
Introduction
Hepatitis B virus (HBV) infection has a wide global distribution. The World
Health Organization (WHO) estimates that there are over 240 million chronically infected
people worldwide. The chronic form of this infection is associated with a variety of
clinical manifestations, ranging from an asymptomatic carrier state to severe liver disease,
including cirrhosis and hepatocellular carcinoma (HCC) [1].
The traditional serological marker of hepatitis B is the HBV surface antigen
(HBsAg), which is detectable in serum during acute and chronic infection. However, with
the development of highly sensitive molecular biology techniques, HBV DNA has been
detected in serum and/or liver without detectable HBsAg. This profile is called occult
HBV infection (OBI) and has been associated with hepatitis B reactivation, increased
severity of liver disease, and HCC development. In addition, an increased risk of HBV
transmission through blood transfusion, organ transplantation, and hemodialysis due to
OBI has been reported [2,3].
HBV isolates are classified into ten genotypes, designated A-J, based on sequence
divergence greater than 7.5% in the complete genome. Most genotypes further segregate
into subgenotypes that differ from each other by 4-7.5%. HBV genotypes/subgenotypes
have different geographical distributions, and influence clinical outcomes and response
to treatment [4,5]. In Brazil, genotype A is the most prevalent, followed by genotypes D
and F, with a higher proportion of subgenotype A1 [6,7].
The genetic variability of HBV can lead to the occurrence of different diagnosis
and clinical profiles. Mutations in the Pre-S/S gene region have been linked to low HBsAg
levels and HBV vaccine/immunoglobulin escape, whereas those found in the Pre-C/C and
BCP (basal core promoter) gene regions can lead to decreased hepatitis B e antigen
(HBeAg) expression and to progression to severe liver disease [8,9].
45
HBV infection occurs in a considerable number of men who have sex with men
(MSM). According to the US CDC [10], about 20% of new cases of HBV infection in
adults in the United States of America occur among gay and bisexual men. In addition, a
high rate of chronic hepatitis B was reported in MSM [11]. Some studies have shown that
MSM are at high risk of sexually transmitted infections (STIs), including hepatitis B [1218]. This greater vulnerability involves the context of violence, conditions of sexual
practices such as unprotected anal intercourse and multiple sexual partners in addition to
low access to health services and social integration, which can lead to unsafe sexual
practices [13,17].
Worldwide, HBV infection prevalence in MSM varies according to geographical
region as well as with the characteristics of the selected subgroup studied. Thus, the
prevalence of this infection in MSM has ranged from 0.9% in Lebanon [19] to 44% in the
Netherlands [11]. In addition, higher HBV rates have been described in specific
subgroups of MSM, such as gays and bisexuals homeless young adults in USA (52.4%)
[20], HIV-positive MSM in Taiwan (52.9%) [16] and male transvestite commercial sex
workers in Uruguay (50.5%) [21].
In Brazil, previous [22,23] and current [15] studies concerning HBV prevalence
among MSM are still rare, and no data regarding the molecular epidemiology of HBV in
MSM has been published thus far. Therefore, this study was conducted in order to
investigate the HBV prevalence, associated factors, occult infection rate and molecular
characterization of viral isolates in MSM in Central Brazil.
Material and Methods
Study population and sampling method
46
A cross-sectional study among MSM was conducted in Goiânia (1,256,514
inhabitants), the capital of the State of Goiás in Central Brazil. From March to November
2014, a total of 522 MSM were recruited using Respondent-Driven Sampling (RDS), a
chain-referral sampling method in which initial participants, called seeds, recruit a limited
number of additional participants. These participants recruit more participants and this
process goes on until the desired sample size is reached. This recruitment strategy is an
efficient data collection method and it is useful to study hidden populations such as MSM
[24,25]. Initially, formative research was conducted to determine study logistics and to
select the seeds. Based on their extensive social network, three seeds were first selected
by collaborating with governmental and non-governmental organizations supporting
LGBT (Lesbian, Gay, Bisexual and Transgender) individuals and during the gay pride
parade. Additionally, two more seeds were included during the study to enroll additional
participants. Each seed received three numbered referral coupons to invite other eligible
MSM to the study (first wave). Eligibility criteria for participation were being born male
sex, aged 18 years or older, leaving in the Goiânia metropolitan area, reporting have had
sex with another man in the 12 months preceding the study, do not identify as transsexual,
and presenting a valid recruitment coupon.
Considering that MSM is a hard-to-reach population, the sample size calculation
took into consideration the expected design effect of 2.0 [26]. The minimum sample size
of 418 participants was calculated using an estimated prevalence for exposure to HBV of
11.4% [15], with confidence interval of 95% and a precision of 4.4%. Due to the return
of some coupons previously issued, the sample size reached 522.
After being informed of the objectives and methodology of the study, individuals
signed the consent form and answered an interviewer-administered structured
questionnaire to collect information about their personal network size, relationship with
47
the recruiter, sociodemographic characteristics and possible factors associated with HBV
infection. Then, a blood sample was collected from each participant for laboratory testing.
All participants received three referral coupons to recruit new MSM of their social
relationships (friends and/or sexual partners), in addition to educational materials and
condoms. As an incentive, each participant received four public transportation tickets and
two additional transportation tickets for each participant they recruited into the study.
The procedures of this study were approved by the Ethics Committee of the
Federal University of Goiás (UFG), Goiânia, Goiás, Brazil. All participants signed
informed written consent. This consent form was approved by the ethics committee.
Serological tests
Serum samples were tested by enzyme-linked immunosorbent assay (ELISA) for
detection of HBsAg (Hepanostika HBsAg Ultra, Biomérieux, Boxtel, The Netherlands),
antibodies against hepatitis B core antigen (anti-HBc) (Hepanostika anti-HBc Uni-form,
Biomérieux), and antibodies against HBsAg (anti-HBs) (Bioelisa anti-HBs, Biokit,
Barcelona, Spain). HBsAg reactive samples were subsequently tested for the presence of
anti-HBc IgM (Bioelisa anti-HBc IgM, Biokit), HBeAg and antibodies against HBeAg
(anti-HBe) (Eti-Ab/Ebk Plus, Diasorin, Italy).
Molecular tests
DNA was extracted from all samples using phenol-chloroform method [27]. The
Pre-S/S region was amplified by semi-nested polymerase chain reaction (PCR) [28]. HBV
DNA-positive samples were submitted to amplification of the complete genome [29].
When the full-length genome amplification was not successfully achieved, the S, BCP,
and Pre-C/C gene regions were further amplified, as previously described [28].
48
Nucleotide sequences of the amplified regions were determined by direct sequencing
using a BigDye Terminator 3.1 cycle sequencing kit (Applied Biosystems, Foster City,
CA), on an ABI 3130 automated sequencer (Applied Biosystems). Sequences were
aligned and edited using SeqMan II v.5.01 (DNASTAR), Clustal W and BioEdit. HBV
genotypes and subgenotypes were determined by phylogenetic analysis using MEGA
program v.6.0 (Molecular Evolutionary Genetics Analysis) and published reference
sequences available in GenBank database (http://www.ncbi.nlm.nih.gov/). To identify
mutations in the HBV genome, the deduction of amino acids (aa) was performed from
nucleotide sequences by using MEGA program v.6.0. The nucleotide sequences obtained
in this study were deposited in GenBank under the accession numbers KU900750 to
KU900754.
Data analysis
Prevalence and 95% confidence intervals (CI) were estimated using RDS Analysis
Tool (RDSAT) v.5.6 (http://rds-analysis-tool.software.informer.com/versions/). To
reduce possible biases associated with chain referral sampling, RDSAT provides weights
for each participant based on his social network size and recruitment patterns [24]. Data
and weights generated through RDSAT were exported to SPSS v.20 (SPSS Inc., IBM,
Chicago, US) for weighted analysis of variables associated with HBV infection [current
or past (defined by the presence of anti-HBc serological marker)] using Pearson’s chisquare test and Fisher’s exact test. Variables associated with this infection at p≤0.10 in
the univariate analysis were included in the multivariable analysis using a logistic
regression model. Finally, a p-value less than 0.05 was considered statistically significant.
The design of social networks to visualize the distribution of the HBV exposure in the
49
recruitment
network
was
performed
using
NetDraw
software
(http://www.analytictech.com/downloadnd.htm).
Results
Sampling
Of a total of 1,227 coupons issued, 530 (43.2%) were redeemed. Among the 530
MSM who presented a valid recruitment coupon, eight were not selected (two refused to
give a blood sample and six were under 18 years old). Therefore, 522 MSM were included
in the analysis (5 seeds and 517 recruits). The median number of waves by seed was 9
(range 3-15), and the median number of recruits by seed was 103 (range 15-169).
Characteristics of participants
The sociodemographic characteristics of the study population are shown in Table
1. Participants were mostly young (≤25 years old, 60%). The majority self-identified as
gay (74.9%), followed by bisexual (19.4%) and transvestite (5.7%). Skin color was
assessed by self-report (59% claimed brown or mixed (pardo), 18.9% white, 16.6% black
and 5.6% others). Most of MSM were single (76.9%), previously attended high school
(10-12 years of study, 63.9%) and were in the lowest tier of Brazilian social class (61.3%).
50
Table 1. Sociodemographic characteristics of 522 MSM in Goiânia, Central Brazil.
N
Unweighted
%
Weighted %
95% CI
≤ 25 years
338
64.75
60.0
50.8-68.5
> 25 years
184
35.25
40.0
31.5-49.2
Gay
355
68.0
74.9
67.2-81.4
Bisexual
76
14.6
19.4
13.4-27.2
Transvestite
91
17.4
5.7
3.8-8.3
Brown (pardo)
296
56.7
59.0
50.0-67.4
White
103
19.7
18.9
13.5-25.7
Black
91
17.4
16.6
9.9-26.4
Yellow (Asian)
21
4.0
4.1
1.7-9.2
Indigenous
11
2.1
1.5
0.7-3.4
Single
420
80.5
76.9
66.9-84.5
Married/in stable relationship
94
18.0
20.1
12.9-9.9
Separated/divorced
8
1.5
3.1
0.9-9.4
≤9
77
14.8
13.7
9.0-20.3
10 - 12
307
59.0
63.9
55.9-71.3
≥ 13
136
26.2
22.4
17.0-28.9
A/B (≥ R$ 8,641)
7
1.4
0.4
0.1-1.7
C (R$ 2,005 - 8,640)
81
15.5
9.9
6.6-14.5
D (R$ 1,255 - 2,004)
140
26.8
28.4
20.3-38.3
E (≤ R$ 1,254)
294
56.3
61.3
52.1-69.7
Characteristics
Age (median: 23.6; range: 18-62)
Self-identification
Skin color/race
Marital status
Education (years) (n=520)
a
Social class (Brazilian criteria)b
MSM, men who have sex with men; CI, confidence interval; R$, Brazilian real.
a
Missing data are not shown.
b
Brazilian criteria classifies individuals into five economic classes [30]: “A” constitutes the highest tier of social class,
while “E” the lowest one (US$ 1.00 is approximately equal to R$ 2.32).
Prevalence of HBV serological markers
Table 2 shows the prevalence of HBV serological markers. Among the 522 MSM
studied, 77 (15.4%; 95% CI: 8.7 to 25.8) had been exposed to HBV. Of these, 5 (0.6%)
were anti-HBc/HBsAg carriers, 60 (9.3%) were reactive for anti-HBc/anti-HBs and 12
(5.5%) were positive for anti-HBc only. Moreover, 206 (40.3%) were reactive for isolated
51
anti-HBs. In addition, 239 (44.3%) were seronegative for all hepatitis B serological
markers. The representation of the recruitment network indicating cases of exposure to
HBV is presented in Fig 1.
Table 2. Prevalence of HBV serological markers among 522 MSM in Goiânia,
Central Brazil.
Unweighted
Weighted % (95%
HBV markers
Total
%
CI)
Anti-HBc/ HBsAg
5
1.0
0.6 (0.2-1.6)
Anti-HBc/ anti-HBs
60
11.5
9.3 (5.9-14.5)
Anti-HBc only
12
2.3
5.5 (1.2-21.8)
Any exposure marker
77
14.8
15.4 (8.7-25.8)
Anti-HBs (immunized)
206
39.5
40.3 (32.3-48.8)
marker 239
45.8
44.3 (36.1-52.9)
Absence
of
(susceptible)
any
HBV, hepatitis B virus; MSM, men who have sex with men; CI, confidence interval; HBsAg, hepatitis B
surface antigen; anti-HBc, antibodies against hepatitis B core antigen; anti-HBs, antibodies against HBsAg.
Fig 1. Recruitment networks of 522 men who have sex with men in Goiânia, Central
Brazil. The seeds are indicated by large squares and recruits by small squares. Individuals
who had been exposed to HBV are in black and others in gray.
Factors associated with HBV infection
Univariate analysis of demographic, behavioral characteristics, and HIV
serological status among unvaccinated MSM (Table 3) revealed that age over 25 years,
more than 10 sex partners in lifetime, history of drugs or alcohol use during sex, receptive
anal intercourse, previous sex with women and history of STIs were statistically
associated with HBV infection (p<0.05). These variables in addition to ever having
received payment for sex (p=0.055) and HIV seropositivity (p=0.079) were included in a
multivariate analysis using a logistic regression model. Age over 25 years old (p<0.001),
52
receptive anal intercourse (p=0.001), previous sex with women (p=0.038), and history of
STIs (p=0.001) were independent factors associated with HBV infection in the study
population (Table 4).
53
Table 3. Demographic, behavioral characteristics and HIV serological status
associated with HBV infection among unvaccinated MSM in Goiânia, Central
Brazil.
Variable
Age (years)
≤ 25
> 25
Self-identification
Gay
Bisexual
Transvestite
Number of sexual
partners in lifetime
≤ 10
> 10
Ever used drugs or
alcohol during sex
No
Yes
Ever received
payment for sex
No
Yes
Receptive anal
intercourse
No
Yes
Condom use at anal
intercourse
Always
Not Always
Sex with women
No
Yes
Group sex
No
Yes
Sex against will
No
Yes
STIs
No
Yes
HIV status
Negative
Positive
Ever used any illicit
drug
No
Yes
Blood transfusion
lifetime
No
Yes
HBV
Pos./total
Unweighted
%
Weighted %
(95% CI)
OR (95% CI)
P
value
22/183
55/133
12.0
41.3
5.2 (2.4-10.8)
46.3 (28.1-65.5)
1
15.73 (5.10-48.39)
49/207
17/61
11/48
23.7
27.9
22.9
28.0 (14.8-46.6)
27.7 (12.7-50.4)
16.5 (5.9-38.4)
1.96 (0.48-8.02)
1.94 (0.43-8.78)
1
16/93
61/223
17.2
27.3
11.9 (5.9-22.6)
35.1 (19.3-55.0)
1
3.99 (1.30-12.23)
0.012
20/102
57/214
19.6
26.6
13.6 (7.0-24.8)
33.4 (18.0-53.4)
1
3.19 (1.10-9.65)
0.034
45/173
32/143
26.0
22.4
17.6 (11.5-26.1)
41.5 (18.3-69.3)
1
3.32 (0.94-11.69)
0.055
11/57
66/259
19.3
25.5
7.0 (2.6-17.5)
32.3 (18.9-49.5)
1
6.35 (1.80-22.53)
0.002
30/157
47/159
19.1
29.5
22.5 (9.0-46.1)
31.3 (18.9-47.2)
1
1.57 (0.44-5.62)
0.484
32/169
45/147
18.9
30.6
15.2 (9.4-23.7)
34.3 (17.3-56.6)
1
2.91 (1.00-8.48)
0.045
28/142
49/172
19.7
28.5
26.3 (11.2-50.1)
26.5 (15.4-41.5)
1
1.01 (0.29-3.49)
0.987
57/216
19/98
26.4
19.4
24.2 (12.2-42.4)
32.1 (15.4-55.0)
1
1.48 (0.42-5.24)
0.543
44/232
33/82
18.9
40.2
12.0 (7.4-18.8)
57.7 (31.9-79.9)
1
10.02 (3.04-33.08)
<0,001
54/246
23/70
21.9
32.8
20.6 (9.2-39.9)
45.2 (24.4-67.8)
1
3.17 (0.84-11.93)
0.079
35/155
42/160
22.6
26.2
23,6 (14,2-36,6)
26.5 (13.4-45.5)
1
1.17 (0.41-3.32)
0.772
70/294
6/17
23.8
35.3
25.5 (14.4-41.0)
31.3 (9.4-66.6)
1
1.33 (0.26-6.87)
0.117
0.000
0.493
HBV, hepatitis B virus; MSM, men who have sex with men; CI, confidence interval; OR, odds ratio; STIs, sexually
transmitted infections; HIV, human immunodeficiency virus.
54
Table 4. Multivariate analysis of factors associated with HBV infection among MSM
in Goiânia, Central Brazil.
Variable
Age (years)
≤ 25
> 25
Number of sexual partners in lifetime
≤ 10
> 10
Ever used drugs or alcohol during sex
No
Yes
Ever received payment for sex
No
Yes
Receptive anal intercourse
No
Yes
Sex with women
No
Yes
STIs
No
Yes
HIV status
Negative
Positive
Adjusted OR (95% CI)a
P value
1
11.32 (4.08-31.42)
<0.001
1
1.68 (0.52-5.45)
0.386
1
1.65 (0.61-4.47)
0.321
1
0.81 (0.27-2.44)
0.702
1
11.60 (2.60-51.72)
0.001
1
2.83 (1.06-7.56)
0.038
1
5.79 (2.16-15.56)
0.001
1
2.01 (0.75-5.42)
0.164
HBV, hepatitis B virus; MSM, men who have sex with men; CI, confidence interval; STIs, sexually transmitted
infections; HIV, human immunodeficiency virus; aAdjusted odds ratio for the following variables: age, number of
sexual partners in lifetime, use of drugs or alcohol during sex, received payment for sex, receptive anal intercourse, sex
with women, STIs and HIV.
Characteristics of HBV DNA positive samples
Of the 522 samples, HBV DNA was detected only in the five anti-HBc/HBsAg
positive ones. Thus, occult HBV infection was not observed in the study population.
Relative to HBV DNA positive samples (Table 5), two and three were HBeAg and antiHBe reactive, respectively. Anti-HBc IgM marker was not detected in any of these
samples. Two samples (Y431 and Y494) were successfully amplified for full-length HBV
genome, one (Y513) for Pre-S/S, BCP and Pre-C/C, one (Y02) for Pre-S/S, and one
(Y413) for S gene region. Sequence analysis of these samples revealed that all HBV
isolates had the T131N amino acid substitution in the S gene. In addition, analysis of BCP
and Pre-C/C gene regions showed the double mutation A1762T/G1764A in sample Y431,
55
G1862T/G1888A in Y494, and G1862T in Y513. No mutations were detected in X and
overlapping HBV polymerase gene regions.
Table 5. Hepatitis B virus biomarkers in MSM with HBV DNA positive in Goiânia,
Central Brazil.
Serological markers
HSH
Age
(years)
Y02
Y413
Y431
37
Y494
37
Y513
26
39
52
Mutations
HBeAg
Anti-HBe
Genome/
regions
amplified
+
-
+
Pre-S/S
S
T131N
T131N
-
+
Full genome
T131N
+
-
Full genome
T131N
-
+
Pre-S/S, BCP
and Pre-C/C
T131N
S region
BCP and
Pre-C/C
region
A1762T,
G1764A
G1862T,
G1888A
Subgenotype
G1862T
A1
A2
A1
A2
A1
HBV, hepatitis B virus; MSM, men who have sex with men; HBeAg, hepatitis B e antigen; anti-HBe,
antibodies against HBeAg; BPC, basal core promoter.
Phylogenetic analysis of the S gene showed that the five isolates belonged to HBV
genotype A, subgenotypes A1 (n=3) and A2 (n=2) (Fig 2). These results were further
confirmed by analysis of other amplified genomic regions.
Fig 2. Phylogenetic tree analysis of the S region of hepatitis B virus (HBV). The
phylogenetic tree performed by using the CLUSTAL W program and analyzed by Kimura
two-parameter methods. Genetic distances were calculated by the maximum composite
likelihood. Phylogenetic tree was constructed by the neighbor-joining method using
MEGA v.6.0 software (bootstrap resampling test with 1,000 replicates), including 5
isolates from Brazilian MSM (black square), 33 GenBank sequences of genotypes A–J
(GenBank accession number, HBV genotype, and country of origin are indicated) and
Wooly Monkey HBV (AF046996) was used as the out group.
56
Discussion
To our knowledge, this is the first study to investigate the epidemiological and
virological aspects of HBV infection in MSM in Brazil using RDS as a recruitment and
data analysis method. The sociodemographic characteristics of the studied population
were similar to previous reports for Brazilian MSM, such as age under 25 years old [15],
self-identification as brown [31], single status [31], high school attended, and lowest tier
of Brazilian social class [15,32]. Although these characteristics were similar to those
reported previously, they can also be influenced by RDS. This recruitment method of
participants depends on a connected social network, and like other sampling methods for
hidden populations, there are tradeoffs [25,33].
The prevalence of HBV infection (15.4%; 95% CI: 8.7-25.8) estimated in this
study was similar to those found in MSM in Argentina (22.9%; 95% CI: 19.9-26.9) [34],
Australia (10.6%; 95% CI: 10.0-11.4) [35], and the USA (19.4%; 95% CI: 15.0-24.0)
[36]. These are countries with a low endemicity for this infection, similar to that reported
in Brazil [37]. This prevalence was also similar to that obtained in another recent study
among MSM in Brazil (Campinas City, São Paulo State: 11.4%; 95% CI: 7.8-14.9) [15].
Nevertheless, the prevalence determined in this study was higher than that observed in
the general population in Central Brazil (5.3%; 95% CI: 4.6-6.1) [38], suggesting that
MSM still have a greater vulnerability to HBV acquisition.
Moreover, the prevalence of anti-HBs alone showed that about 40% of the
population had serological evidence of immunization against HBV. In addition, a high
percentage (44.3%) of MSM was seronegative for all hepatitis B serological markers,
indicating susceptibility to HBV infection. These data suggest lower vaccination
coverage than desired, since the HBV vaccine is recommended and available free to all
MSM in Brazil. Therefore, it is important to emphasize the need to reassess and improve
57
strategies for prevention and control of hepatitis B in this group, mainly to increase the
number of MSM vaccinated against HBV.
As described by other authors [14,36,39], multivariate analysis shows that age
over 25 years old was independently associated with HBV infection in this study. The
association between HBV infection and older age has been widely reported and it is
probably due to the increased risk of exposure over time and also to the greater
vaccination coverage especially among children and young people in the last decades
[36,40].
Receptive anal intercourse and history of STIs were factors associated with HBV
infection in this population, as well as in other MSM [14,39]. Indeed, mucosal lesions
caused by anal sex have been associated with transmission of several STIs [41].
Additionally, sex with women was associated with HBV infection in this study. Although
most participants have self-identified as gay, almost half (47%) reported previous sex
with women. Studies indicate that men who have sex with both genders are a potential
bridge for STIs between MSM and women [34]. A previous study conducted among
Brazilian MSM has suggested that bisexual men who have practiced unprotected vaginal
and anal sex with their female partners as well as unprotected anal intercourse with their
male partners probably have an increased risk for HIV exposure and, consequently, for
other STIs [23].
HBV DNA was found in all HBsAg-positive MSM, showing that they have active
hepatitis B and a higher potential for HBV transmission. Additionally, this risk is directly
related to the level of HBV DNA in serum, and it is usually higher in those HBeAgpositive patients [41,42].
Despite the importance of researching occult HBV infection due to the risk of
progression to serious liver disease and potential transmission of HBV [2], there is only
58
one study concerning to OBI in MSM in the world, showing an OBI prevalence of 0.2%
in HIV-positive individuals in Germany [41]. Reflecting this low prevalence, OBI was
not observed in MSM analyzed in this study.
Phylogenetic analysis showed that HBV genotype A (A1 and A2) was identified
in the study population, corroborating previous studies which have indicated that this
genotype is the most prevalent in Brazil [7,38]. In addition, all HBV isolates analyzed
here presented the T131N substitution in the S gene. It has been suggested that this
mutation is a natural polymorphism in HBV genotypes A and G, being associated with
persistence of the HBV even after loss of HBsAg and anti-HBs seroconversion as well as
with vaccine escape [43].
The typical double mutation in BCP (A1762T and G1764A) found in one HBeAgnegative individual (Y431) is responsible for decreased HBeAg expression and has been
linked to HBV oncogenesis [9]. In this study, the Pre-C G1862T mutation was found in
one HBeAg-negative (Y513) and in one HBeAg-positive (Y494) participant (along with
G1888A), both belonging to subgenotype A1. As reported elsewhere [9,44], the presence
of G1862T in some HBeAg-positive patients suggests that this mutation can be genotype
specific, since it was predominantly found in HBV/A1 isolates. G1888A is also
characteristic of subgenotype A1 [45]. These findings indicate that HBV
genotypes/subgenotypes may display different clinical implications on the variability of
BCP, Pre-C/C and S gene regions and may impact hepatitis B prognosis.
These results must be considered in the context of the study's limitations. First, as
this was a cross-sectional study, it could not establish the causality between associated
factors and HBV infection; therefore a longitudinal study is needed to explore these
factors among Brazilian MSM. Second, as interviews were conducted face-to-face, it is
possible that behavioral responses may be sensitive for some participants resulting in
59
information biases, although interviewers were trained to minimize these biases. Third,
RDS is a relatively recent method and has its own limitations regarding calculation of the
sample size and appropriate tools for data analysis, as well as definition of estimators
[46]. In this study, although we have considered a design effect of 2 to the sample size
calculation, as often recommended in the literature [26,33], and some findings on
multivariate associations were significant, CIs were wide due to the modest sample size.
Lastly, the incentive reward offered by the RDS may attract more low-income MSM to
participate in the study. In addition, this was also limited to MSM aged 18 years or older,
potentially limiting the representativeness of the studied sample. Despite these
limitations, RDS is an effective approach to access hidden populations such as MSM.
Additionally, this study provided a comprehensive investigation of the epidemiological
and virological characteristics of HBV in a group of MSM in Brazil. Therefore, further
national study is necessary to confirm our findings.
In conclusion, this study shows that the HBV prevalence among MSM was higher
than that previously reported in the general population in Central Brazil, and was
associated with sexual risk behaviors. The large proportion of the study population
showed susceptibility to HBV infection, highlighting the need to increase HBV
immunization coverage in MSM, as well as the sexual health education programs in
Brazil. It is also worth mentioning the need for expert assistance and monitoring of HBV
DNA-positive individuals to prevent progression to more severe diseases.
Acknowledgements
The authors thank all MSM that participated in this study and the collaborators of
governmental and non-governmental organizations of LGBT (Lesbian, Gay, Bisexual and
Transgender) movement. Brian Ream provided English editing services.
60
References
1- World Health Organization (WHO). Hepatitis B. Fact sheet n°204. WHO, 2015.
Available: http://www.who.int/mediacentre/factsheets/fs204/en/. Accessed 11 Jan
2016.
2- Kwak MS, Kim YJ. Occult hepatitis B virus infection. World J Hepatol 2014;6(12):
860-869.
3- Pondé RA. Molecular mechanisms underlying HBsAg negativity in occult HBV
infection. Eur J Clin Microbiol Infect Dis. 2015;34(9): 1709-1731.
4- Kramvis A. Genotypes and genetic variability of hepatitis B virus. Intervirology.
2014;57(3-4): 141-150.
5- Pourkarim MR, Amini-Bavil-Olyaee S, Kurbanov F, Van Ranst M, Tacke F.
Molecular identification of hepatitis B virus genotypes/subgenotypes: revised
classification hurdles and updated resolutions. World J Gastroenterol. 2014;20(23):
7152-7168.
6- Lago BV, Mello FC, Kramvis A, Niel C, Gomes SA. Hepatitis B virus subgenotype
A1: evolutionary relationships between Brazilian, African and Asian isolates. PLoS
One, 2014;9(8): 1-9.
7- Mello FC, Souto FJ, Nabuco LC, Villela-Nogueira CA, Coelho HS, Franz HC et al.
Hepatitis B virus genotypes circulating in Brazil: molecular characterization of
genotype F isolates. BMC Microbiol. 2007;7: 103.
8- Gao S, Duan ZP, Coffin CS. Clinical relevance of hepatitis B virus variants. World
J Hepatol. 2015;7(8): 1086-1096.
9- Lazarevic I. Clinical implications of hepatitis B virus mutations: recent advances.
World J Gastroenterol. 2014;20(24): 7653-7664.
61
10- Centers for Disease Control and Prevention (CDC). Viral Hepatitis. Information for
Gay and Bisexual Men. CDC, 2013. Available: www.cdc.gov/hepatitis. Accessed 11
Jan 2016.
11- van Houdt R, Bruisten SM, Speksnijder AG, Prins M. Unexpectedly high proportion
of drug users and men having sex with men who develop chronic hepatitis B
infection. J Hepatol. 2012;57(3): 529-533.
12- Chow EP, Tucker JD, Wong FY, Nehl EJ, Wang Y, Zhuang X, et al. Disparities and
risks of sexually transmissible infections among men who have sex with men in
China: a meta-analysis and data synthesis. PLoS One. 2014;9(2): 1-13.
13- de Vries HJ. Sexually transmitted infections in men who have sex with men. Clin
Dermatol. 2014;32(2): 181-188.
14- Lama JR, Agurto HS, Guanira JV, Ganoza C, Casapia M, Ojeda N, et al. Hepatitis B
infection and association with other sexually transmitted infections among men who
have sex with men in Peru. Am J Trop Med Hyg. 2010;83(1): 194-200.
15- Soares CC, Georg I, Lampe E, Lewis L, Morgado MG, Nicol AF, et al. HIV-1, HBV,
HCV, HTLV, HPV-16/18, and Treponema pallidum infections in a sample of
Brazilian men who have sex with men. PLoS One. 2014;9(8):e102676. doi:
10.1371/journal.pone.0102676
16- Tseng YT, Sun HY, Chang SY, Wu CH, Liu WC, Wu PY, et al. Seroprevalence of
hepatitis virus infection in men who have sex with men aged 18-40 years in Taiwan.
J Formos Med Assoc. 2012;111(8): 431-438.
17- Urbanus AT, van Houdt R, van de Laar TJ, Coutinho RA. Viral hepatitis among men
who have sex with men, epidemiology and public health consequences. Euro
Surveill. 2009;14(47): 19421.
62
18- World Health Organization (WHO). Guidelines: Prevention and treatment of HIV
and other sexually transmitted infections among men who have sex with men and
transgender people. Recommendations for a public health approach. 2011.
19- Kassak K, Mahfoud Z, Kreidieh K, Shamra S, Afifi R, Ramia S. Hepatitis B virus
and hepatitis C virus infections among female sex workers and men who have sex
with men in Lebanon: prevalence, risk behaviour and immune status. Sex Health.
2011;8(2): 229-233.
20- Nyamathi A, Salem B, Reback CJ, Shoptaw S, Branson CM, Idemundia FE, et al.
Correlates of hepatitis B virus and HIV knowledge among gay and bisexual homeless
young adults in Hollywood. Am J Mens Health. 2013;7(1): 18-26.
21- Russi JC, Serra M, Viñoles J, Pérez MT, Ruchansky D, Alonso G, et al. Sexual
transmission of hepatitis B virus, hepatitis C virus, and human immunodeficiency
virus type 1 infections among male transvestite comercial sex workers in
Montevideo, Uruguay. Am J Trop Med Hyg. 2003;68(6): 716-720.
22- Sutmoller F, de Souza CT, Monteiro JC, et al. The Rio de Janeiro HIV vaccine siteII. Recruitment strategies and socio-demographic data of a HIV negative homosexual
and bisexual male cohort in Rio de Janeiro, Brazil. Mem Inst Oswaldo Cruz.
1997;92(1): 39-46.
23- Sutmoller F, Penna TL, de Souza CT, Lambert J. Human immunodeficiency virus
incidence and risk behavior in the 'Projeto Rio': results of the first 5 years of the Rio
de Janeiro open cohort of homosexual and bisexual men, 1994-98. Int J Infect Dis.
2002;6(4): 259-265.
24- Heckathorn DD. Respondent-Driven Sampling: A new approach to the study of
hidden populations. Social Problems. 1997;44: 174-199.
63
25- Kendall C, Kerr LR, Gondim RC, Werneck GL, Macena RH, Pontes MK, et al. An
empirical comparison of respondent-driven sampling, time location sampling, and
snowball sampling for behavioral surveillance in men who have sex with men,
Fortaleza, Brazil. AIDS Behav. 2008;12(Suppl 4): S97-104.
26- Salganik MJ. Variance estimation, design effects, and sample size calculations for
respondent-driven sampling. J Urban Health. 2006;83(Suppl 6): i98-112.
27- Niel C, Moraes MTB, Gaspar AMC, Yoshida CFT, Gomes AS. Genetic diversity of
hepatites B vírus strains isolated in Rio de Janeiro, Brazil. J Med Virol. 1994;44:
180-186.
28- Motta-Castro AR, Martins RM, Araujo NM, Niel C, Facholi GB, Lago BV, et al.
Molecular epidemiology of hepatits B virus in an isolated Afro-Brazilian community.
Arch Virol. 2008;153: 2197-2205.
29- Günther S, Li BC, Miska S, Krüger DH, Meisel H, Will H. A novel method for
efficient amplification of whole hepatitis B virus genomes permits rapid functional
analysis and reveals deletion mutants in immunosuppressed patients. J Virol.
1995;69(9): 5437-5444.
30- Brasil. Secretaria de Assuntos Estratégicos da Presidência da República do Brasil.
Assuntos estratégicos: Social e renda - A Classe Média Brasileira. Brasília, DF, 2014.
31- Sabidó M, Kerr LR, Mota RS, Benzaken AS, de A Pinho A, Guimaraes MD, et al.
Sexual violence against men who have sex with men in Brazil: A Respondent-Driven
Sampling Survey. AIDS Behav. 2015;19(9): 1630-1641.
32- Kerr LR, Mota RS, Kendall C, Pinho A de A, Mello MB, Guimarães MB, et al. HIV
among MSM in a large middle-income country. AIDS. 2013;27(3): 427-35.
64
33- Johnston LG, Hakim AJ, Dittrich S, Burnett J, Kim E, White RG. A Systematic
Review of Published Respondent-Driven Sampling Surveys Collecting Behavioral
and Biologic Data. AIDS Behav. 2016; DOI: 10.1007/s10461-016-1346-5.
34- Pando MA, Balán IC, Marone R, Dolezal C, Leu CS, Squiquera L, et al. HIV and
other sexually transmitted infections among men who have sex with men recruited
by RDS in Buenos Aires, Argentina: high HIV and HPV infection. PLoS One.
2012;7(6): e39834.
35- Gamagedara N, Weerakoon AP, Zou H, Fehler G, Chen MY, Read TR, et al. Crosssectional study of hepatitis B immunity in MSM between 2002 and 2012. Sex Transm
Infect. 2014;90(1): 41-45.
36- Pitasi MA, Bingham TA, Sey EK, Smith AJ, Teshale EH. Hepatitis B virus (HBV)
infection, immunity and susceptibility among men who have sex with men (MSM),
Los Angeles County, USA. AIDS Behav. 2014;18: 248-255.
37- Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide
prevalence of chronic hepatitis B virus infection: a systematic review of data
published between 1965 and 2013. Lancet, 2015;386(10003): 1546-1555.
38- Pereira LM, Martelli CM, Merchán-Hamann E, Montarroyos UR, Braga MC, de
Lima ML, et al. Population-based multicentric survey of hepatitis B infection and
risk factor differences among three regions in Brazil. Am J Trop Med Hyg.
2009;81(2): 240-247.
39- Linkins RW, Chonwattana W, Holtz TH, Wasinrapee P, Chaikummao S, Varangrat
A, et al. Hepatitis A and hepatitis B infection prevalence and associated risk factors
in men who have sex with men, Bangkok, 2006-2008. J Med Virol. 2013;85(9):
1499-505.
65
40- Souto FJ. Distribution of hepatitis B infection in Brazil: the epidemiological situation
at the beginning of the 21 st century. Rev Soc Bras Med Trop. 2016;49(1): 11-23.
41- Jansen K, Thamm M, Bock CT, Scheufele R, Kücherer C, Muenstermann D, et al.
High prevalence and high incidence of coinfection with hepatitis B, hepatitis C, and
syphilis and low rate of effective vaccination against hepatitis B in HIV-positive men
who have sex with men with known date of HIV seroconversion in Germany. PLoS
One. 2015;10(11): e0142515.
42- Shiffman ML. Management of cute hepatitis B. Clin Liver Dis. 2010;4: 75-91.
43- Svicher V, Cento V, Salpini R, Mercurio F, Fraune M, Beggel B, et al. Role of
hepatitis B virus genetic barrier in drug-resistance and immune-escape development.
Dig Liver Dis. 2011;43(12): 975-83.
44- Chandra PK, Banerjee A, Datta S, Chakravarty R. G1862T mutation among hepatitis
B virus-infected individuals: association with viral genotypes and disease outcome
in Kolkata, Eastern India. Intervirology. 2007;50(3): 173-180.
45- Kimbi GC, Kew MC, Kramvis A. The effect of the G1888A mutation of subgenotype
A1 of hepatitis B virus on the translation of the core protein. Virus Res. 2012;163(1):
334-340.
46- White RG, Lansky A, Goel S, Wilson D, Hladik W, Hakim A, et al. Respondent
driven sampling--where we are and where should we be going? Sex Transm Infect.
2012;88(6): 397-399.
66
Fig 1. Recruitment networks of 522 men who have sex with men in Goiânia, Central
Brazil. The seeds are indicated by large squares and recruits by small squares. Individuals
who had been exposed to HBV are in black and others in gray.
67
KJ854695 A1 Brazil
KJ854707 A1 Brazil
AY344109 A1 Brazil
Y 513
KJ854700 A1 Brazil
A1
Y 413
KJ854694 A1 Brazil
KJ854690 A1 Brazil
Y 494
Y 02
Y 431
KJ854710 A2 Brazil
A2
KJ854709 A2 Brazil
GU563554 A2 Belgium
GQ331048 A6 Belgium
FJ692609 A5 Haiti
AM180623 A4 Mali
AB194951 A3 Cameroon
FN545829 A7 Cameroon
FN545840 A7 Cameroon
FJ023664 I Laos
FJ023660 I Laos
AB064312 G United States
AB056515 G United States
AF282918 B China
AB104712 D1 Egypt
AB205126 D2 Japan
AY090452 D3 Spain
AB048702 D4 Australia
X75664 E Africa
AB091255 E Ivory Coast
V00867 C Japan
AB486012 J Japan
AY090459 F1 Costa Rica
JF815629 F2 Brazil
AB036915 F3 Venezuela
FJ657528 F4 Argentina
AY090457 H Nicaragua
AF046996 Woolly Monkey
68
Fig 2. Phylogenetic tree analysis of the S region of hepatitis B virus (HBV). The
phylogenetic tree performed by using the CLUSTAL W program and analyzed by Kimura
two-parameter methods. Genetic distances were calculated by the maximum composite
likelihood. Phylogenetic tree was constructed by the neighbor-joining method using
MEGA v.6.0 software (bootstrap resampling test with 1,000 replicates), including 5
isolates from Brazilian MSM (black square), 33 GenBank sequences of genotypes A–J
(GenBank accession number, HBV genotype, and country of origin are indicated) and
Wooly Monkey HBV (AF046996) was used as the out group.
69
4.2 Artigo 2
Hepatitis B vaccination and associated factors among men who have sex
with men in Brazil
70
ABSTRACT
Background: Despite the availability of the hepatitis B virus (HBV) vaccine for people
at high-risk of infection, such as men who have sex with men (MSM), a large proportion
of this population does not have evidence of protection against HBV infection. In Brazil,
there is no data regarding factors associated with hepatitis B immunization among MSM.
This study aims to assess the frequency of HBV vaccination and associated factors among
MSM in Brazil.
Methods: This is a cross-sectional study among MSM in Central Brazil. From March to
November 2014, 522 MSM were recruited using respondent-driven sampling (RDS). All
participants answered a questionnaire to gather sociodemographic data, behavioral
characteristics, and previous HBV vaccination information. Blood samples collected
were tested for HBV serological markers.
Results: The prevalence of serological evidence of hepatitis B vaccination (anti-HBs
alone) was 40.3%, while 76.2% self-reported receiving HBV vaccine. Nearly 15% had
serological marker of current or past infection (anti-HBc) and 44.3% remained
susceptible to HBV infection. A greater frequency of positivity for anti-HBs alone was
observed among MSM up to 25 years old, followed by declining vaccination rate with
increasing age. HBV vaccination was associated with unprotected anal intercourse (OR
= 2.40) and history of sexually transmitted infection (STI) (OR = 2.14, with a borderline
p-value). This study found a poor agreement (kappa = 0.17) between self-reported and
serologic evidence of HBV vaccination.
Conclusions: Strategies to increase HBV vaccine coverage among adults, especially the
older MSM group, must be improved. In addition, the need for a booster dose of HBV
vaccine should be better evaluated for people at high-risk of exposure to HBV such as
MSM.
71
KEYWORDS: hepatitis B; immunity; vaccination; associated factors; MSM.
1. INTRODUCTION
Hepatitis B represents a serious public health problem worldwide, and it is
responsible for cirrhosis, hepatocellular carcinoma, and high mortality rate. Strategies to
reduce the spread of hepatitis B virus (HBV) infection include the immunization of
susceptible individuals, treatment of chronic carriers, screening for HBV of all donated
blood, not sharing needles and syringes, and safer sex practices [1,2].
Vaccination against HBV is the most effective and safe strategy to prevent
infection among susceptible people. The complete vaccination schedule induces levels of
protective antibody (hepatitis B surface antibody, anti-HBs levels > 10 mIU/mL) in more
than 95% of vaccinated individuals. The HBV vaccine has been recommended by the
World Health Organization (WHO) for children, adolescents, and people in high-risk
groups of infection, including men who have sex with men (MSM), people with multiple
sexual partners, injection drug users, people interned in prisons, and health care workers
[2,3].
In a context of violence, social stigma, unsafe sexual practices and low access
to health services, MSM are considered at high-risk of sexually transmitted infections
(STIs), including hepatitis B [4,5]. Many studies have shown that this population has a
high prevalence of HBV infection and low immunization coverage against hepatitis B [68]. In recent years, HBV immunization rates in the group of MSM ranged from 9.2% in
Thailand [6] to 45.5% in the United States [9].
The low HBV vaccination coverage in MSM has been associated with sociodemographic characteristics, behavioral factors, social-cognitive factors and health
service access [8]. In Brazil, just one study conducted in the Southeast region has reported
72
a serological profile compatible with HBV vaccine response (anti-HBs alone) among
MSM [10]. Moreover, no data regarding factors associated with hepatitis B immunization
among Brazilian MSM have been published. Therefore, this study aims to assess the
frequency of HBV vaccination and associated factors among MSM in Central Brazil.
2. MATERIAL AND METHODS
This is a cross-sectional study in MSM in Goiânia (1,256,514 inhabitants),
the capital city of the State of Goiás, located in Central Brazil. From March to November
2014, a total of 522 participants were recruited using respondent-driven sampling (RDS),
a chain-referral sampling method useful to study hidden populations such as MSM, in
which participants recruit a limited number of additional participants [11]. The recruiting
methodology has been described elsewhere in further detail [12]. Individuals who agreed
to participate of the study signed a consent form and answered a structured questionnaire
to gather sociodemographic data, behavioral characteristics, and previous HBV
vaccination information. This study was approved by the Ethics Committee of the Federal
University of Goiás (UFG), Goiânia, Goiás, Brazil.
Blood specimens (10 mL) were collected from all participants, and serum
samples were tested by enzyme-linked immunosorbent assay (ELISA) for hepatitis B core
antibodies (anti-HBc) (Hepanostika anti-HBc Uni-form, BioMérieux, Marcy l’Étoile,
Lyon, France) and anti-HBs (titers were measured semi-quantitatively considering as
positive results levels ≥ 10 mIU/mL) (Bioelisa anti-HBs, Biokit, Barcelona, Spain). The
results of HBV serological tests were interpreted according to the CDC criteria [13]:
previous or ongoing HBV infection was defined by the presence of anti-HBc, immunity
to hepatitis B through vaccination was defined by the sole presence of anti-HBs, and
susceptibility to HBV infection was characterized as absence of any marker.
73
Data analysis was conducted using unweighted and weighted frequency
distribution estimates with 95% confidence intervals (CI). The respondent-driven
sampling analysis tool (RDSAT) v.5.6 was used to provide weights controlling for
selective recruitment bias and social network size [11]. The program SPSS v.20 (SPSS
Inc., IBM, Chicago, US) was used for analysis of variables associated with HBV
vaccination, using Pearson’s chi-square test and Fisher’s exact test. P-values less than
0.05 were considered statistically significant. Additionally, sensitivity, specificity,
positive predictive value (PPV), and negative predictive value (NPV) were calculated by
comparing the self-reported of HBV vaccination to the results of serological tests as the
“gold standard” (individuals who did not report HBV vaccination were excluded, n = 82;
of these, 21 were anti-HBs positive). The agreement using the kappa (k) coefficient was
calculated, and maximum value of 1.0 indicates perfect agreement.
3. RESULTS
Of a total of 522 MSM, 206 (39.5%; 40.3%, 95% CI: 32.3-48.8 after weighted
by RDSAT) had serological evidence of hepatitis B vaccination (anti-HBs), and 327
(62.6%; 76.2%, 95% CI: 68.1-82.8 weighted by RDSAT) self-reported receiving HBV
vaccine. In addition, 77 (14.8%; 15.4%, 95% CI: 8.7-25.8 weighted by RDSAT) had a
profile of previous or ongoing HBV infection. The prevalence rates of anti-HBs alone,
self-reported HBV vaccination, and HBV infection marker (anti-HBc) in different age
groups are shown in Figure 1. The highest prevalence for anti-HBs occurred in the age
group of 21 to 25 years old. Thereafter, there was a decrease in the positivity of this
marker with increasing age. Regarding self-reported HBV vaccination, there was an
increase in prevalence up to 30 years old, followed by a decline in the older MSM group.
By contrast, an increase of anti-HBc positivity with increasing age was observed.
74
Of 206 MSM who had serological evidence of HBV vaccination, 156 (75.7%)
self-reported receiving HBV vaccine. Anti-HBs seropositivity was found among 60.6%
(74/122) who reported receiving 3 or more HBV vaccine doses, 35.8% (38/106) who
reported fewer than 3 doses, and 44.4% (44/99) of those who reported an unknown
number of doses. Overall, of 327 participants who reported having been vaccinated in the
past, 47.7% (n = 156) were anti-HBs positive (Figure 2). In addition, 13.1% (43/327) had
evidence of past infection (anti-HBc positive), and 39.1% (128/327) were susceptible to
HBV infection. Moreover, 239/522 (45.8%; 44.3% after weighted by RDSAT) of studied
MSM were susceptible to HBV infection. Overall, the measure of self-reported hepatitis
B vaccination (regardless of the number of doses) had a sensitivity of 84.3% (95% CI:
78.1-89.1) and specificity of 32.4% (95% CI: 27.3-39.1) when compared against the
results of serological tests (anti-HBs). This corresponds to PPV of 47.7% (95% CI: 42.253.3), NPV of 74.34% (95% CI: 65.1-81.9), and kappa coefficient of 0.17.
Analysis of sociodemographic and behavioral characteristics among nonHBV infected MSM (Table 1) showed that only the variable irregular condom use at anal
intercourse has been statistically associated with HBV vaccination (OR = 2.40; 95% CI:
1.19-4.48). The other associated variable was history of STI (OR = 2.14; 95% CI: 0.865.36, with a borderline p-value).
4. DISCUSSION
Despite the availability of hepatitis B vaccine since 1998 for all newborns in
Brazil and the gradual expansion of vaccination availability for adolescents and adults, in
addition to the recommendation of HBV vaccine for people at high-risk of infection, such
as MSM [15,16], the findings of this study showed that after being weighted by RDSAT,
just 40.3% of the study population had serological evidence of HBV vaccination and
75
44.3% remained susceptible to HBV infection. These results were similar to those
observed in other recent studies among MSM [9,10,17], indicating that a large proportion
of this population did not have evidence of protection against HBV infection.
As expected, a greater frequency of anti-HBs was observed among the MSM
up to 25 years old. Although this estimate cannot be statistically compared, the association
between younger age and HBV vaccination was reported in other studies conducted
among MSM [8,9]. The presentation of greater rate of HBV vaccination among younger
groups with a subsequent decline with increasing age, accompanied by a contrast with an
increase in HBV infection marker, may reflect the expansion of HBV vaccine coverage,
mainly among children and adolescents, in the last decades, and a consequent decrease in
infection rates in younger groups [16]. In this way, it shows that the focus should be on
improving public health strategies to increase HBV vaccine coverage among adults,
especially older MSM group.
As reported elsewhere [8,17,18], HBV vaccination was associated with
unprotected anal intercourse and history of STI (with a borderline p-value), providing
evidence that MSM with high-risk behaviors are more likely to be vaccinated. Probably,
they have been vaccinated against hepatitis B due having accessed health care services to
diagnose and treat STI [17].
The results of this study showed poor agreement (k = 0.17) when comparing
the self-reported and serologic evidence of HBV vaccination. Based on the results of
serological testing, the self-report measure had moderate ability to detect true positives
(sensitivity of 84.3%) and low power to detect true negatives (specificity of 32.4%).
These findings suggest that evaluating vaccine status based on self-reports in the absence
of serological testing could result in misclassifications. Among MSM who reported being
vaccinated, only 47.7% (PPV) had serological evidence of vaccination. On the other hand,
76
among MSM who self-reported being unvaccinated, 74.3% (NPV) did not have this
serological evidence.
Self-reporting may have generated different forms of misclassification. First,
the participant’s vaccination record was not checked to verify the administration of the
number of doses of the HBV vaccine. Second, 13.1% of those who reported vaccination
had evidence of past infection, which may reflect the administration of vaccine to
individuals who were already infected. Third, less than 40% (122/327) of those who selfreported previous vaccination declared that they had completed the vaccination schedule
with 3 doses, therefore, it is expected that a considerable part of those who were partially
vaccinated have not developed an immune response.
Furthermore, the hepatitis B vaccination rate may be underestimated, since
anti-HBs levels decrease over time and may reach undetectable levels. In line with this,
some studies conducted in immunocompetent persons who have completed their
vaccination course properly have shown that the protective effects of HBV vaccination
remain even as anti-HBs levels become undetectable. Therefore, there is no indication for
a booster dose in immunocompetent individuals who have completed the full course of
vaccination [1,3,19,20]. However, a study in Taiwan has reported chronic hepatitis B in
adolescents who had received primary infant immunization, and indicates that some
people who received the HBV vaccine 15 years ago or more may have low or no
immunological memory against the virus, being susceptible to HBV infection [21].
Although WHO does not recommend booster vaccination in routine immunization
programs against hepatitis B [2], the need for a booster dose should be better studied
mainly for people in high-risk groups of exposure to HBV such as MSM.
In conclusion, our data show that despite the free availability of the hepatitis
B vaccine, it is noted that there was a large proportion of MSM who did not have
77
serological evidence of protection from HBV infection. Vaccination for adult MSM needs
to be encouraged and new strategies should be developed to increase the immunization
coverage in this population. In addition, further studies are required to elucidate the need
to implement the booster dose of the HBV vaccine after anti-HBs levels become
undetectable.
AUTHOR CONTRIBUTIONS
Design of the study: Martins RMB, Oliveira MP, Lopes CLR, Matos MAD.
Acquisition of data: Martins RMB, Oliveira MP, Lopes CLR, Silva AMC, Andrade AA,
Santana EBR, Freitas NR, Matos MAD.
Analysis and interpretation of data: Mota RMS, Martins RMB, Oliveira MP.
Drafting of manuscript: Oliveira MP, Martins RMB.
All authors read and approved the final manuscript.
COMPETING INTERESTS
None declared.
ETHICAL APPROVAL
This study were approved by the Ethics Committee of the Federal University of Goiás
(UFG), Goiânia, Goiás, Brazil.
ACKNOWLEDGEMENTS
78
This study was supported by the Brazilian Ministry of Health/Secretariat of Health
Surveillance/Department of STD, Aids and Viral Hepatitis through the Project of
International Technical Cooperation BRAK57 between the Brazilian Government and the
United Nations Office on Drugs and Crime-UNODC. The authors would like to thank all
MSM that participated in this study and the collaborators of governmental and nongovernmental organizations of LGBT (Lesbian, Gay, Bisexual and Transgender)
movement. We also thank Brian Ream for English language review.
5. REFERENCES
[1] Trépo C, Chan Hl, Lok A. Hepatitis B virus infection. Lancet 2014;384(9959):205363.
[2]
WHO
(World
Health
Organization).
Hepatitis
B.
Fact
sheet
n°204,
http://www.who.int/mediacentre/factsheets/fs204/en/; 2015 [accessed 06.05.16].
[3] Said ZN, Abdelwahab KS. Induced immunity against hepatitis B virus. World J
Hepatol 2015;7(12):1660-70.
[4] Lama JR, Agurto HS, Guanira JV, Ganoza C, Casapia M, Ojeda N, et al. Hepatitis B
infection and association with other sexually transmitted infections among men who
have sex with men in Peru. Am J Trop Med Hyg 2010;83(1):194-200.
[5] De Vries HJ. Sexually transmitted infections in men who have sex with men. Clin
Dermatol 2014;32(2):181-8.
[6] Linkins RW, Chonwattana W, Holtz TH, Wasinrapee P, Chaikummao S, Varangrat
A, et al. Hepatitis A and hepatitis B infection prevalence and associated risk factors
in men who have sex with men, Bangkok, 2006-2008. J Med Virol 2013;85(9):1499505.
79
[7] Chow EP, Tucker JD, Wong FY, Nehl EJ, Wang Y, Zhuang X, et al. Disparities and
risks of sexually transmissible infections among men who have sex with men in
China: a meta-analysis and data synthesis. PLoS One 2014;9(2):e89959.
[8] Vet R, de Wit JB, Das E. Factors associated with hepatitis B vaccination among men
who have sex with men: a systematic review of published research. Int J STD AIDS
2015;1-9.
[9] Pitasi MA, Bingham TA, Sey EK, Smith AJ, Teshale EH. Hepatitis B virus (HBV)
infection, immunity and susceptibility among men who have sex with men (MSM),
Los Angeles County, USA. AIDS Behav 2014;18:248-55.
[10] Soares CC, Georg I, Lampe E, Lewis L, Morgado MG, Nicol AF, et al. HIV-1, HBV,
HCV, HTLV, HPV-16/18, and Treponema pallidum infections in a sample of
Brazilian men who have sex with men. PLoS One 2014;9(8):e102676.
[11] Heckathorn DD. Respondent-driven sampling: a new approach to the study of hidden
populations. Social Problems 1997;44:174-99.
[12] Oliveira MP, Matos MA, Silva ÁM, Lopes CL, Teles SA, Matos MA, et al.
Prevalence, Risk Behaviors, and Virological Characteristics of Hepatitis B Virus
Infection in a Group of Men Who Have Sex with Men in Brazil: Results from a
Respondent-Driven Sampling Survey. PLoS One 2016;11(8):e0160916.
[13] CDC (Centers for Disease Control and Prevention). NC Hepatitis B Public Health
Program Manual/Hepatitis B Serology. Interpretation of Hepatitis B Serology,
http://www.cdc.gov/;2012; [accessed 07.06.16].
[14] Brasil. Secretaria de Assuntos Estratégicos da Presidência da República do Brasil.
Assuntos estratégicos: Social e renda - A Classe Média Brasileira. Brasília, DF, 2014.
[15] Brasil. Ministério da Saúde. Fundação Nacional de Saúde. Manual de Procedimentos
para Vacinação. Brasília-DF, 2001.
80
[16] Souto FJ. Distribution of hepatitis B infection in Brazil: the epidemiological situation
at the beginning of the 21 st century. Rev Soc Bras Med Trop 2016;49(1):11-23.
[17] Wang C, Wang Y, Huang X, Li X, Zhang T, Song M, et al. Prevalence and factors
associated with hepatitis B immunization and infection among men who have sex
with men in Beijing, China. PLoS One 2012;7(10):e48219.
[18] Storholm ED, Fisher DG, Reynolds GL, Napper LE, Morrisse TA, Kochems LM.
Hepatitis vaccination of men who have sex with men at gay pride events. Prev Sci
2010;11(2):219-27.
[19] McMahon BJ, Dentinger CM, Bruden D, Zanis C, Peters H, Hurlburt D, et al.
Antibody levels and protection after hepatitis B vaccine: results of a 22-year followup study and response to a booster dose. J Infect Dis 2009;200(9):1390-6.
[20] Wasley A, Kruszon-Moran D, Kuhnert W, Simard EP, Finelli L, McQuillan G, et al.
The prevalence of hepatitis B virus infection in the United States in the era of
vaccination. J Infect Dis 2010;202(2):192-201.
[21] Wu TW, Lin HH, Wang LY. Chronic hepatitis B infection in adolescents who
received primary infantile vaccination. Hepatology 2013;57(1):37-45.
81
Figure 1 - Prevalence of self-reported receiving hepatitis B virus (HBV) vaccine,
serological evidence of hepatitis B vaccination (anti-HBs alone), and HBV infection
(anti-HBc) among men who have sex with men in Brazil according to age group.
82
Figure 2 - Venn diagram representing the intersection between the men who have sex
with men with serological evidence of hepatitis B virus (HBV) vaccination and those selfreported receiving HBV vaccine.
83
Table 1 - Sociodemographic and behavioral characteristics associated with hepatitis B vaccination among
non-HBV infected men who have sex with men (MSM) in Brazil (N=445)
Variables
Anti-HBs Pos./
non-HBV infect.
Age (years)
18-20
21-25
26-30
31
Self-identification
Gay
Bisexual
Transvestite
Skin color/race
Brown (pardo)
White
Black
Yellow (Asian)/
Indigenous
Marital status
Single
Married/in stable
relationship
Education (years)
≤9
10 - 12
≥ 13
Social class (Brazilian
criteria)a
A/B/C (≥ R$ 2,005)
D (R$ 1,255-2,004)
E (≤ R$ 1,254)
Number of sexual partners
in lifetime
≤ 10
> 10
Ever received payment for sex
No
Yes
Receptive anal intercourse
No
Yes
Condom use at anal
intercourse
Always
Not Always
STIs
No
Yes
HIV status
Negative
Positive
Ever used any illicit drug
No
Yes
Blood transfusion lifetime
No
Yes
Health care access
No
Yes, public
Yes, private
Yes, public and private
Unweighted
%
Weighted %
(95% CI)
OR (95% CI)
p
75/167
80/149
32/74
19/55
44.9
53.7
43.2
34.5
50.3 (36.0-64.5)
53.4 (39.0-67.2)
45.7 (30.0-62.3)
31.9 (13.1-59.4)
2.15 (0.60-7.75)
2.44 (0.68-8.77)
1.79 (0.48-6.74)
1.00
0.432
148/306
28/65
30/74
48.4
43.1
40.5
49.1 (39.4-58.8)
45.3 (25.7-66.5)
36.7 (21.0-55.8)
1.66 (0.69-3.98)
1.43 (0.44-4.61)
1.00
0.664
114/256
44/86
34/75
15/28
44.5
51.2
45.3
53.6
49.5 (38.2-60.8)
46.3 (28.9-64.5)
48.5 (31.6-65.7)
28.4 ( 9.8-59.1)
2.47 (0.63-9.72)
2.17 (0.49-9.65)
2.37 (0.54-10.36)
1.00
0.662
161/369
45/80
43.6
56.2
45.8 (36.4-55.5)
57.0 (38.1-74.0)
1.00
1.57 (0.66-3.70)
0.302
17/58
126/271
62/114
29.3
46.5
54.4
25.3 (11.3-47.2)
49.8 (38.8-60.9)
51.3 (36.7-65.6)
1.00
2.94 (0.99-8.60)
3.11 (0.99-9.76)
0.116
35/67
52/116
119/262
52.2
44.8
45.4
39.8 (21.6-61.2)
46.9 (30.3-64.2)
49.0 (38.5-59.6)
1.00
1.34 (0.43-4.12)
1.46 (0.55-3.85)
0.781
63/140
142/304
45.0
46.7
43.0 (30.6-56.4)
50.8 (39.7-61.9)
1.00
1.37 (0.68-2.76)
0.379
108/236
96/207
45.8
46.4
45.1 (35.0-55.6)
50.8 (36.2-65.3)
1.00
1.26 (0.60-2.62)
0.538
31/77
174/367
40.3
47.4
39.6 (22.4-59.8)
50.4 (41.2-59.6)
1.00
1.55 (0.63-3.82)
0.335
95/222
108/220
42.8
49.1
37.7 (27.4-49.4)
59.2 (46.4-70.9)
1.00
2.40 (1.19-4.84)
0.014
156/344
46/95
45.3
48.4
42.7 (34.1-51.6)
61.5 (40.8-78.7)
1.00
2.14 (0.86-5.36)
0.099
170/362
36/83
47.0
43.4
48.6 (39.4-57.9)
41.4 (22.7-62.9)
1.34 (0.52-3.48)
1.000
0.543
120/238
86/206
50.4
41.7
47.0 (36.7-57.6)
49.4 (36.5-62.4)
1.00
1.10 (0.56-2.17)
0.784
197/421
8/19
46.8
42.1
47.7 (39.1-56.5)
49.4 (14.4-85.0)
1.00
1.07 (0.18-6.42)
0.942
23/60
79/183
52/107
52/95
38.3
43.2
48.6
54.7
47.8 (24.2-72.3)
49.0 (36.2-61.9)
42.0 (25.9-60.0)
52.0 (35.0-68.6)
1.26 (0.35-4.54)
1.33 (0.54-3.26)
1.00
1.50 (0.55-4.12)
0.885
MSM, men who have sex with men; CI, confidence interval; OR, odds ratio; STIs, sexually transmitted infections; HIV, human
immunodeficiency virus; R$, Brazilian real.
aBrazilian criteria to classify individuals into five economic classes [14]: “A” constitutes the highest tier of social class, while “E” the
lowest one (US$ 1.00 is approximately equal to R$ 2.32).
84
5 DISCUSSÃO
A presente tese representa o primeiro estudo com o intuito de investigar os
aspectos epidemiológicos e virológicos da hepatite B em homens que fazem sexo com
homens no Brasil, utilizando o RDS como método de recrutamento. Nesse sentido, esta
foi composta por dois artigos científicos. O primeiro com foco na prevalência e fatores
associados à infecção pelo HBV em HSH, e nas características genotípicas e mutações
presentes nos isolados virais (OLIVEIRA et al., 2016b). Complementarmente, o segundo
artigo abordou aspectos relacionados à vacinação contra hepatite B na população
estudada.
As características sociodemográficas da população estudada foram
semelhantes às reportadas em outros estudos em HSH no Brasil. A maioria dos
participantes tinha idade inferior a 25 anos, caracterizando a população como
predominantemente jovem, resultado concordante aos verificados nos estudos realizados
nas cidades de Campinas-SP (SOARES et al., 2014) e Campo Grande (FERNANDES et
al., 2015), bem como em sete das 10 cidades incluídas no estudo multicêntrico no Brasil
(KERR et al., 2013). Em relação à cor da pele, houve predominância de indivíduos
pardos, assim como relatado em outras investigações brasileiras (BRIGNOL et al., 2016;
GONÇALVES et al., 2016; KERR et al., 2013; SABIDÓ et al., 2015). A maior parte dos
participantes se auto declarou gay e solteira, características também observadas por outros
autores (SABIDÓ et al., 2015; VERAS et al., 2014; VOLK et al., 2016). Nível médio de
escolaridade (10 a 12 anos de estudo) foi mais frequente entre os HSH entrevistados, dado
similar ao descrito por Fernandes et al. (2015) e Brito et al. (2015). Por fim, grande parte
dos participantes deste estudo pertencia ao nível mais baixo de classe social, assim como
os HSH nas cidades do Rio de Janeiro, Santos e Curitiba (KERR et al., 2013).
A prevalência global da infecção pelo HBV de 15,4% (IC 95%: 8,7-25,8)
estimada no presente estudo foi semelhante à obtida (11,4%; IC 95%: 7,8-14,9) por
Soares et al. (2014). Ainda, foi próxima às encontradas em HSH de outros países com
baixa endemicidade para o HBV, como Argentina (22,9%; IC 95%: 19,9-26,9) (PANDO
et al., 2012), Estados Unidos (19,4%; IC 95%: 15,0-24,0) (PITASI et al., 2014) e
Austrália (10,6%; IC 95%: 10,0-11,4) (GAMAGEDARA et al., 2014). Considerando o
estudo de base populacional nas capitais da Região Centro-Oeste (PEREIRA et al., 2009),
a prevalência observada nesta tese foi superior à verificada (5,3%; IC 95%: 4,6-6,1) na
85
população geral da nossa região, sugerindo que os HSH apresentam maior
vulnerabilidade à infecção pelo HBV.
Após análise multivariada, idade acima de 25 anos foi independentemente
associada à infecção pelo HBV. Esta associação tem sido amplamente relatada em HSH
(LAMA et al., 2010; LINKINS et al., 2013; PITASI et al., 2014), e pode ser devido ao
aumento do risco de exposição ao vírus ao longo da vida, principalmente pela via sexual
(LINKINS et al., 2013; PITASI et al., 2014). Nesse contexto, sexo anal receptivo e
histórico de IST foram fatores associados à hepatite B nesta população, assim como em
outros HSH (GORGOS, 2013; LAMA et al., 2010; LINKINS et al., 2013). De fato, lesões
na mucosa anorretal causadas pela prática do sexo anal podem propiciar a transmissão de
várias IST (JANSEN et al., 2015). Adicionalmente, sexo com mulheres foi associado à
infecção pelo HBV neste estudo. Pesquisas indicam que os homens que têm relações
sexuais com ambos os sexos são uma potencial ponte para IST entre HSH e mulheres
(JEFFRIES, 2014; PANDO et al., 2012).
O marcador HBsAg foi identificado em 0,6% (IC 95%: 0,2-1,6) dos
participantes. Após a realização dos testes moleculares, o HBV DNA foi detectado em
todos os HSH HBsAg positivos, mostrando que esses são portadores de hepatite B ativa
e apresentam um maior potencial de transmissão do vírus (JANSEN et al., 2015;
SHIFFMAN, 2010). A análise filogenética revelou a presença do genótipo A
(subgenótipos A1 e A2) do HBV na população estudada, o que corrobora a predominância
desse genótipo no Brasil (MELLO et al., 2007; PEREIRA et al., 2009).
Apesar da importância da pesquisa de infecção oculta pelo HBV devido ao
risco de progressão para doença hepática grave e potencial transmissão viral (KWAK;
KIM, 2014), existe apenas um estudo em HSH referente ao tema em questão. Nesse,
Jansen et al. (2015) estimaram uma prevalência de 0,2% para infecção oculta pelo HBV
em portadores do HIV na Alemanha. Corroborando essa baixa prevalência, tal infecção
não foi observada nos HSH participantes deste estudo.
Ao analisar as sequências de nucleotídeos das amostras HBV DNA positivas,
notou-se que todos os isolados apresentavam a substituição de T131N no gene S. Essa
mutação tem sido sugerida como um polimorfismo natural nos genótipos A e G do HBV,
estando associada à persistência do HBV no organismo mesmo após negativar o HBsAg
e ocorrer a soroconversão para anti-HBs, bem como ao escape vacinal. Além disso, essa
substituição pode gerar um novo sítio de glicosilação propiciando a liberação do vírus,
principalmente na presença da mutação M133T/S (SVICHER et al., 2011). Tendo em
86
vista a importância dessa alteração genômica, o acompanhamento clínico desses
pacientes é importante pois são potenciais portadores da infecção oculta pelo HBV no
futuro. A típica dupla mutação na região BCP (A1762T e G1764A), encontrada em um
indivíduo HBeAg negativo, tem sido relacionada à diminuição da expressão do HBeAg
e à oncogênese do HBV (LAZAREVIC, 2014). Ainda, alterações nas regiões Pré-C/C
foram observadas em amostras de HSH participantes deste estudo, como as substituições
G1862T e G1888A características do subgenótipo A1 (CHANDRA et al., 2007; KIMBI;
KEW; KRAMVIS, 2012; LAZAREVIC, 2014). Esses achados indicam que os genótipos
e subgenótipos do HBV podem ter impacto no prognóstico da hepatite B.
Apesar da disponibilidade de vacina contra a hepatite B desde 1998 para todos
os recém-nascidos no Brasil e da expansão gradual da cobertura vacinal para adolescentes
e adultos, além da recomendação da vacina contra o HBV para pessoas com maior
vulnerabilidade à infecção, como HSH (BRASIL, 2001; SOUTO, 2016), nossos achados
mostraram que 40,3% da população do estudo apresentaram evidência sorológica de
vacinação contra o HBV e 44,3% eram suscetíveis à infecção. Estes resultados foram
semelhantes aos observados em outros estudos entre HSH (PITASI et al., 2014; SOARES
et al., 2014; WANG et al., 2012), indicando que uma grande proporção dessa população
não possui evidência sorológica de proteção contra a hepatite B.
Como esperado, uma maior frequência de anti-HBs isolado foi verificada
entre os HSH com até 25 anos de idade, seguida de seu declínio com o aumento da idade
e, em contraste, observou-se aumento da taxa de infecção pelo HBV. Tais dados podem
refletir a expansão da cobertura vacinal contra hepatite B, principalmente entre crianças
e adolescentes nas últimas décadas, e consequente diminuição do índice de infecção no
grupo mais jovem (SOUTO, 2016). Desta forma, há necessidade de aumentar a cobertura
vacinal contra o HBV entre os HSH adultos, especialmente aqueles com idade superior a
25 anos.
Como descrito por outros autores (STORHOLM et al., 2010; VET; DE WIT;
DAS, 2015), sexo anal desprotegido foi fator associado à vacinação contra o HBV no
presente estudo. Esse fato pode reafirmar a hipótese de que HSH com comportamentos
de risco são mais propensos à vacinação (STORHOLM et al., 2010). Adicionalmente,
neste estudo, história de IST mostrou-se marginalmente associada à imunização contra
hepatite B. Essa associação foi previamente relatada (VET; DE WIT; DAS, 2015, WANG
et al., 2012) e pode sugerir oportunidade de acesso à vacina contra o HBV ao buscar o
serviço de saúde para diagnóstico e tratamento de outras IST (WANG et al., 2012).
87
Semelhantemente ao mostrado em outros estudos (GILBERT et al., 2010;
WANG et al., 2012; YEE; RHODES, 2002), neste foi observada uma maior frequência
de vacinação contra o HBV entre HSH com maior nível de escolaridade. Essa
característica indica que programas de educação em saúde podem aumentar a
conscientização dessa população sobre a importância da vacinação contra hepatite B,
incentivando os HSH suscetíveis a receber o esquema de vacinação completo (GILBERT
et al., 2010; WANG et al., 2012).
Os resultados da presente investigação mostraram uma baixa concordância
(kappa = 0,17) entre o auto relato (76,2%) e a evidência sorológica (40,3%) de vacinação
contra hepatite B. Baseando-se na presença do marcador anti-HBs, o auto relato
apresentou moderada habilidade para detectar verdadeiros positivos (sensibilidade de
84,3%) e baixa capacidade de identificar verdadeiros negativos (especificidade de
32,4%). Dentre os 327 HSH que relataram vacinação prévia, apenas 156 (47,7%)
apresentaram evidência sorológica. Por outro lado, dos HSH que informaram não
vacinação, 74,3% (84/113) realmente não possuíam evidencia sorológica de imunização
prévia. Estes achados sugerem a possibilidade de erros na determinação do status vacinal
baseada apenas no auto relato.
Nesse contexto, diferentes falhas podem ter ocorrido ao considerar o auto
relato de vacinação. Primeiramente, não foi checado o cartão de vacinação para verificar
a veracidade da informação quanto à administração e o número de doses da vacina contra
o HBV. Em segundo lugar, cerca de 13% dos que relataram vacinação tinham evidência
sorológica de infecção passada pelo HBV, podendo refletir a administração da vacina
após a exposição ao vírus. Em terceiro lugar, menos de 40% dos que reportaram
vacinação prévia declararam ter completado o esquema vacinal com três doses. Portanto,
é esperado que parte dos que foram parcialmente vacinados não tenha desenvolvido uma
resposta imunológica adequada.
Além disso, a taxa de vacinação contra hepatite B baseada na evidência
sorológica pode ter sido subestimada, uma vez que os níveis de anti-HBs diminuem ao
longo do tempo e podem atingir níveis indetectáveis. Nesse sentido, alguns estudos
realizados em imunocompetentes que completaram o esquema vacinal mostraram que o
efeito protetor da vacina contra o HBV permanece mesmo após a queda do marcador antiHBs a valores indetectáveis. Assim sendo, não há indicação de dose de reforço para esses
indivíduos (MCMAHON et al., 2009; SAID; ABDELWAHAB, 2015; TREPO et al.,
2014; WASLEY et al., 2010). No entanto, um estudo realizado em Taiwan relatou casos
88
de hepatite B crônica em adolescentes que haviam recebido o esquema vacinal na
primeira infância, sugerindo que, após 15 anos ou mais da administração da vacina,
algumas pessoas podem apresentar baixa ou até mesmo nenhuma memória imunológica
contra o HBV, sendo suscetíveis à infecção (WU; LIN; WANG, 2013). Embora a dose
de reforço da vacina contra hepatite B não seja recomendada pela OMS nos programas
de imunização de rotina (WHO, 2015a), tal questão deve ser melhor estudada,
principalmente, em grupos de maior vulnerabilidade para infecção pelo HBV, como os
HSH.
Os resultados aqui apresentados devem ser considerados no contexto das
limitações do estudo. Primeiramente, por se tratar de um estudo transversal, não se pode
estabelecer uma relação de causalidade entre fatores associados e a infecção pelo HBV,
assim, seria necessário um estudo longitudinal para explorar esses fatores entre os HSH
brasileiros. Em segundo lugar, embora os entrevistadores tenham sido treinados para
minimizar vieses, como as entrevistas foram realizadas frente a frente com os
participantes, é possível que perguntas relacionadas a comportamentos de risco tenham
sido consideradas inconvenientes para alguns participantes, resultando em viés de
informação. Terceiro, o RDS é um método relativamente recente e tem suas próprias
limitações quanto ao cálculo do tamanho da amostra e ferramentas apropriadas para
análise de dados (WHITE et al., 2012). Neste estudo, foi considerado um efeito de
desenho de dois para o cálculo do tamanho da amostra, como recomendado na literatura
(JOHNSTON et al., 2016; SALGANIK, 2006) e, após análise multivariada, algumas
associações foram significativas, porém os intervalos de confiança foram amplos devido
ao tamanho modesto da amostra. Por fim, o incentivo oferecido pelo recrutamento
utilizando o RDS pode ter atraído mais HSH de baixa renda para participar do estudo.
Além disso, a população de estudo é limitada aos HSH com idade igual ou superior a 18
anos, diminuindo, assim, a representatividade da amostra estudada. Apesar dessas
limitações, o RDS é uma metodologia eficaz para recrutar populações de difícil acesso,
como HSH, produzindo uma amostra diversificada (KENDALL et al., 2008; WEI et al.,
2012).
Por fim, considerando os resultados obtidos nesta tese, recomendamos que os
portadores do HBV sejam monitorados quanto à progressão da doença, visto que nos
isolados virais foram identificadas mutações que podem ter impacto no prognóstico da
infecção. Do ponto de vista epidemiológico, a prevalência elevada da infecção pelo HBV
nos HSH associada a comportamentos sexuais de risco e, por outro lado, uma frequência
89
baixa de vacinação contra a hepatite B, evidencia a necessidade de políticas públicas
contínuas de saúde voltadas para a população-alvo, incluindo estratégias para aumentar a
cobertura vacinal contra o HBV. Além disso, estudos adicionais são necessários para
elucidar se há necessidade de implementar a dose reforço da vacina para grupos
vulneráveis, como HSH, após os níveis de anti-HBs se tornarem indetectáveis.
90
6 CONCLUSÕES
- A prevalência do marcador anti-HBc estimada nos HSH em Goiânia-Goiás foi de 15,4%,
e do HBsAg foi de 0,6%;
- A infecção pelo vírus da hepatite B em HSH foi associada à idade superior a 25 anos,
sexo anal receptivo, ter feito sexo com mulheres e histórico de IST;
- A infecção oculta pelo HBV não foi observada na população estudada;
- O genótipo A e os seus subgenótipos A1 e A2 foram identificados, corroborando a
circulação desses no Brasil;
- Mutações no genoma do HBV nas regiões S (T131N), BCP (A1762T/G1764A) e PréC/C (G1862T/G1888A e G1862T) foram detectadas;
- Verificou-se evidência sorológica de vacinação contra a hepatite B em 40,3% dos
indivíduos estudados, enquanto que 76,2% relataram ter recebido previamente essa
vacina;
- A imunização contra o HBV entre os HSH foi associada à pratica de sexo anal
desprotegido.
91
7 REFERÊNCIAS
AIRES, R. S. et al. Prevalence of hepatitis B virus infection among tuberculosis patients
with or without HIV in Goiânia City, Brazil. J Clin Virol, v. 54, n. 4, p. 327-331,
2012.
ALTER, M. J. et al. Hepatitis B virus transmission between heterosexuals. JAMA, v.
256, n. 10, p. 1307-1310, 1986.
ALTER, M. J. Epidemiology of hepatitis B in Europe and worldwide. J Hepatol, v. 39,
p. S64-69, 2003.
ALVARADO-MORA, M. V.; PINHO, J. R. Distribution of HBV genotypes in Latin
America. Antivir Ther, v. 18, p. 459-465, 2013.
ARAUJO, O. C. et al. Genetic variability of hepatitis B and C viruses in Brazilian patients
with and without hepatocellular carcinoma. J Med Virol, v. 86, n. 2, p. 217-223,
2014.
ARAUJO, N. M. et al. High proportion of subgroup A' (genotype A) among Brazilian
isolates of hepatitis B virus. Arch Virol, v. 149, n. 7, p. 1383-1395, 2004.
ARAUJO, N. M. et al. Identification of novel recombinants of hepatitis B virus genotypes
F and G in human immunodeficiency virus-positive patients from Argentina and
Brazil. J Gen Virol, v. 94, n. 1, p. 150-158, 2013.
ARAUJO, N. M.; WAIZBORT, R.; KAY, A. Hepatitis B virus infection from an
evolutionary point of view: how viral, host, and environmental factors shape
genotypes and subgenotypes. Infect Genet Evol, v. 11, n. 6, p. 1199-1207, 2011.
ARAUZ-RUIZ, P. et al. Genotype H: a new Amerindian genotype of hepatitis B virus
revealed in Central America. J Gen Virol, v. 83, p. 2059-2073, 2002.
ASPINALL, E. J. et al. Hepatitis B prevention, diagnosis, treatment and care: a review.
Occup Med (Lond), v. 61, p. 531-540, 2011.
ASSIS, D. R. et al. Characteristics of an outpatient chronic hepatitis B virus infection
cohort. Einstein (Sao Paulo), v. 13, n. 2, p. 189-195, 2015.
AZEVEDO, M. S. P. et al. Rastreamento sorológico para hepatite B em profissionais de
saúde na cidade de Goiânia - Goiás. Rev Soc Bras Med Trop, v. 27, n. 3, p. 15762, 1994.
BALAYAN, M. S. et al. Evidence for a virus in non-A, non-B hepatitis transmitted via
fecal-oral route. Intervirol, v. 20, p. 23-31, 1983.
92
BANCROFT, W. H.; MUNDON, F. K.; RUSSELL, P. K. Detection of additional
antigenic determinants of hepatitis B antigen. J Immunol, v. 109, p. 842-848,
1972.
BAQI, S. et al. Seroprevalence of HIV, HBV, and syphilis and associated risk behaviours
in male transvestites (Hijras) in Karachi, Pakistan. Int J STD AIDS, v. 10, n. 5,
p. 300-304, 1999.
BARROS, L. A. et al. Epidemiology of the viral hepatitis B and C in female prisoners of
Metropolitan Regional Prison Complex in the State of Goiás, Central Brazil. Rev
Soc Bras Med Trop, v. 46, n. 1, p. 24-29, 2013.
BASTOS, C. C. Estudo soroepidemioilógico para o vírus da hepatite B, hepatite C e
da imunodeficinêcia humana em pacientes com doenças falciformes. 2000.
79f. Dissertação (Mestrado). Instituto de Patologia Tropical e Saúde
Pública/Universidade Federal de Goiás (IPTSP/UFG), Goiânia, Goiás, 2000.
BAUMERT, T. F.; THIMME, R.; VON WEIZSÄCKER, F. Pathogenesis of hepatitis B
virus infection. World J Gastroenterol, v. 13, n. 1, p. 82-90, 2007.
BAUMERT, T. F. et al. Entry of hepatitis B and C viruses - recent progress and future
impact. Curr Opin Virol, v. 4, p. 58-65, 2014.
BECK, J.; NASSAL, M. Hepatitis B virus replication. World J Gastroenterol, v. 13, n.
1, p. 48-64, 2007.
BERTOLINI, D. A. et al. Hepatitis B virus genotypes from European origin explains the
high endemicity found in some areas from southern Brazil. Infect Genet Evol, v.
12, n. 6, p. 1295-1304, 2012.
BIERNACKI, P.; WALDORF, D. Snowball Sampling: Problems and Techniques of
Chain Referral Sampling. Sociol Methods Res, v. 10, n. 2, p. 141, 1981.
BLEEKER, A. et al. Prevalence of syphilis and hepatitis B among homosexual men in
two saunas in Amsterdam. Br J Vener Dis, v. 57, n. 3, p. 196-199, 1981.
BLUMBERG, B. S.; ALTEN, H. J.; VISNICH, S. A “new” antigen in leukemia sera.
JAMA, v. 191, p. 541-546, 1965.
BOND, W. W. et al. Survival of hepatitis B virus after drying and storage for 1 week.
Lancet, v. 1, p. 550-551, 1981.
BORGES, A. M. T. et al. Hepatite B em pacientes de centros de diálise de Goiânia –
Goiás. Rev Patol Trop, v. 26, n. 1, p. 9-16, 1997.
BOZICEVIC, I. et al. Prevalence of sexually transmitted infections among men who have
sex with men in Zagreb, Croatia. AIDS Behav, v. 13, n. 2, p. 303-309, 2009.
93
BRANDÃO, N. A. et al. Prevalence of hepatitis B and C infection and associated factors
in people living with HIV in Midwestern Brazil. Braz J Infect Dis, v. 19, n. 4, p.
426-430, 2015.
BRASIL. Ministério da Saúde. Fundação Nacional de Saúde. Manual de Procedimentos
para Vacinação. Brasília-DF, 2001.
BRASIL. Ministério da Saúde. Programa Nacional de Imunizações, 30 anos. Brasília,
DF, 2003.
BRASIL. Ministério da Saúde. Brasil Sem Homofobia. Programa de Combate à
Violência e à Discriminação contra GLTB e de Promoção da Cidadania
Homossexual. Brasília, DF, 2004.
BRASIL. Ministério da Saúde. Plano de enfrentamento da epidemia de Aids e das
DST entre população de Gays, HSH e Travestis. Brasília, DF, 2007.
BRASIL. Ministério da Saúde. Hepatites Virais: o Brasil está atento, 3ª edição.
Brasília, DF, 2008.
BRASIL. Ministério da Saúde. A B C D E das Hepatites Virais para Agentes
Comunitários de Saúde. Brasília, DF, 2009.
BRASIL. Ministério da Saúde. Estudo de prevalência de base populacional das
infecções pelos vírus das hepatites a, b e c nas capitais do Brasil. Brasília, DF,
2010a.
BRASIL. Ministério da Saúde. Parecer técnico nº 04/2010/CGPNI/DEVEP/SMS/MS e
AIDS e HEPATITES VIRAIS/SMS/MS “Atualização da indicação da vacina
hepatite B nos serviços de saúde”. 2010b.
BRASIL. Ministério da Saúde. Boletim Epidemiológico Hepatites Virais. Ano III, n. 1,
Brasília, DF, 2012.
BRASIL. Ministério da Saúde. Nota técnica conjunta nº 02/2013/CGPNI/DEVEP e
CGDHRV/DST-AIDS/SVS/MS. Ampliação da oferta da vacina hepatite B
para faixa etária de 30 a 49 anos em 2013. Brasília, DF, 2013.
BRASIL.
Ministério
da
Saúde.
Nota
informativa
nº
149,
de
2015/CGPNI/DEVIT/SVS/MS. Informa as mudanças para o calendário
nacional de vacinação para o ano de 2016. Brasília, DF, 2015.
BRASIL. Ministério da Saúde. Protocolo Clínico e Diretrizes Terapêuticas para
Hepatite B e Coinfecções. Brasília, DF, 2016.
94
BRIGNOL, S. et al. Vulnerability in the context of HIV and syphilis infection in a
population of men who have sex with men (MSM) in Salvador, Bahia State,
Brazil. Cad Saúde Pública, v. 31, n. 5, p. 1035-1048, 2015.
BRITO, A. M. et al. Factors Associated with Low Levels of HIV Testing among Men
Who Have Sex with Men (MSM) in Brazil. PLoS One, v. 10, n. 6, p. 1-13, 2015.
BURNS, G. S.; THOMPSON, A. J. Viral hepatitis B: clinical and epidemiological
characteristics. Cold Spring Harb Perspect Med, v. 4, n. 12, p. 1-14, 2014.
CAETANO, K. A. A. Epidemiologia da Infecção pelo Vírus da Hepatite B em
Assentados em Goiás: Subsídios para Ações de Prevenção e Controle em
Populações Emergentes. 2014. 99f. Tese (Doutorado). Ciências da Saúde da
Universidade Federal de Goiás. Goiânia, Goiás, 2014.
CARDOSO, D. D. P. et al. Soroprevalência para infecção pelo vírus da hepatite B pelos
marcadores AgHBs e anti-HBs em população feminina de área urbana de GoiâniaGo. Rev Patol Trop, v. 19, n. 2, p. 135-141, 1990.
CARDOSO, D. D. P. et al. Soroepidemiologia para o vírus da hepatite B (VHB) em
gestantes/parturientes e sua transmissão para recém-nascidos em Goiânia-GO.
Rev Soc Bras Med Trop, v. 29, n. 4, p. 349-53, 1996.
CARMAN, W. F. et al. Vaccine-induced escape mutant of hepatitis B virus. Lancet, v.
336, p. 325-329, 1990.
CARNEIRO, A. F.; DAHER, R. R. Soroprevalência do vírus e hepatite B em
anestesiologistas. Rev Bras Anestesiol, v. 53, n. 5, p. 672-679, 2003.
CARVALHO, P. M. R. S. Epidemiologia da hepatite B em indivíduos em situação de
rua abrigados em casa de passagem de Goiânia, Goiás. 2016. Dissertação
(mestrado). Programa de Pós-Graduação em Enfermagem da Faculdade de
Enfermagem da Universidade Federal de Goiás. Goiânia, Goiás, 2016.
CDC (Centers for Disease Control and Prevention) 2013. Viral Hepatitis. Information for
Gay and Bisexual Men. CDC. Disponível em: <www.cdc.gov/hepatitis>. Acesso
em: 11 de janeiro de 2016).
CDC (Centers for Disease Control and Prevention) 2015a. Lesbian, Gay, Bisexual, and
Transgender
Health.
Disponível
em:
<http://www.cdc.gov/lgbthealth/youth.htm>. Acesso em: 05 de junho de 2015.
CDC (Centers for Disease Control and Prevention) 2015b. Viral Hepatitis Serology
Training.
Disponível
em:
95
<http://www.cdc.gov/hepatitis/resources/professionals/training/serology/training
.htm>. Acesso em: 31 de agosto de 2016.
CHANDRA, P. K. et al. G1862T mutation among hepatitis B virus-infected individuals:
association with viral genotypes and disease outcome in Kolkata, Eastern India.
Intervirology, v. 50, n. 3, p. 173-180, 2007.
CHANG, M. H. Prevention of hepatitis B virus infection and liver cancer. Recent Results
Cancer Res, v. 193, p. 75-95, 2014.
CHEN, P. et al. Computational evolutionary analysis of the overlapped surface (S) and
polymerase (P) region in hepatitis B virus indicates the spacer domain in P is
crucial for survival. PLoS One, v. 8, n. 4, p. 1-9, 2013.
CHEVALIEZ, S.; PAWLOTSKY, J. M. Virological techniques for the diagnosis and
monitoring of hepatitis B and C. Ann Hepatol, v. 8, n. 1, p. 7-12, 2009.
CHOI, K. H. et al. High level of hepatitis B infection and ongoing risk among
Asian/Pacific Islander men who have sex with men, San Francisco, 2000-2001.
Sex Transm Dis, v. 32, n. 1, p. 44-48, 2005.
CHOO, Q. L. et al. Isolation of a clone derived from a blod-borne non-A, non-B viral
hepatitis genome. Science, v. 244, p. 359-362, 1989.
CHOW, E. P. et al. Disparities and risks of sexually transmissible infections among men
who have sex with men in China: a meta-analysis and data synthesis. PLoS One,
v. 9, n. 2, 2014.
COLÓN-LÓPEZ, V. et al. HIV-related risk behaviors among a sample of men who have
sex with men in Puerto Rico: an overview of substance use and sexual practices.
P R Health Sci J, v. 30, n. 2, p. 65-68, 2011.
COSTA, E. F. A. Análise da soroprevalência para as infecções pelos vírus das
hepatites B e C em idosos residentes em asilos no município de Goiânia. 2004.
106f. Dissertação (Mestrado). Programa de Pós-Graduação em Medicina
Tropical- IPTSP/UFG. Goiânia, Goiás, 2004.
COUROUCÉ-PAUTY, A. M.; PLANÇON, A.; SOULIER, J. P. Distribution of HBsAg
subtypes in the world. Vox Sang, v. 44, n. 4, p. 197-211, 1983.
CROAGH, C. M.; DESMOND, P. V.; BELL, S. J. Genotypes and viral variants in chronic
hepatitis B: A review of epidemiology and clinical relevance. World J Hepatol,
v. 7, n. 3, p. 289-303, 2015.
96
CROAGH, C. M.; LUBEL, J. S. Natural history of chronic hepatitis B: phases in a
complex relationship. World J Gastroenterol, v. 20, n. 30, p. 10395-10404,
2014.
CROSS, J. C.; WEN, P.; RUTTER, W. J. Transactivation by hepatitis B virus X protein
is promiscuous and dependent on mitogen-activated cellular serine/threonine
kinases. Proc Natl Acad Sci USA, v. 90, n. 17, p. 8078-8082, 1993.
DAMACENA, G. N.; SZWARCWALD, C. L.; BARBOSA JÚNIOR, A. Implementation
of respondent-driven sampling among female sex workers in Brazil, 2009. Cad
Saude Publica, v. 27, p. S45-55, 2011.
DANE, D. S.; CAMERON, C. H.; BRIGGS, M. Virus-like particles in serum of patients
with Australia-antigen-associated hepatitis. Lancet, v. 1, p. 695-698, 1970.
DASH, S. et al. Significance of natural polymerized albumin and its receptor on hepatitis
B infection of hepatocytes. Hepatol, v. 13, p. 134-142, 1991.
DATTA, S. et al. Genotype, phylogenetic analysis, and transmission pattern of occult
hepatitis B virus (HBV) infection in families of asymptomatic HBsAg carriers. J
Med Virol, v. 78, n. 1, p. 53-59, 2006.
DATTA, S.; CHATTERJEE, S.; VEER, V. Recent advances in molecular diagnostics of
hepatitis B virus. World J Gastroenterol, v. 20, n. 40, p. 14615-14625, 2014.
DE PAIVA, E. M. et al. Serological markers and risk factors related to hepatitis B virus
in dentists in the Central West region of Brazil. Braz J Microbiol, v. 39, n. 2, p.
251-256, 2008.
DE SOUZA, M. M. et al. Soroprevalência da infecção pelo vírus da hepatite B em
portadores de doença mental. Rev Bras Psiquiatr, v. 26, p. 35-38, 2004.
DE VRIES, H. J. Sexually transmitted infections in men who have sex with men. Clin
Dermatol, v. 32, n. 2, p. 181-188, 2014.
DÉNY, P.; ZOULIM, F. Hepatitis B virus: from diagnosis to treatment. Pathol Biol
(Paris), v. 58, n. 4, p. 245-253, 2010.
DEVI, U.; LOCARNINI, S. Hepatitis B antivirals and resistance. Curr Opin Virol, v. 3,
n. 5, p. 495-500, 2013.
DIAMOND, C. et al. Viral hepatitis among young men who have sex with men:
prevalence of infection, risk behaviors, and vaccination. Sex Transm Dis, v. 30,
n. 5, p. 425-432, 2003.
97
DIAS, A. L. et al. Molecular characterization of the hepatitis B virus in autochthonous
and endogenous populations in the Western Brazilian Amazon. Rev Soc Bras
Med Trop, v. 45, n. 1, p. 9-12, 2012.
DOO, C. E.; GHANY, G. M. Hepatitis B virology for clinicians. Clin Liver Dis, v. 14,
p. 397-408, 2010.
DOS ANJOS, G. R. L. C. et al. Epidemiology of hepatitis B virus infection in first-time
blood donors in the southwestern region of Goiás, central Brazil. Rev Bras
Hematol Hemoter, v. 33, n. 1, p. 38-42, 2011.
DOS RAMOS FARÍAS, M. S. et al. First report on sexually transmitted infections among
trans (male to female transvestites, transsexuals, or transgender) and male sex
workers in Argentina: high HIV, HPV, HBV, and syphilis prevalence. Int J Infect
Dis, v. 15, n. 9, p. 635-640, 2011.
EASL (European Association for the Study of the Liver). EASL clinical practice
guidelines: Management of chronic hepatitis B virus infection. J Hepatol, v. 57,
n. 1, p. 167-185, 2012.
ELGOUHARI, H. M.; TAMIMI, T. I.; CAREY, W. D. Hepatitis B virus infection:
Understanding its epidemiology, course, and diagnosis. Cleve Clin J Med, v. 75,
n. 12, p. 881-889, 2008.
FDA (Food and Drug Administration). Hepatitis B and C treatments, 2015. Disponível
em:
http://www.fda.gov/ForPatients/Illness/HepatitisBC/ucm408658.htm.
Acesso em: 18 de dezembro de 2015.
FEINSTONE, S. M.; KAPIKIAN, A. Z.; PURCELI R. H. Hepatitis A: detection by
immune electron microscopy of a virus like antigen associated with acute illness.
Science, v. 182, p. 1026-1028, 1973.
FERNANDES, C. N. et al. Prevalence of seropositivity for hepatitis B and C in pregnant
women. Rev Esc Enferm USP, v. 48, n. 1, p. 91-98, 2014.
FERNANDES, F. R. et al. HIV seroprevalence and high-risk sexual behavior among
female sex workers in Central Brazil. AIDS Care, v. 26, n. 9, p. 1095-1099, 2014.
FERNANDES, F. R. et al. Syphilis infection, sexual practices and bisexual behaviour
among men who have sex with men and transgender women: a cross-sectional
study. Sex Transm Infect, v. 91, n. 2, p. 142-149, 2015.
FERRARI, C. HBV and the immune response. Liver Int, v. 35, p. 121-128, 2015.
98
FERREIRA, R. C. et al. Hepatitis B virus infection profile in hemodialysis patients in
Central Brazil: prevalence, risk factors, and genotypes. Mem Inst Oswaldo Cruz,
v. 101, n. 6, p. 689-692, 2006.
FERREIRA, R. C. Infecção pelo vírus da hepatite B em usuários de drogas ilícitas na
região Centro-Oeste do Brasil: aspectos epidemiológicos e moleculares. 2008.
112f.
Tese
(Doutorado).
Instituto
de
Patologia
Tropical
e
Saúde
Pública/Universidade Federal de Goiás (IPTSP/UFG), Goiânia, Goiás, 2008.
FORREST, J. I. et al. Factors Associated with Productive Recruiting in a RespondentDriven Sample of Men who Have Sex with Men in Vancouver, Canada. J Urban
Health, v. 93, n. 2, p. 379-387, 2016.
FRANCO, E. et al. Hepatitis B: Epidemiology and prevention in developing countries.
World J Hepatol, v. 4, n. 3, p. 74-80, 2012.
FUENTE, R. A. et al. Pathogenesis of occult chronic hepatitis B virus infection. World
J Gastroenterol, v. 17, n. 12, p. 1543-1548, 2011.
FUJISAKI, S. et al. Outbreak of infections by hepatitis B virus genotype A and
transmission of genetic drug resistance in patients coinfected with HIV-1 in Japan.
J Clin Microbiol, v. 49, n. 3, p. 1017-1024, 2011.
GAMAGEDARA, N. et al. Cross-sectional study of hepatitis B immunity in MSM
between 2002 and 2012. Sex Transm Infect, v. 90, n. 1, p. 41-45, 2014.
GANEM, D.; VARMUS H. E. The molecular biology of the hepatitis B viruses. Annu
Rev Biochem, v. 56, p. 651-693, 1987.
GAO, S.; DUAN, Z. P.; COFFIN, C. S. Clinical relevance of hepatitis B virus variants.
World J Hepatol, v. 7, n. 8, p.1086-1096, 2015.
GERBER, M. A. et al. Electron microscopy and immunoelectronmicroscopy of
cytoplasmic hepatitis B antigen in hepatocytes. Am J Pathol, v. 75, n. 3, p. 489502, 1974.
GERLICH, W. H. Prophylactic vaccination against hepatitis B: achievements, challenges
and perspectives. Med Microbiol Immunol, v. 204, n. 1, p. 39-55, 2015.
GILBERT, L. K. et al. A comparison of hepatitis A and hepatitis B measures among
vaccinated and susceptible online men who have sex with men. Int J STD AIDS,
v. 21, n. 6, p. 400-405, 2010.
GISH, R. G. et al. Chronic hepatitis B: Virology, natural history, current management and
a glimpse at future opportunities. Antiviral Res, v. 121, p. 47-58, 2015.
99
GLEBE D.; BREMER C. M. The molecular virology of hepatitis B virus. Semin Liver
Dis, v. 33, n. 2, p. 103-112, 2013.
GOMES-GOUVÊA, M. S. et al. HBV carrying drug-resistance mutations in chronically
infected treatment-naive patients. Antivir Ther, v. 20, n. 4, p. 387-395, 2015.
GONÇALVES, V. F. et al. Incentives and barriers to HIV testing in men who have sex
with men in a metropolitan area in Brazil. Cad Saude Publica, v. 32, n. 5, p. 1-10,
2016.
GORGOS, L. Sexual transmission of viral hepatitis. Infect Dis Clin North Am, v. 27, n.
4, p. 811-836, 2013.
GUIDOTTI, L. G.; ISOGAWA, M.; CHISARI, F. V. Host-virus interactions in hepatitis
B virus infection. Curr Opin Immunol, v. 36, p. 61-66, 2015.
GUIMARÃES, M. L. et al. Assessing the HIV-1 Epidemic in Brazilian Drug Users: A
Molecular Epidemiology Approach. PLoS One, v. 10, n. 11, p. 1-17, 2015.
HAKRE, S. et al. Prevalence of HIV, syphilis, and other sexually transmitted infections
among MSM from three cities in Panama. J Urban Health, v. 91, n. 4, p. 793-808,
2014.
HALEGOUA-DE MARZIO, D.; HANN, H. W. Then and now: the progress in hepatitis
B treatment over the past 20 years. World J Gastroenterol, v. 20, n. 2, p. 401-413,
2014.
HECKATHORN, D. D. Respondent-driven sampling: a new approach to the study of
hidden populations. Social Problems, v. 44, p. 174-199, 1997.
HECKATHORN, D. D. Snowball versus respondent-driven sampling. Sociol Methodol,
v. 41, n. 1, p. 355-366, 2011.
HHS-CDC (Health and Human Services, Centers for Disease Control and Prevention).
Introduction to Respondent Driven Sampling. Participant Manual. 2008.
HOFFMANN, C. J. et al. Maternal hepatitis B and infant infection among pregnant
women living with HIV in South Africa. J Int AIDS Soc, v. 17, p. 1-5, 2014.
HOLLINGER, F. B. Hepatitis B virus genetic diversity and its impact on diagnostic
assays. J Viral Hepat, v. 14, n. 1, p. 11-15, 2007.
HOU, J.; LIU, Z.; GU, F. Epidemiology and prevention of hepatitis B virus infection. Int
J Med Sci, v. 2, p. 50-57, 2005.
HU, F. et al. Associations between hepatitis B virus basal core promoter/pre-core region
mutations and the risk of acute-on-chronic liver failure: a meta-analysis. Virol J,
v. 12, n. 87, p. 1-13, 2015.
100
HÜBSCHEN, J. M. et al. Detection of a new subgenotype of hepatitis B virus genotype
A in Cameroon but not in neighbouring Nigeria. Clin Microbiol Infect, v. 17, n.
1, p. 88-94, 2011.
HUNT, C. M. et al. Clinical relevance of hepatitis B viral mutations. Hepatol, v. 31, p.
1037-1044, 2000.
HUY, T. T. et al. Genomic characterization of HBV genotype F in Bolivia: genotype F
subgenotypes correlate with geographic distribution and T(1858) variant. Arch
Virol, v. 151, n. 3, p. 589-597, 2006.
ICTV (International Committee on Taxonomy of Viruses) 2015. In: Virus Taxonomy:
2014. Disponível em: < http://ictvonline.org/virustaxonomy.asp>. Acesso em: 05
de setembro de 2016.
INGILIZ, P. et al. Sexually transmitted infection with an immune-escape mutant hepatitis
B virus (HBV) in an HBV-vaccinated individual with acute HIV-HCV infection.
J Int AIDS Soc, v. 15, n. 6, p.18432, 2012.
ITO, K. et al. Impairment of hepatitis B virus virion secretion by single-amino-acid
substitutions in the small envelope protein and rescue by a novel glycosylation
site. J Virol, v. 84, n. 24, p. 12850-61, 2010.
JANSEN, K. et al. High prevalence and high incidence of coinfection with hepatitis B,
hepatitis C, and syphilis and low rate of effective vaccination against hepatitis B
in HIV-positive men who have sex with men with known date of HIV
seroconversion in Germany. PLoS One, v. 10, n. 11, p. 1-18, 2015.
JARAMILLO, C. M.; NAVAS, M. C. Escape mutants of hepatitis B virus. Rev Chilena
Infectol, v. 32, n. 2, p. 190-197, 2015.
JAYALAKSHMI, M. K.; KALYANARAMAN, N.; PITCHAPPAN, R. Hepatitis B virus
genetic diversity: Disease pathogenesis, viral replication (2013). Dr. German
Rosas-Acosta (Ed.), ISBN: 978-953-51-1055-2, InTech, DOI: 10.5772/53818.
Disponível em: <http://www.intechopen.com/books/viral-replication/hepatitis-bvirus-genetic-diversity-disease-pathogenesis>. Acesso em: 02 de fevereiro de
2016.
JEFFRIES, W. L. Beyond the bisexual bridge: sexual health among U.S. men who have
sex with men and women. Am J Prev Med, v. 47, n. 3, p. 320-329, 2014.
JIN, F. et al. Hepatitis A and B infection and vaccination in a cohort of homosexual men
in Sydney. Sex Health, v. 1, n. 4, p. 227-237, 2004.
101
JINDAL, A.; KUMAR, M.; SARIN, S. K. Management of acute hepatitis B and
reactivation of hepatitis B. Liver Int, v. 33, p. 164-175, 2013.
JOHNSTON, L. G. et al. HIV risk and the overlap of injecting drug use and high-risk
sexual behaviours among men who have sex with men in Zanzibar (Unguja),
Tanzania. Int J Drug Policy, v. 21, n. 6, p. 485-492, 2010.
JOHNSTON, L. G. et al. An empirical examination of respondent driven sampling design
effects among HIV risk groups from studies conducted around the world. AIDS
Behav, v. 17, n. 6, p. 2202-2210, 2013.
JOHNSTON, L. G. et al. A Systematic Review of Published Respondent-Driven
Sampling Surveys Collecting Behavioral and Biologic Data. AIDS Behav, v. 20,
n. 8, p. 1754-1776, 2016.
KAMIJO, N. et al. Mutations of pre-core and basal core promoter before and after
hepatitis B e antigen seroconversion. World J Gastroenterol, v. 21, n. 2, p. 541548, 2015.
KASSAK, K. et al. Hepatitis B virus and hepatitis C virus infections among female sex
workers and men who have sex with men in Lebanon: prevalence, risk behaviour
and immune status. Sex Health, v. 8, n. 2, p. 229-233, 2011.
KAY, A.; ZOULIM, F. Hepatitis B virus genetic variability and evolution. Virus Res, v.
127, p. 164-176, 2007.
KENDALL, C. et al. An empirical comparison of respondent-driven sampling, time
location sampling, and snowball sampling for behavioral surveillance in men who
have sex with men, Fortaleza, Brazil. AIDS Behav, v. 12, p. S97-104, 2008.
KERR, L. R. F. S. et al. HIV among MSM in a large middle-income country. AIDS, v.
27, p. 427-435, 2013.
KHANANI, M. R. et al. Prevalence of single, double, and triple infections of HIV, HCV
and HBV among the MSM community in Pakistan. J Infect, v. 61, n. 6, p. 507509, 2010.
KIDD-LJUNGGREN, K.; MIYAKAWA, Y.; KIDD, A. H. Genetic variability in
hepatitis B viruses. J Gen Virol, v. 83, p. 1267-1280, 2002.
KIMBI, G. C.; KEW, M. C.; KRAMVIS, A. The effect of the G1888A mutation of
subgenotype A1 of hepatitis B virus on the translation of the core protein. Virus
Res, v. 163, n. 1, p. 334-340, 2012.
102
KOIBUCHI, T. et al. Predominance of genotype A HBV in an HBV-HIV-1 dually
positive population compared with an HIV-1-negative counterpart in Japan. J
Med Virol, v. 64, n. 4, p. 435-440, 2001.
KOMATSU, H. Hepatitis B virus: where do we stand and what is the next step for
eradication? World J Gastroenterol, v. 20, n. 27, p. 8998-9016, 2014.
KRAMVIS, A. Genotypes and genetic variability of hepatitis B virus. Intervirology, v.
57, n. 3-4, p. 141-150, 2014.
KRAMVIS, A.; KEW, M. C. Relationship of genotypes of hepatitis B virus to mutations,
disease progression and response to antiviral therapy. J Viral Hepat, v. 12, n. 5,
p. 456-464, 2005.
KUO, A.; GISH, R. Chronic hepatitis B infection. Clin Liver Dis, v. 16, n. 2, p. 347-369,
2012.
KURBANOV, F.; TANAKA, Y.; MIZOKAMI, M. Geographical and genetic diversity
of the human hepatitis B virus. Hepatol Res, v. 40, n. 1, p. 14-30, 2010.
KWAK, M. S.; KIM, Y. J. Occult hepatitis B virus infection. World J Hepatol, v. 6, n.
12, p. 860-869, 2014.
KWON, S. Y.; LEE, C. H. Epidemiology and prevention of hepatitis B virus infection.
Korean J Hepatol, v. 17, p. 87-95, 2011.
LAGO, B. V. et al. Hepatitis B virus subgenotype A1: evolutionary relationships between
Brazilian, African and Asian isolates. PLoS One, v. 9, n. 8, p. 1-9, 2014.
LAMA, J. R. et al. Hepatitis B infection and association with other sexually transmitted
infections among men who have sex with men in Peru. Am J Trop Med Hyg, v.
83, n. 1, p. 194-200, 2010.
LANE, T. et al. High HIV prevalence among men who have sex with men in Soweto,
South Africa: results from the Soweto Men's Study. AIDS Behav, v. 15, n. 3, p.
626-634, 2011.
LAVANCHY, D. Hepatitis B virus epidemiology, disease burden, treatment, and current
and emerging prevention and control measures. J Viral Hepat, v. 11, n. 2, p. 97107, 2004.
LAZAREVIC, I. Clinical implications of hepatitis B virus mutations: recent advances.
World J Gastroenterol, v. 20, n. 24, p. 7653-7664, 2014.
LE BOUVIER, G. L. The heterogeneity of Australia antigen. J Infect Dis, v. 123, n. 6,
p. 671-675, 1971.
103
LI, Z.; HOU, X.; CAO, G. Is mother-to-infant transmission the most important factor for
persistent HBV infection? Emerg Microbes Infect, v. 4, n. 5, p. 1-9, 2015.
LIANG, T. J. Hepatitis B: The virus and disease. Hepatol, v. 49, p. 13-21, 2009.
LIAO, Y. et al. Precore mutation of hepatitis B virus may contribute to hepatocellular
carcinoma risk: evidence from an updated meta-analysis. PLoS One, v. 7, n. 6, p.
1-9, 2012.
LIAW, Y. F.; CHU, C. M. Hepatitis B virus infection. Lancet, v. 373, n. 9663, p. 582592, 2009.
LIN, C. L.; KAO, J. H. The clinical implications of hepatitis B virus genotype: Recent
advances. J Gastroenterol Hepatol, v. 26, p. 123-130, 2011.
LINKINS, R. W. et al. Hepatitis A and hepatitis B infection prevalence and associated
risk factors in men who have sex with men, Bangkok, 2006-2008. J Med Virol,
v. 85, n. 9, p. 1499-1505, 2013.
LIU, L. P. et al. HBx mutants differentially affect the activation of hypoxia-inducible
factor-1α in hepatocellular carcinoma. Br J Cancer, v. 110, n. 4, p. 1066-1073,
2014.
LIU, S. et al. Associations between hepatitis B virus mutations and the risk of
hepatocellular carcinoma: a meta-analysis. J Natl Cancer Inst, v. 101, n. 15, p.
1066-1082, 2009.
LOCARNINI, S.; ZOULIM, F. Molecular genetics of HBV infection. Antivir Ther, v.
15, p. 3-14, 2010.
LOCARNINI, S. et al. Possible origins and evolution of the hepatitis B virus (HBV).
Semin Cancer Biol, v. 23, p. 561-575, 2013.
LOCARNINI, S. et al. Strategies to control hepatitis B: Public policy, epidemiology,
vaccine and drugs. J Hepatol, v. 62, n. 1S, p. S76-S86, 2015.
LOK, A. S. et al. Antiviral drug-resistant HBV: standardization of nomenclature and
assays and recommendations for management. Hepatol, v. 46, p. 254-265, 2007.
LOPES, C. L. R. et al. Perfil soroepidemiológico da infecção pelo vírus da hepatite B em
profissionais das unidades de hemodiálise de Goiânia-Goiás, Brasil Central. Rev
Soc Bras Med Trop, v. 34, n. 6, p. 543-548, 2001.
LOZANO, R. et al. Global and regional mortality from 235 causes of death for 20 age
groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease
Study 2010. Lancet, v. 380, n. 9859, p. 2095-2128, 2012.
104
LUNA, E. J. et al. Efficacy and safety of the Brazilian vaccine against hepatitis B in
newborns. Rev Saude Publica, v. 43, n. 6, p. 1014-1020, 2009.
MA, N. F. et al. COOH-terminal truncated HBV X protein plays key role in
hepatocarcinogenesis. Clin Cancer Res, v. 14, n. 16, p. 5061-5068, 2008.
MA, X. et al. Trends in prevalence of HIV, syphilis, hepatitis C, hepatitis B, and sexual
risk behavior among men who have sex with men. Results of 3 consecutive
respondent-driven sampling surveys in Beijing, 2004 through 2006. J Acquir
Immune Defic Syndr, v. 45, n. 5, p. 581-587, 2007.
MACKELLAR, D. A. et al. Two decades after vaccine license: hepatitis B immunization
and infection among young men who have sex with men. Am J Public Health, v.
91, n. 6, p. 965-971, 2001.
MACLACHLAN, J. H.; COWIE, B. C. Hepatitis B virus epidemiology. Cold Spring
Harb Perspect Med, v. 5, n. 5, p. 1-12, 2015.
MAGNANI, R. et al. Review of sampling hard-to-reach and hidden populations for HIV
surveillance. AIDS, v. 19, p. S67-72, 2005.
MARINHO, T. A. et al. Epidemiology of hepatitis B virus infection among recyclable
waste collectors in central Brazil. Rev Soc Bras Med Trop, v. 47, n. 1, p. 18-23,
2014.
MARQUES, J. M. S. Investigação soroepidemiológica da infecção pelo vírus da
hepatite B em pacientes com diabetes mellitus tipo 2 em Goiânia-Goiás. 2015.
107f. Dissertação (Mestrado). Instituto de Patologia Tropical e Saúde
Pública/Universidade Federal de Goiás (IPTSP/UFG), Goiânia, Goiás, 2015.
MARTELLI, C. M. et al. Soroprevalência e fatores de risco para a infecção pelo vírus da
hepatite B pelos marcadores AgHBs e anti-HBs em prisioneiros e primodoadores
de sangue. Rev Saude Publica, v. 24, p. 270-276, 1990.
MATOS, M. A. et al. Epidemiology of hepatitis B virus infection in truck drivers in
Brazil, South America. Sex Transm Infect v. 84, n. 5, p. 386-389, 2008.
MATOS, M. A. Aspectos soroepidemiológicos e moleculares da infecção pelo vírus
da hepatite B em mulheres profissionais do sexo em Goiânia-Goiás. 2014.
Tese (Doutorado). Ciências da Saúde da Universidade Federal de Goiás. Goiânia,
Goiás, 2014.
MATOS, M. A. D. et al. Epidemiological study of hepatitis A, B, and C in the largest
Afro-Brazilian isolated community. Trans R Soc Trop Med Hyg, v. 103, p. 899905, 2009.
105
MCCREESH, N. et al. Respondent driven sampling: determinants of recruitment and a
method to improve point estimation. PLoS One, v. 8, n. 10, p. 1-9, 2013.
MCMAHON, B. J. The influence of hepatitis B virus genotype and subgenotype on the
natural history of chronic hepatitis B. Hepatol Int, v. 3, p. 334-342, 2009.
MCMAHON, B. J. et al. Antibody levels and protection after hepatitis B vaccine: results
of a 22-year follow-up study and response to a booster dose. J Infect Dis, v. 200,
n. 9, p. 1390-1396, 2009.
MCMILLAN, A. The changing prevalence of hepatitis B virus infection among men who
have sex with men who attended a sexually transmitted infections clinic in
Edinburgh, Scotland between 1989 and 2003. Int J STD AIDS, v. 17, n. 8, p. 539542, 2006.
MEDHI, G. K. et al. Factors associated with HIV among female sex workers in a high
HIV prevalent state of India. AIDS Care, v. 24, n. 3, p. 369-376, 2012.
MEIRELES, L. C.; MARINHO, R. T.; VAN DAMME, P. Three decades of hepatitis B
control with vaccination. World J Hepatol, v. 7, n. 18, p. 2127-2132, 2015.
MELLO, F. C. et al. Hepatitis B virus genotypes circulating in Brazil: molecular
characterization of genotype F isolates. BMC Microbiol, v. 7, p. 103, 2007.
MILICH, D. R.; MCLACHLAN, A. The nucleocapsid of hepatitis B virus is both a Tcellindependent and a T-cell-dependent antigen. Science, v. 234, p. 1398-1401,
1986.
MIRANDOLA, S. et al. Large-scale survey of naturally occurring HBV polymerase
mutations associated with anti-HBV drug resistance in untreated patients with
chronic hepatitis B. J Viral Hepat, v. 18, n. 7, p. 212-216, 2011.
MONTEALEGRE, J. R. et al. Respondent driven sampling for HIV biological and
behavioral surveillance in Latin America and the Caribbean. AIDS Behav, v. 17,
n. 7, p. 2313-2340, 2013.
MORAES, J. C.; LUNA, E. J.; GRIMALDI, R. A. Immunogenicity of the Brazilian
hepatitis B vaccine in adults. Rev Saude Publica, v. 44, n. 2, p. 353-359, 2010.
MORAES, T. C. et al. Hepatitis B virus infection among institutionalized mentally ill
patients in Brazil. Braz J Infect Dis, v. 19, n. 6, p. 643-647, 2015.
MOTTA-CASTRO, A. R. et al. Molecular epidemiology of hepatits B virus in a isolated
Afro-Brazilian community. Arch Virol, v. 153, p. 2197-2205, 2008.
106
MULYANTO et al. Identification of four novel subgenotypes (C13-C16) and two intergenotypic recombinants (C12/G and C13/B3) of hepatitis B virus in Papua
province, Indonesia. Virus Res, v. 163, n. 1, p. 129-140, 2012.
NABUCO, L. C. et al. Hepatitis B virus genotypes in Southeast Brazil and its relationship
with histological features. Mem Inst Oswaldo Cruz, v. 107, n. 6, p. 785-789,
2012.
NASSAL, M. HBV cccDNA: viral persistence reservoir and key obstacle for a cure of
chronic hepatitis B. Gut, v. 64, n. 12, p. 1972-1984, 2015.
NASSAL, M.; SCHALLER, H. Hepatitis B virus replication-an update. J Viral Hepat,
v. 3, p. 217-226, 1996.
NEURATH, A. R. et al. Identification and chemical synthesis of a host cell receptor
binding site on hepatitis B virus. Cell, v. 46, n. 3, p. 429-436, 1986.
NI, Y. et al. Hepatitis B and D viruses exploit sodium taurocholate co-transporting
polypeptide for species-specific entry into hepatocytes. Gastroenterology, v.
146, n. 4, p. 1070-1083, 2014.
NIELSEN, U. S. et al. Hepatitis B infection and vaccination coverage in men who have
sex with men consulting a Danish venereal disease clinic. Infect Dis (Lond), v.
47, n. 8, p. 517-522, 2015.
NORDER, H.; COUROUCE, A. M.; MAGNIUS, L. O. Molecular basis of hepatitis B
virus serotype variations within the four major subtypes. J Gen Virol, v. 73, n.
12, p. 3141- 3145, 1992.
NORDER, H. et al. Comparison of the amino acid sequences of nine different serotypes
of hepatitis B surface antigen and genomic classification of the corresponding
hepatitis B virus strains. J Gen Virol, v. 73, n. 5, p. 1201-1208, 1992.
NYAMATHI, A. et al. Correlates of hepatitis B virus and HIV knowledge among gay
and bisexual homeless young adults in Hollywood. Am J Mens Health, v. 7, n.
1, p. 18-26, 2013.
OKAMOTO, H. et al. Genomic heterogeneity of hepatitis B virus in a 54-year-old woman
who contracted the infection through materno-fetal transmission. Jpn J Exp Med,
v. 57, p. 231-236, 1987.
OKAMOTO, H. et al. Typing hepatitis B virus by homology in nucleotide sequence:
comparison of surface antigen subtypes. J Gen Virol, v. 69, p. 2575-2583, 1988.
107
OLIVEIRA, M. D. et al. Seroepidemiology of hepatitis B virus infection and high rate of
response to hepatitis B virus Butang vaccine in adolescents from low income
families in Central Brazil. Mem Inst Oswaldo Cruz, v. 101, p. 251-256, 2006.
OLIVEIRA, M. P. et al. Overt and occult hepatitis B virus infection among treatmentnaive HIV-infected patients in Brazil. J Med Virol, 2016a.
OLIVEIRA, M. P. et al. Prevalence, Risk Behaviors, and Virological Characteristics of
Hepatitis B Virus Infection in a Group of Men Who Have Sex with Men in Brazil:
Results from a Respondent-Driven Sampling Survey. PLoS One, v. 11, n. 8, p .114, 2016b.
ORDÖG, K. et al. Perinatal and intrafamily transmission of hepatitis B virus in three
generations of a low-prevalence population. J Med Virol, v. 70, n. 2, p. 194-204,
2003.
ORLANDO, R. et al. Prevention of hepatitis B virus infection: from the past to the future.
Eur J Clin Microbiol Infect Dis, v. 34, n. 6, p. 1059-1070, 2015.
OSIOWY, C. et al. Hepatitis B virus genotype G epidemiology and co-infection with
genotype A in Canada. J Gen Virol, v. 89, p. 3009-3015, 2008.
OTT, J. J. et al. Global epidemiology of hepatitis B virus infection: new estimates of agespecific HBsAg seroprevalence and endemicity. Vaccine, v. 30, n. 12, p. 22122219, 2012.
OZARAS, R. et al. Epidemiology of HBV subgenotypes D. Clin Res Hepatol
Gastroenterol, v. 39, n. 1, p. 28-37, 2015.
OZASA, A. et al. Influence of genotypes and precore mutations on fulminant or chronic
outcome of acute hepatitis B virus infection. Hepatology, v. 44, n. 2, p. 326-334,
2006.
OZKAL-BAYDIN, P. How did hepatitis B virus effect the host genome in the last
decade? World J Hepatol, v. 6, n. 12, p. 851-859, 2014.
PANDO, M. A. et al. Epidemiology of human immunodeficiency virus, viral hepatitis (B
and C), treponema pallidum, and human T-cell lymphotropic I/II virus among men
who have sex with men in Buenos Aires, Argentina. Sex Transm Dis, v. 33, n. 5,
p. 307-313, 2006.
PANDO, M. A. et al. HIV and other sexually transmitted infections among men who have
sex with men recruited by RDS in Buenos Aires, Argentina: high HIV and HPV
infection. PLoS One, v. 7, n. 6, p. 1-7, 2012.
108
PENROD, J. et al. A discussion of chain referral as a method of sampling hard-to-reach
populations. J Transcult Nurs, v. 14, n. 2, p. 100-107, 2003.
PEREIRA, L. M. et al. Population-based multicentric survey of hepatitis B infection and
risk factor differences among three regions in Brazil. Am J Trop Med Hyg, v.
81, n. 2, p. 240-247, 2009.
PITASI, M. A. et al. Hepatitis B virus (HBV) infection, immunity and susceptibility
among men who have sex with men (MSM), Los Angeles County, USA. AIDS
Behav, v. 18, p. 248-255, 2014.
POLLICINO, T. et al. Hepatitis B virus PreS/S gene variants: pathobiology and clinical
implications. J Hepatol, v. 61, n. 2, p. 408-417, 2014.
POLLICINO, T.; RAIMONDO, G. Occult hepatitis B infection. J Hepatol, v. 61, n. 3,
p. 688-689, 2014.
PONDÉ, R. A. Molecular mechanisms underlying HBsAg negativity in occult HBV
infection. Eur J Clin Microbiol Infect Dis, v. 34, n. 9, p. 1709-1731, 2015.
PORTO, S. O. et al. Prevalence and risk factors for HBV infection among street youth in
central Brazil. J Adolesc Health, v. 15, n. 7, p. 577-581, 1994.
POURKARIM, M. R. et al. Molecular identification of hepatitis B virus
genotypes/subgenotypes: revised classification hurdles and updated resolutions.
World J Gastroenterol, v. 20, n. 23, p. 7152-7168, 2014.
PRASETYO, A. A. et al. Men having sex with men in Surakarta, Indonesia:
demographics, behavioral characteristics and prevalence of blood borne
pathogens. Southeast Asian J Trop Med Public Health, v. 45, n. 5, p. 10321047, 2014.
PURI, P. Acute exacerbation of chronic hepatitis B: the dilemma of differentiation from
acute viral hepatitis B. J Clin Exp Hepatol, v. 3, n. 4, p. 301-312, 2013.
RAIMONDO, G. et al. Occult HBV infection. Semin Immunopathol, v. 35, n. 1, p. 3952, 2013.
RAJBHANDARI, R.; CHUNG, R. T. Treatment of Hepatitis B: A Concise Review. Clin
Transl Gastroenterol, v. 7, n. 9, p. 1-10, 2016
RAJPUT, P.; SHUKLA, S. K.; KUMAR, V. The HBx oncoprotein of hepatitis B virus
potentiates cell transformation by inducing c-Myc-dependent expression of the
RNA polymerase I transcription factor UBF. Virol J, v. 12, n. 62, 2015.
109
RAPICETTA, M.; FERRARI C.; LEVRERO, M. Viral determinants and host imune
responses in the pathogenesis of HBV infection. J Med Virol, v. 67, p. 454-457,
2002.
REINER, N. E.et al. Asymptomatic rectal mucosal lesions and hepatitis B surface antigen
at sites of sexual contact in homosexual men with persistent hepatitis B virus
infection. Ann Intern Med, v. 96, n. 2, p. 170-173, 1982.
REMIS, R. S. et al. Association of hepatitis B virus infection with other sexually
transmitted infections in homosexual men. Omega Study Group. Am J Public
Health, v. 90, n. 10, p. 1570-1574, 2000.
REMIS, R. S. et al. Prevalence of Sexually Transmitted Viral and Bacterial Infections in
HIV-Positive and HIV-Negative Men Who Have Sex with Men in Toronto. PLoS
One, v. 11, n. 7, p. 1-16, 2016.
RISHER, K. et al. Sexual stigma and discrimination as barriers to seeking appropriate
healthcare among men who have sex with men in Swaziland. J Int AIDS Soc, v.
16, n. 3, 2013.
RIZZETO, M. et al. Immunoflorescence detection of a new antigen/antibody system
(delta/antidelta) associated with hepatitis B virus in liver and serum of HBsAg
carriers. Gut, v. 18, p. 998-1003, 1977.
ROMERO, M. et al. Clinical significance of occult hepatitis B virus infection. World J
Gastroenterol, v. 17, n. 12, p. 1549-1552, 2011.
ROSA, H. et al. Associação entre hanseníase e infecção pelo vírus da hepatite B. Estudo
de prevalência realizado em Goiânia, Brasil Central. Rev Inst Med trop S Paulo,
v. 34, n. 5, 1992.
RUAN, Y. et al. Incidence of HIV-1, syphilis, hepatitis B, and hepatitis C virus infections
and predictors associated with retention in a 12-month follow-up study among
men who have sex with men in Beijing, China. J Acquir Immune Defic Syndr,
v. 52, n. 5, p. 604-610, 2009.
RUSSI, J. C. et al. Sexual transmission of hepatitis B virus, hepatitis C virus, and human
immunodeficiency virus type 1 infections among male transvestite comercial sex
workers in Montevideo, Uruguay. Am J Trop Med Hyg, v. 68, n. 6, p. 716-720,
2003.
SABIDÓ, M. et al. Sexual violence against men who have sex with men in Brazil: A
respondent-driven sampling survey. AIDS Behav, v. 19, n. 9, p. 1630-1641. 2015.
110
SAID, Z. N.; ABDELWAHAB, K. S. Induced immunity against hepatitis B virus. World
J Hepatol, v. 7, n. 12, p. 1660-1670, 2015.
SALGANIK, M. J.; HECKATHORN, D. D. Sampling and Estimation in Hidden
Populations Using Respondent-Driven Sampling. Sociological Methodology, v.
34, n. 1, p. 193-240, 2004.
SALGANIK, M. J. Variance estimation, design effects, and sample size calculations for
respondent-driven sampling. J Urban Health, v. 83, p. 98-112, 2006.
SAMAL, J.; KANDPAL, M.; VIVEKANANDAN, P. Molecular mechanisms underlying
occult hepatitis B virus infection. Clin Microbiol Rev, v. 25, n. 1, p. 142-163,
2012.
SCHREEDER, MT. et al. Hepatitis B in homosexual men: prevalence of infection and
factors related to transmission. J Infect Dis, v. 146, n. 1, p. 7-15, 1982.
SCHWEITZER, A. et al. Estimations of worldwide prevalence of chronic hepatitis B
virus infection: a systematic review of data published between 1965 and 2013.
Lancet, v. 386, n. 10003, p. 1546-1555, 2015.
SCOTT, R. M. et al. Experimental transmission of hepatitis B virus by semen and saliva.
J Infect Dis, v. 142, n. 1, p. 67-71, 1980.
SEAGE, G. R. et al. HIV and hepatitis B infection and risk behavior in young gay and
bisexual men. Public Health Rep, v. 112, n. 2, p. 158-167, 1997.
SEEGER, C.; MASON, W.S. Hepatitis B virus biology. Microbiol Mol Biol Rev, v. 64,
n. 1, p. 51-68, 2000.
SEEGER, C.; MASON, W.S. Molecular biology of hepatitis B virus infection. Virology,
v. 479, p. 672-686, 2015.
SHI, Y. H. Correlation between hepatitis B virus genotypes and clinical outcomes. Jpn J
Infect Dis, v. 65, n. 6, p. 476-482, 2012.
SHI, Y. H.; SHI, C. H. Molecular characteristics and stages of chronic hepatitis B virus
infection. World J Gastroenterol, v. 15, n. 25, p. 3099-3105, 2009.
SHIFFMAN, M. L. Management of cute hepatitis B. Clin Liver Dis, v. 4, p. 75-91, 2010.
SHLOMAI, A.; DE JONG, Y. P.; RICE, C. M. Virus associated malignancies: the role
of viral hepatitis in hepatocellular carcinoma. Semin Cancer Biol, v. 26, p. 7888, 2014.
SILVA, C. O. et al. Seroprevalence of hepatitis B virus infection in individuals with
clinical evidence of hepatitis in Goiania, Goiás. Detection of viral DNA and
111
determination of subtypes. Rev Inst Med Trop Sao Paulo, v. 44, p. 331-334,
2002.
SILVA, P. A. et al. Seroprevalence of hepatitis B virus infection and seroconvertion to
anti-HBsAg in laboratory staff in Goiania, Goias. Rev Soc Bras Med Trop, v.
38, p. 153-156, 2005.
SILVA, L. N. Prevalência da infecção pelo vírus da Hepatite B e situação vacinal em
usuários de crack institucionalizados em Goiânia - Goiás. 2014. 109f.
Dissertação (Mestrado). Ciências da Saúde da Universidade Federal de Goiás.
Goiânia, Goiás, 2014.
SOARES, C. C. et al. HIV-1, HBV, HCV, HTLV, HPV-16/18, and Treponema pallidum
infections in a sample of Brazilian men who have sex with men. PLoS One, v. 9,
n. 8, p. 1-8, 2014.
SONG, E. Y. et al. Prevalence of occult hepatitis B virus infection in a general adult
population in Korea. Intervirology, v. 52, n. 2, p. 57-62, 2009.
SOUTO, F. J. Distribution of hepatitis B infection in Brazil: the epidemiological situation
at the beginning of the 21 st century. Rev Soc Bras Med Trop, v. 49, n.1, p. 1123, 2016.
SQUADRITO, G.; SPINELLA, R.; RAIMONDO, G. The clinical significance of occult
HBV infection. Ann Gastroenterol, v. 27, n. 1, p. 15-19, 2014.
STORHOLM, E. D. et al. Hepatitis vaccination of men who have sex with men at gay
pride events. Prev Sci, v. 11, n. 2, p. 219-27, 2010.
STUEVE, A. et al. Time-space sampling in minority communities: results with young
Latino men who have sex with men. Am J Public Health, v. 91, n. 6, p. 922-926,
2001.
STUYVER, L. et al. A new genotype of hepatitis B virus: complete genome and
phylogenetic relatedness. J Gen Virol, v. 81, p. 67-74, 2000.
SUNBUL, M. Hepatitis B virus genotypes: global distribution and clinical importance.
World J Gastroenterol, v. 20, n. 18, p. 5427-5434, 2014.
SUTMOLLER, F. et al. The Rio de Janeiro HIV vaccine site-II. Recruitment strategies
and socio-demographic data of a HIV negative homosexual and bisexual male
cohort in Rio de Janeiro, Brazil. Mem Inst Oswaldo Cruz, v. 92, n. 1, p. 39-46,
1997.
SUTMOLLER, F. et al. Human immunodeficiency virus incidence and risk behavior in
the 'Projeto Rio': results of the first 5 years of the Rio de Janeiro open cohort of
112
homosexual and bisexual men, 1994-98. Int J Infect Dis, v. 6, n. 4, p. 259-265,
2002.
SVICHER, V. et al. Role of hepatitis B virus genetic barrier in drug-resistance and
immune-escape development. Dig Liver Dis, v. 43, n. 12, p. 975-983, 2011.
TAJIRI, K.; SHIMIZU, Y. Unsolved problems and future perspectives of hepatitis B virus
vaccination. World J Gastroenterol, v. 21, n. 23, p. 7074-7083, 2015.
TAN, A.; KOH, S.; BERTOLETTI, A. Immune response in hepatitis B virus infection.
Cold Spring Harb Perspect Med, v. 5, n. 8, p. 1-18, 2015.
TAN, Y. W. et al. Natural YMDD-motif mutants affect clinical course of lamivudine in
chronic hepatitis B. World J Gastroenterol, v. 21, n. 7, p. 2089-2095, 2015.
TATEMATSU, T. et al. A genetic variant of hepatitis B virus divergent from known
human and ape genotypes isolated from a Japanese patient and provisionally
assigned to new genotype J. J Virol, v. 22, n. 4, p. 10538-10547, 2009.
TAVARES, R. S. et al. Infecção pelo vírus da hepatite B em hemofílicos em Goiás:
soroprevalência, fatores de risco associados e resposta vacinal. Rev Bras
Hematol Hemoter, v. 26, n. 3, p. 183-188, 2004.
TELES, S. A. et al. Hepatitis B virus infection profile in Central Brazilian hemodialysis
population. Rev Inst Med trop S Paulo, v. 40, n. 5, 1998.
TELES, S. A. et al. Hepatitis B virus transmission in Brazilian hemodialysis units:
serological and molecular follow-up. J Med Virol, v. 68, p. 41-49, 2002.
THEDJA, M. D. et al. Ethnogeographical structure of hepatitis B virus genotype
distribution in Indonesia and discovery of a new subgenotype, B9. Arch Virol, v.
156, n. 5, p. 855-868. 2011.
THOMAS, E.; YONEDA, M.; SCHIFF, E. R. Viral hepatitis: past and future of HBV and
HDV. Cold Spring Harb Perspect Med, v. 5, n. 2, p. 1-11, 2015.
THUNG, S. N.; GERBER, M. A. Polyalbumin receptors: their role in the attachment of
hepatitis B virus to hepatocytes. Semin Liver Dis, v. 4, p. 69-75, 1984.
TIIT (The Incident Investigation Teams and Others). Transmission of hepatitis B to
patients from four infected surgeons without hepatitis B e antigen. N Engl J Med,
v. 336, n. 3, p. 178-184, 1997.
TILLMANN, H. L.; PATEL, K. Therapy of acute and fulminant hepatitis B.
Intervirology, v. 57, n. 3-4, p. 181-188, 2014.
TRAN, T. T.; TRINH, T. H.; ABE, K. New complex recombinant genotype of hepatitis
B virus identified in Vietnam. J Virol, v. 82, n. 11, p. 5657-5663, 2008.
113
TRÉPO, C.; CHAN, H. L.; LOK, A. Hepatitis B virus infection. Lancet, v. 384, n. 9959,
p. 2053-2063, 2014.
TRINKS, J. et al. Two simultaneous hepatitis B virus epidemics among injecting drug
users and men who have sex with men in Buenos Aires, Argentina: characterization
of the first D/A recombinant from the American continent. J Viral Hepat, v. 15, n.
11, p. 827-838, 2008.
TSENG, Y. T. et al. Seroprevalence of hepatitis virus infection in men who have sex with
men aged 18-40 years in Taiwan. J Formos Med Assoc, v. 111, n. 8, p. 431-438,
2012.
TUTTLEMAN, J. S.; POURCEL, C.; SUMMERS, J. Formation of the pool of covalently
closed circular viral DNA in hepadnavirus-infected cells. Cell, v. 47, n. 3, p. 451460, 1986.
URBANUS, A. T. et al. Viral hepatitis among men who have sex with men, epidemiology
and public health consequences. Euro Surveill, v. 14, n. 47, p. 19421, 2009.
VALADEZ, J. J. et al. Filling the Knowledge Gap: Measuring HIV Prevalence and Risk
Factors among Men Who Have Sex with Men and Female Sex Workers in Tripoli,
Libya. PLoS One, v. 8, n. 6, p. 1-14, 2013.
VAN DER KUYL, A. C. et al. High prevalence of hepatitis B virus dual infection with
genotypes A and G in HIV-1 infected men in Amsterdam, the Netherlands, during
2000-2011. BMC Infect Dis, v. 13, n. 540, p. 1-8, 2013.
VAN HOUDT, R. et al. Ongoing transmission of a single hepatitis B virus strain among
men having sex with men in Amsterdam. J Viral Hepat, v. 17, n. 2, p. 108-114,
2010.
VAN HOUDT, R. et al. Unexpectedly high proportion of drug users and men having sex
with men who develop chronic hepatitis B infection. J Hepatol, v. 57, n. 3, p.
529-533, 2012.
VERAS, M. A. S. M. et al. High HIV Prevalence among Men who have Sex with Men in
a Time-Location Sampling Survey, São Paulo, Brazil. AIDS Behav, v. 19, n. 9,
p. 1589-98, 2014.
VET, R.; DE WIT, J. B.; DAS, E. Factors associated with hepatitis B vaccination among
men who have sex with men: a systematic review of published research. Int J
STD AIDS, p. 1-9, 2015.
VILLAR, L. M. et al. Update on hepatitis B and C virus diagnosis. World J Virol, v. 4,
n. 4, p. 323-342, 2015.
114
VOLK, J. E. et al. Acceptability and feasibility of HIV self-testing among men who have
sex with men in Peru and Brazil. Int J STD AIDS, v. 27, n. 7, p. 531-6, 2016.
VOLZ, E.; HECKATHORN, D. D. Probability Based Estimation Theory for Respondent
Driven Sampling. Journal of Official Statistics, v. 24, n. 1, p. 79-97, 2008.
WANG, C. et al. Prevalence and factors associated with hepatitis B immunization and
infection among men who have sex with men in Beijing, China. PLoS One, v. 7,
n. 10, p. 1-8, 2012.
WARNER, N.; LOCARNINI, S. Mechanisms of hepatitis B virus resistance
development. Intervirology, v. 57, n. 3-4, p. 218-224, 2014.
WASLEY, A. et al. The prevalence of hepatitis B virus infection in the United States in
the era of vaccination. J Infect Dis, v. 202, n. 2, p. 192-201, 2010.
WEI, C. et al. Reaching black men who have sex with men: a comparison between
respondent-driven sampling and time-location sampling. Sex Transm Infect, v.
88, n. 8, p. 622-626, 2012.
WHITE, R. G. et al. Respondent driven sampling--where we are and where should we be
going? Sex Transm Infect, v. 88, n. 6, p. 397-399, 2012.
WHITE, R. G. et al. Strengthening the Reporting of Observational Studies in
Epidemiology for respondent-driven sampling studies: "STROBE-RDS"
statement. J Clin Epidemiol, v. 68, n. 12, p. 1463-1471, 2015.
WHO (World Health Organization). Hepatitis B vaccines. Wkly Epidemiol Rec, v. 84,
n. 40, p. 405-19, 2009.
WHO (World Health Organization). Prevention and treatment of HIV and other
sexually transmitted infections among men who have sex with men and
transgender people. Recommendations for a public health approach. 2011.
WHO (World Health Organization). Prevention e control of viral hepatitis infection:
Framework for Global Action. 2012.
WHO (World Health Organization). Hepatitis B. Fact sheet n°204. Disponível em: <
http://www.who.int/mediacentre/factsheets/fs204/en/> Acesso em: 05 de junho de
2015a.
WHO (World Health Organization). Guidelines for the prevention, care and treatment
of persons with chronic hepatitis B infection. 2015b.
WU, T. W.; LIN, H. H.; WANG, L. Y. Chronic hepatitis B infection in adolescents who
received primary infantile vaccination. Hepatology, v. 57, n. 1, p. 37-45, 2013.
115
YAN, H. et al. Sodium taurocholate cotransporting polypeptide is a functional receptor
for human hepatitis B and D virus. Elife, v. 1, p. 1-28, 2012.
YANG, H. C. et al. Distinct evolution and predictive value of hepatitis B virus precore
and basal core promoter mutations in interferon-induced hepatitis B e antigen
seroconversion. Hepatology, v. 57, n. 3, p. 934-943, 2013.
YANO, Y.; AZUMA, T.; HAYASHI, Y. Variations and mutations in the hepatitis B virus
genome and their associations with clinical characteristics. World J Hepatol, v.
7, n. 3, p. 583-592, 2015.
YEE, L. J.; RHODES, S. D. Understanding correlates of hepatitis B virus vaccination in
men who have sex with men: what have we learned? Sex Transm Infect, v. 78,
n. 5, p. 374-377, 2002.
YOU, C. R. et al. Update on hepatitis B virus infection. World J Gastroenterol, v. 20,
n. 37, p. 13293-13305, 2014.
ZEHENDER, G. et al. Enigmatic origin of hepatitis B virus: an ancient travelling
companion or a recent encounter? World J Gastroenterol, v. 20, n. 24, p. 76227634, 2014.
ZHAND, S. et al. Correlation between hepatitis B G1896A precore mutations and HBeAg
in chronic HBV patients. Jundishapur J Microbiol, v. 8, n. 2, p. 1-4, 2015.
ZHANG, X. D.; WANG, Y.; YE, L. H. Hepatitis B virus X protein accelerates the
development of hepatoma. Cancer Biol Med, v. 11, n. 3, p. 182-190, 2014.
ZHANG, X.; DING, H. G. Key role of hepatitis B virus mutation in chronic hepatitis B
development to hepatocellular carcinoma. World J Hepatol, v. 7, n. 9, p. 12821286, 2015.
ZHANG, Y. et al. Comparative study of the different activities of hepatitis B virus wholeX protein and HBx in hepatocarcinogenesis by proteomics and bioinformatics
analysis. Arch Virol, v. 160, n. 7, p. 1645-1656, 2015.
ZHU, M. et al. HBx induced AFP receptor expressed to activate PI3K/AKT signal to
promote expression of Src in liver cells and hepatoma cells. BMC Cancer, v. 15,
n. 362, p. 1-9, 2015.
116
ANEXOS
Anexo 1 - Parecer do Comitê de Ética em Pesquisa.
117
Anexo 2 - Artigo 1: Prevalence, Risk Behaviors, and Virological Characteristics of
Hepatitis B Virus Infection in a Group of Men Who Have Sex with Men in Brazil:
Results from a Respondent-Driven Sampling Survey (artigo publicado).
118