UNIVERSIDADE FEDERAL DE PERNAMBUCO
CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE PÓS-GRADUAÇÃO EM MEDICINA TROPICAL
ALBA MARIA ELOY ZAIDAN
CARACTERIZAÇÃO GENÉTICA DO VÍRUS DA HEPATITE B EM
ALAGOAS, BRASIL
RECIFE – PE
2009
ALBA MARIA ELOY ZAIDAN
CARACTERIZAÇÃO GENÉTICA DO VÍRUS DA HEPATITE B EM
ALAGOAS, BRASIL
Tese apresentada ao Programa de Pós-Graduação
em Medicina Tropical do Centro de Ciências da
Saúde da Universidade Federal de Pernambuco,
como parte dos requisitos para a obtenção do título
de Doutor em Medicina Tropical.
Orientadora: Prof.a Dr.a Maria Rosângela Cunha Duarte Coêlho
Co-orientadora: Dr.a Regina Célia Moreira
RECIFE – PE
2009
Zaidan, Alba Maria Eloy
Caracterização genética do vírus da hepatite B em
Alagoas / Alba Maria Eloy Zaidan. – Recife : O Autor,
2009.
121 folhas ; il., fig., tab.
Tese (doutorado) – Universidade Federal
Pernambuco. CCS. Medicina Tropical, 2009.
de
Inclui bibliografia, anexos e apêndices.
1. Hepatite B.
616.36-002
616.362 3
I. Título.
CDU (2.ed.)
CDD (22.ed.)
UFPE
CCS2009-097
UNIVERSIDADE FEDERAL DE PERNAMBUCO
CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE PÓS-GRADUAÇÃO EM MEDICINA TROPICAL
REITOR
Profº. Amaro Henrique Pessoa Lins
PRÓ-REITOR PARA ASSUNTOS DE PESQUISA E PÓS-GRADUAÇÃO
Profº. Anísio Brasileiro de Freitas Dourado
DIRETOR DO CENTRO DE CIÊNCIAS DA SAÚDE
Profº. José Tadeu Pinheiro
COORDENADOR DO PROGRAMA DE PÓS-GRADUAÇÃO EM MEDICINA
TROPICAL
Profª. Heloísa Ramos Lacerda de Melo
VICE-COORDENADOR DO PROGRAMA DE PÓS-GRADUAÇÃO EM MEDICINA
TROPICAL
Profª. Maria Rosângela Cunha Duarte Coêlho
CORPO DOCENTE
Profª. Célia Maria Machado Barbosa de Castro
Profª. Elizabeth Malagueño de Santana
Profª. Heloísa Ramos Lacerda de Melo
Profª. Maria Amélia Vieira Maciel
Profª. Maria Rosângela Cunha Duarte Coelho
Profº. Ricardo Arraes de Alencar Ximenes
Profª. Vera Magalhães da Silveira
Profº Edmundo Pessoa de Almeida Lopes Neto
Profª Maria do Amparo Andrade
Profª. Valdênia Maria Oliveira de Souza
Ao meu pai, João Xavier Eloy (in memorian) e a minha mãe, Maria de Lourdes Eloy
A busca do conhecimento foi a herança que recebi de vocês e por este caminho busquei a minha
realização pessoal. Hoje estou conquistando mais uma vitória!
Aos meus filhos Tiago e Clarissa, por estarem sempre ao meu lado e reconhecerem a importância
deste trabalho para a minha profissão.
Aos meus irmãos e cunhados, pelo apoio e incentivo.
AGRADECIMENTOS
Ó Senhor meu Deus! Obrigada pelos amigos que colocastes à minha disposição e pelo carinho
e apoio da minha família. Sempre senti em todos uma torcida sincera revelando a Tua vontade.
Obrigada Senhor por esta vitória!
À Profa. Dra. Maria Rosângela C.D. Coêlho pela orientação deste trabalho, atenção, apoio e
estímulo, tornando-me uma admiradora de sua força e determinação para a pesquisa.
À Dra. Regina Célia Moreira por ter aceito a co-orientação deste trabalho colocando a
disposição o Laboratório de Hepatites Virais do Instituto Adolfo Lutz de São Paulo para o treinamento
das técnicas em biologia molecular.
À Coordenação do Curso de Pós-Graduação em Medicina Tropical da UFPE pela contribuição
na melhoria do nível científico dos docentes.
Ao Professor da Pós-Graduação em Medicina Tropical Dr. Ricardo Ximenes pela construção
de uma forma mais elaborada do projeto de tese.
Aos funcionários do Departamento de Medicina Tropical da UFPE, Sr. Walter Galdino e Sra.
Jupira Ramos pelos serviços prestados.
Ao Dr. João Macário de Omena (in memorian), ex-diretor geral do HUAA, pelo apoio
recebido para seguir em frente ainda quando estava tentando iniciar o curso de Pós-Graduação.
Ao Dr. Paulo Luiz Cavalcante, diretor geral do HUAA, pelo apoio recebido.
Ao Prof. Dr. Cícero Eduardo Ramalho por ter colocado à disposição o Laboratório de
Biotecnologia do CECA/UFAL para a realização dos procedimentos técnicos de biologia molecular.
Aos amigos do Laboratório de Biotecnologia do CECA/UFAL, representados pela Profa. Leila
de Paula Rezende, Velber Xavier e Luiz Sérgio Duarte, pelo apoio e momentos de descontração.
Aos amigos e colegas do Instituto de Ciências Biológicas e da Saúde da UFAL, em especial
Laura Vasconcelos, Silvana Aires, Eliane Maurício e Erlon Oliveira pelo apoio durante o
afastamento das minhas atividades docentes.
Aos médicos Fernando Barreiros, Rosileide Alves, Andréa Agra, Leila Tojal, Rosângela
Wyszomirsks e Manoel Calheiros pelo encaminhamento dos pacientes.
Aos funcionários e amigas Arliete Ramos, Vânia Maia, Eliege dos Santos e Maria
Marluce Nogueira do Laboratório de Análises Clínicas do HUAA/UFAL e do HEHA/UNCISAL
pela coleta das amostras e dosagem de ALT.
Ao Dr. Marcílio Figueiredo do Instituto Adolfo Lutz pelo treinamento das técnicas de
PCR “in house” e análise das seqüências.
Aos funcionários do Laboratório de Hepatites Virais do Instituto Adolfo Lutz pela
convivência agradável e em especial a Dra. Ângela Spina pela assistência recebida.
Ao Dr. José Luiz de Lima Filho, diretor do LIKA/UFPE pelo apoio e, ao Setor de
Virologia, especialmente ao doutorando da Pós-Graduação em Medicina Tropical Jéfferson
Almeida pela revisão da tese e submissão dos artigos.
À chefe do Setor de Biologia Molecular do LIKA/UFPE, Profa. Dra. Cíntia Rocha, ao
doutorando Lucas Brandão e ao graduando Michel Naslavsky pela colaboração na utilização do
seqüenciador automático.
Aos colegas do doutorado pelo companheirismo e troca de conhecimentos. Em especial a
Linda Délia pela parceria nas viagens Maceió↔Recife e à Matilde Carrera pela companhia nas
leituras do Evangelho, fortalecendo nossa caminhada.
À Maria Helena Lessa, bibliotecária da UFAL, pela orientação bibliográfica deste
trabalho.
À Edjaneide dos Santos (Didi) pelos serviços de apoio.
À FAPEAL pela concessão de uma bolsa de Doutorado.
Aos pacientes que participaram da pesquisa os quais foram imprescindíveis para a sua
realização.
Avance para águas mais profundas, e lancem as redes para a pesca.
Lucas 5,4
RESUMO
O vírus da hepatite B (HBV) está classificado em oito genótipos, A – H, com prevalências
distintas em diferentes áreas geográficas. As divergências intergenotípicas foram definidas
arbitrariamente como uma variação nucleotídica superior a 8% na seqüência completa do genoma
viral. Naturalmente são encontradas variantes das regiões pré-S/S, pré-core/C e P. A mutação na
região pré-core, G1896A geralmente é descrita em indivíduos portadores de infecções pelo HBV
com ausência de HBeAg (antígeno e do vírus da hepatite B) e replicação viral ativa, apesar da
presença de anti HBe. Enquanto, que a detecção das mutações na região basal do promotor core
(BCP), A1762T e G1764A, independem do perfil HBeAg/anti-HBe. O objetivo deste estudo foi
investigar os genótipos e a presença de mutações pré-core G1896A e BCP A1762T e G1764A no
HBV, analisando carga viral, perfil HBeAg/anti-HBe e nível sérico de alanina aminotransferase
(ALT) em pacientes portadores de infecções pelo HBV. Foi realizado um estudo transversal
descritivo envolvendo pacientes encaminhados pelos Centros de Referências em Hepatites Virais
do Estado de Alagoas, Brasil, durante o período de setembro de 2006 a abril de 2008. Foram
selecionados 119 pacientes com HBsAg e anti-HBc positivos, entre os quais, 2,5% (3) tinham o
diagnóstico de hepatite aguda, 69,7% (83) de portador assintomático e 27,8% (33) de hepatite
crônica. As amostras de sangue foram submetidas aos procedimentos de extração e amplificação
do genoma viral visando o seqüenciamento parcial do gene S e da região pré-core. O DNA HBV
foi detectado em 70,6% (84/119) dos pacientes, e os genótipos foram identificados em 95,2%
(80/84). O genótipo A em 92,5% (74/80), seguido do genótipo C em 5,0% (4/80) e 1,25% (1/80)
para ambos os genótipos D e F. No genótipo A, a presença de timina/citosina na posição 1858 foi
identificada em 50% (13/26) das seqüências analisadas, a mutação G1896A em 3,8% (1/26) e as
mutações BCP A1762T e G1764A em 52,4% (11/21). A pesquisa demonstrou que o genótipo A
foi predominante em Alagoas, Brasil e a maioria das infecções apresentou carga viral reduzida,
concentração sérica normal da ALT e soroconversão do HBeAg para anti-HBe, caracterizando a
fase residual da infecção crônica pelo HBV. O estudo também revelou a circulação de mutantes
pré-core e BCP do genótipo A. As mutações BCP foram detectadas equitativamente nos
portadores assintomáticos e com hepatite crônica, independentemente da carga viral e nível sérico
de ALT.
Palavras chaves: Vírus da hepatite B, genótipos, mutação pré-core, mutação no promotor core.
ABSTRACT
Hepatitis B virus (HBV) has been classified into eight genotypes (A to H), with distinct
geographical distributions. The divergences between the genotypes have been defined arbitrarily,
based on a difference of more than 8% in the virus genome sequence. Naturally variants are found
in regions pre-S/S, pre-core/C and P. The mutation of the precore region (G1896A) is most
frequently detected in genotypes B, C, D, E and F, in hepatitis B virus (HBV) infections, while
mutations in the basal core promoter (BCP) region (1762T/1764A) have been described in all
genotypes. The aim of this study was to investigate the genotypes and the presence of pre-core
mutations G1896A and BCP A1762T and G1764A in HBV, analyzing, viral load, profile HBeAg
/ anti-HBe and serum levels of alanine aminotransferase (ALT) in patients with infections HBV.
This was a descriptive cross-sectional study involving patients referred by the Reference Center
on Viral Hepatitis of the State of Alagoas, Brazil, during the period September 2006 to April
2008. We selected 119 patients with HBsAg and anti-HBc positive, including 2.5% (3) had the
diagnosis of acute hepatitis, 69.7% (83) of asymptomatic carriers and 27.8% (33) of chronic
hepatitis. Blood samples were subjected to the procedures for extraction and amplification of the
viral genome to the partial sequencing of the gene S and pre-core region. The HBV DNA was
detected in 70.6% (84/119) of patients and the genotypes in 95.2% (80/84). The following
genotypes were identified: genotype A in 92.5% (74/80), followed by genotype C in 5.0% (4/80)
and 1.25% (1/80) for both genotypes D and F. In genotype A, the presence of thymine/cytosine at
position 1858 was identified in 50% (13/26) of the sequences analyzed, the G1896A mutation in
3.8% (1/26) and the BCP mutations in 52.4% (11/21). The research showed that genotype A was
predominant in Alagoas, Brazil, most of the infections had reduced viral load, normal serum
concentration of ALT and serum-conversion of HBeAg to anti-HBe, characterizing the residual
phase of chronic HBV infection. BCP mutations were detected equally in asymptomatic carriers
and chronic hepatitis, independently the viral load and serum levels of ALT.
Key words: Hepatitis B virus, genotypes, pre-core mutation, mutation in the core promoter.
LISTA DE ILUSTRAÇÕES
Tese
Figura 1 Estrutura do vírus da hepatite B
20
Figura 2. Microscopia eletrônica do vírus da hepatite B
21
Figura 3. Genoma do vírus da hepatite B e proteínas codificadas
22
Artigo II
Versão em português
Figura 1. Genótipos Identificados em Alagoas-Brasil. Setembro 2006 a Outubro 2007..
68
Versão em inglês
Figure 1. Genotypes identified in Alagoas, Brazil. September 2006 to Outubro 2007….
80
LISTA DE TABELAS
Tese
Tabela 1. Taxa de positividade dos genótipos do HBV mais freqüentes no Brasil.............
Tabela 2. Relação dos Primers utilizados nas amplificações do gene S e regiões pré-core
e core.
Artigo I
34
36
Versão em português
Tabela 1. Dados laboratoriais das infecções pelo HBV genótipo A segundo a condição
clínica. Alagoas, Nordeste/ Brasil. Setembro 2006 a Abril 2008........................................
Versão em inglês
Table 1. Laboratory data on HBV infections due to genotype A, according to clinical
condition. Alagoas, northeastern Brazil. September 2006 to April 2008…………………
Artigo II
46
56
Versão em português
Tabela 1. Dados demográficos e características da infecção pelo vírus da hepatite B em
portadores assintomáticos e hepatite crônica. Alagoas-Brasil, Setembro 2006 a Outubro 2007......
67
Versão em inglês
Table 1. Demographic data and characteristics of infections due to hepatitis B virus
among asymptomatic carriers and those with chronic hepatitis. Alagoas, Brazil,
September 2006 to October 2007…………………………………………………………
79
LISTA DE ABREVIATURAS E SIGLAS
ALT – Alanina aminotransferase
Anti-HBc – Anticorpo contra o antígeno do capsídeo do vírus da hepatite B
Anti-HBs – Anticorpo contra o antígeno da superfície do vírus da hepatite B
Anti-HBe – Anticorpo contra o antígeno e do vírus da hepatite B
BCP – Basal core promoter
cccDNA – Covalenty closed circular DNA
CHC – Carcinoma hepatocelular
DNA HBV– Ácido desoxirribonucléico do vírus da hepatite B
E1/E2 – Enhacers
ELISA – Enzime Linked Immunosorbent Assay
FAPEAL – Fundação de Amparo à Pesquisa do Estado de Alagoas
FINEP – Financiadora de Estudos e Projetos
gp – glicoproteína
HBcAg – Antígeno capsídeo do vírus da hepatite B
HBeAg – Antígeno e do vírus da hepatite B
HBsAg – Antígeno de superfície do vírus da hepatite B
HUAA – Hospital Universitário Prof. Dr. Alberto Antunes
HEHA – Hospital Escola Prof. Dr. Hélvio Auto
IBGE – Instituto Brasileiro de Geografia e Estatística
LIKA – Laboratório de Imunopatologia Keiko-Asami
LIPA– Line Probe Assay
NADH – Nicotinamida-Adenina-Dinucleotídio na sua forma reduzida
NCBI – The National Center for Biotechnology Information
ORF – Open Reading Frame
PCR – Polimerase Chain Reaction
RFLP – Restriction Fragment Lenght Polymorphism
RNA – Ácido ribonucléico
UFAL – Universidade Federal de Alagoas
UNCISAL – Universidade de Ciências da Saúde do Estado de Alagoas
HBV – Vírus da hepatite B
SUMÁRIO
1.0 Revisão de literatura.........................................................................................................
20
2.0 Formulação da questão da pesquisa.................................................................................
32
3.0 Objetivos .........................................................................................................................
33
3.1 Objetivo geral...................................................................................................................
33
3.2 Objetivos específicos.......................................................................................................
33
4.0 Metodologia.....................................................................................................................
34
4.1 Desenho do estudo...........................................................................................................
34
4.2 Definição do tamanho amostral.......................................................................................
34
4.3 População de estudo.........................................................................................................
35
4.4 Coleta de dados e amostras..............................................................................................
35
4.5 Dosagem de alanina aminotrasferase...............................................................................
35
4.6. Marcadores sorológicos................................................................................................... 35
4.7 Extração do DNA viral..................................................................................................... 35
4.8 Amplificação do gene S e regiões pré-core e core - PCR nested.....................................
36
4.9.Amplificação parcial do gene S ......................................................................................
37
4.10 Amplificação parcial da região pré-core .......................................................................
37
4.11.Carga viral - Titulação do DNA HBV..........................................................................
37
4.12 Eletroforese em gel de agarose dos fragmentos genômicos..........................................
38
4.13 Reação de seqüenciamento............................................................................................
38
4.14 Análise das seqüências...................................................................................................
38
4.15 Análise dos dados..........................................................................................................
39
4.16 Limitação metodológica do estudo................................................................................
39
5.0 Artigo I (Caracterização genotípica do vírus da hepatite B em Alagoas, Brasil)..... 40
Resumo..................................................................................................................................
40
Introdução..............................................................................................................................
41
Material e Métodos ...............................................................................................................
42
Desenho do estudo e seleção dos pacientes...........................................................................
42
Coleta de dados e amostras....................................................................................................
42
Dosagem de alanina aminotransferase ..................................................................................
43
Marcadores sorológicos.......................................................................................................
43
Extração e amplificação parcial do gene S – fragmento de 417 pb.....................................
43
Carga viral - Titulação do DNA HBV................................................................................
43
Identificação dos fragmentos genômicos............................................................................
44
Reação de seqüenciamento..................................................................................................
44
Análise das seqüências.........................................................................................................
44
Análise dos dados................................................................................................................
45
Resultados............................................................................................................................
45
Discussão.............................................................................................................................
46
Referências…………….......................................................................................................
47
6.0 Versão em inglês do artigo I (Genotypic characterization of the hepatitis B
virus in Alagoas, Brazil)....................................................................................................
51
Abstract................................................................................................................................
51
Introduction..........................................................................................................................
52
Material and methods ..........................................................................................................
53
Study design and patient selection......................................................................................
53
Data and sample collection..................................................................................................
53
Alanine aminotransferase assay...........................................................................................
53
Serological markers.............................................................................................................
54
Extraction and S gene partial amplification - DNA fragment of 417 bp …………...…….
54
Viral load - Titration of the HBV DNA…………………..……………………………….
54
Identification of genomic fragments ……………..……………………………………….
55
Sequencing reaction.............................................................................................................
55
Analysis of the sequences...................................................................................................
55
Analysis .............................................................................................................................
55
Results.................................................................................................................................
55
Discussion...........................................................................................................................
56
References...........................................................................................................................
58
7.0 Artigo II (Mutações pré-core (1896) e BCP (1762/1764) no vírus da hepatite B
em pacientes de Alagoas, Brasil) .....................................................................................
62
Resumo................................................................................................................................
62
Introdução............................................................................................................................
63
Pacientes e métodos ............................................................................................................
64
Pacientes..............................................................................................................................
64
Dosagem de alanina aminotransferase ...............................................................................
64
Marcadores sorológicos......................................................................................................
64
Extração e amplificação parcial do gene S e região pré-core..............................................
64
Carga viral - Ttitulação do DNA HBV...............................................................................
65
Identificação dos fragmentos genômicos.............................................................................
65
Reação de seqüenciamento..................................................................................................
65
Análise das seqüências........................................................................................................
66
Resultados............................................................................................................................
66
Discussão.............................................................................................................................
68
Contribuição dos autores.....................................................................................................
68
Agradecimentos...................................................................................................................
68
Financiamento.....................................................................................................................
68
Conflito de interesses...........................................................................................................
68
Aprovação ética...................................................................................................................
68
Referências..........................................................................................................................
68
8.0 Versão em inglês do artigo II (Pre-core mutation (1896) and BCP (1762/1764) in
the hepatitis B virus in patients of Alagoas, Brazil) ………………………………….
74
Abstract...............................................................................................................................
74
Introduction.........................................................................................................................
75
Patients and methods ..........................................................................................................
76
Patients................................................................................................................................
76
Alanine aminotransferase assay …….................................................................................
76
Serological markers.............................................................................................................
76
Extraction and amplification of the S gene and precore region …………….…….……...
76
Viral load - Titration of the HBV DNA…………………………………………………..
77
Identification of genomic fragments.………………………………………….………….
77
Sequencing reaction............................................................................................................
78
Analysis of the sequences...................................................................................................
78
Results.................................................................................................................................
78
Discussion...........................................................................................................................
80
The authors’ contributions..................................................................................................
82
Ethical approval...................................................................................................................
82
Acknowlegments.................................................................................................................
82
Funding...............................................................................................................................
82
Conflicts of interest.............................................................................................................
82
References...........................................................................................................................
82
9.0 Conclusões.....................................................................................................................
86
10.0 Recomendações...........................................................................................................
87
Referências..........................................................................................................................
88
Apêndices ..........................................................................................................................
97
A. Termo de compromisso livre e esclarecido....................................................................
98
B. Questionário....................................................................................................................
100
Anexos ................................................................................................................................
102
A. Carta de aprovação do Comitê de Ética em Pesquisa.....................................................
103
B. Instructions authors – Memórias do Instituto Oswaldo Cruz.........................................
104
C. Guide for authors – Transactions of The Royal Society of Tropical Medicine and
Hygiene...............................................................................................................................
111
D. Comprovante de submissão do artigo I ao periódico Memórias do Instituto Oswaldo
Cruz.....................................................................................................................................
120
E. Comprovante de submissão do artigo II ao periódico Transactions of The Royal
Society of Tropical Medicine and Hygiene.........................................................................
121
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
APRESENTAÇÃO
A variação genética do vírus da hepatite B (HBV) é responsável pela emergência de
quasispecies virais em um mesmo paciente ao longo do curso de uma infecção crônica. Essa
característica viral mostra a necessidade de estudos moleculares objetivando determinar o perfil
genético do HBV, incluindo a identificação dos genótipos, relevantes no âmbito da epidemiologia
molecular; a pesquisa de mutações, visando variantes que escapam da imunização por meio da
vacina e/ou que modulam a secreção de HBeAg e a carga viral para indicar e monitorar o
tratamento com drogas antivirais.
No Brasil, os estudos de caracterização do HBV são escassos, principalmente em relação à
região Nordeste e em especial ao estado de Alagoas, motivo pelo qual foi realizada a presente
pesquisa.
Como professora da disciplina de Imunologia e Virologia da Universidade Federal de
Alagoas (UFAL), sempre tivemos interesse pelo diagnóstico laboratorial das infecções virais.
Com o HBV, iniciamos pesquisando HBsAg, ainda pelo método de hemaglutinação passiva
reversa em gestantes, com a finalidade de detectar portadoras assintomáticas da infecção. O
projeto envolveu também, o estudo da eventual ocorrência de transmissão materno-infantil com o
objetivo de indicar à Secretaria de Saúde os casos de crianças necessitando imunização ativa e
passiva. Com o resultado da pesquisa, a sorologia para o referido marcador viral foi incluída na
rotina de pré-natal do Hospital Universitário Prof. Alberto Antunes/UFAL. Além disso, a pesquisa
chamou atenção para a imunização dos recém-nascidos filhos de mães portadoras do HBsAg.
Paralelamente, fui responsável pela criação do Setor de Imunodiagnóstico do Laboratório
de Análise Clínicas, do Hospital Universitário e na ocasião implantamos o ensaio
imunoenzimático (ELISA) para o diagnóstico laboratorial da hepatite B, sendo posteriormente
estendido para outras patologias de etiologias distintas. Participei ainda de outras pesquisas
envolvendo a infecção pelo HBV como a identificação dos subtipos do HBsAg, por imunodifusão
radial e a detecção dos marcadores HBsAg/anti-HBs, anti-HBc e HBeAg/anti-HBe em portadores
de esquistossomose mansônica.
Por motivos circunstanciais, no Mestrado trabalhei com a técnica de imunofluorescência
indireta para o diagnóstico das infecções respiratórias pelos vírus, influenza A e B, parainfluenza
tipos 1,2 e 3, sincicial respiratório e adenovírus, em crianças.
Para o tema do Doutorado retomei minha antiga paixão buscando ampliar o diagnóstico
laboratorial
das
infecções
pelo
HBV
em
Alagoas.
Partindo
dos
marcadores
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
sorológicos, como critério de seleção das amostras, pesquisamos as características genéticas do
vírus para responder a pergunta condutora do estudo: Qual o perfil genético do vírus da hepatite B
que circula em Alagoas?
A pesquisa contou com diversas parcerias institucionais e o apoio financeiro foi oriundo
da FINEP pelo Programa INOVA-ALAGOAS e da Fundação de Amparo à Pesquisa do Estado de
Alagoas-FAPEAL, por meio da concessão de uma Bolsa de Doutorado.
A parceria com o Instituto Adolfo Lutz de São Paulo permitiu a realização de
treinamentos no Laboratório de Hepatites Virais, sob a supervisão da co-orientadora Dra. Regina
Célia Moreira, para padronização dos procedimentos moleculares. O desenvolvimento da pesquisa
ocorreu nos seguintes locais: Laboratório de Biotecnologia do Centro de Ciências Agrárias da
UFAL, Setor de Imunodiagnóstico do Laboratório de Análises Clínicas do Hospital Universitário,
ambos da UFAL e Setor de Virologia do Laboratório de Imunopatologia Keizo-Asami (LIKA) da
Universidade Federal de Pernambuco (UFPE).
A pesquisa foi iniciada com a realização de reuniões para apresentação do projeto,
contando com o apoio de médicos infectologistas e hepatologistas dos Centros de Referências em
Hepatites Virais do Estado. Devido à ausência do diagnóstico molecular em Alagoas, o projeto
teve uma excelente aceitação por parte dos pacientes, não ocorrendo nenhum caso de recusa.
Por fim, o envolvimento das referidas instituições foi fundamental, uma vez que
proporcionou a formação de um grupo de pesquisa interinstitucional com a possibilidade de
realizar novos projetos.
A tese está apresentada na forma de dois artigos, registrando pela primeira vez em
Alagoas estudos moleculares da infecção pelo HBV. O primeiro artigo trata da “Caracterização
genotípica do vírus da hepatite B em Alagoas, Brasil”, submetido ao periódico Memórias do
Instituto Oswaldo Cruz e o segundo com o título “Mutações pré-core (1896) e região basal do
promotor core (1762/1764) no vírus da hepatite B em pacientes de Alagoas, Brasil”, enviado para
publicação no Transactions of The Royal Society of Tropical Medicine and Hygiene.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
20
1.0 REVISÃO DA LITERATURA
O vírus da hepatite B pertence à família Hepadnaviridae, gênero Orthohepadnavírus, por
ser DNA e infectar preferencialmente hepatócitos (NORDER et al., 1992). Com base em uma
variação nucleotídica, definida arbitrariamente em igual ou superior a 8%, na seqüência completa
do genoma viral, foram descritos oito genótipos denominados de A – H, com prevalências
distintas em diferentes áreas geográficas (OKAMOTO et al., 1988; NORDER et al., 1992;
STUYVER et al., 2000; ARAUZ-RUIZ et al., 2002).
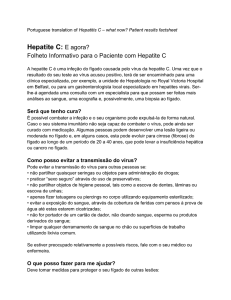
O vírion, denominado de partícula Dane, com 42 nm de diâmetro, é constituído por um
nucleocapsídeo icosaédrico envolvido por um envelope (Figura 1).
Figura 1. Estrutura do vírus da Hepatite B
(http://images.google.com.br/images?hl=pt-BR&q=virus+hepatite+b&gbv=2&aq=0&oq=v%C3%ADrus+hepatite+B)
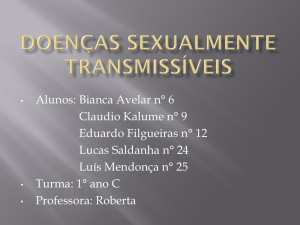
Na microscopia eletrônica, além do vírion, são visualizadas formas esféricas e
filamentosas, de vários comprimentos, com 22 nm de diâmetro, constituídas apenas de lipídios e
principalmente de proteínas do envelope viral e por isso não são infecciosas (MAHONEY, 1999)
(Figura 2). Em alguns casos de infecções crônicas essas formas estão presentes em quantidades
excessivas, dez mil a um milhão de vezes o número de partículas infecciosas (TIOLLAIS;
POURCEL; DEJEAN, 1985; WORLD HEALT ORGANIZATION, 2002).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
21
Figura 2. Microscopia eletrônica do vírus da hepatite B.
(Collier; Oxford, 2000)
O genoma completo apresenta-se com uma conformação circular, constituída de fita
parcialmente dupla de DNA. A fita negativa é completa, representando o comprimento da
unidade, em torno de 3200 nucleotídeos, enquanto a fita positiva tem uma diferença de
aproximadamente 700 nucleotídeos em comprimento (COLLIER; OXFORD, 2000). Sua
organização é altamente compacta, seqüências comuns são compartilhadas por genes distintos e
elementos reguladores, como promotores e acentuadores de transcrição. As proteínas virais
são codificadas por quatro matrizes de leitura aberta (ORF - open reading frame) superpostas,
denominadas de pré-S/S; pré-C/C; P e X. (TIOLLAIS; POURCEL; DEJEAN, 1985). Esse tipo de
organização é tão significante que a proteína estrutural HBsAg é codificada por uma seqüência
representativa da porção central do gene P (CLARKE; BLOOR, 2002) (Figura 3).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
22
Figura 3. Genoma do vírus da hepatite B e proteínas codificadas
(Murray; Rosenthal; Pfaller, 2006)
A região pré-S/S tem uma organização complexa, apresentando dois códons internos de
iniciação. É responsável pelas glicoproteínas do envelope viral, pré-S1, pré-S2 e S, denominadas
respectivamente de L (large), M (middle) e S (small), principal antígeno de superfície do HBV
(HBsAg) (GANEM, 1996). A região pré-C/C, possui também, uma organização similar e codifica
as proteínas, HBcAg (antígeno do capsídeo do HBV) e HBeAg (antígeno “e” do HBV) (KONG;
HONG; LEE, 2000). O gene P ocupa 70% do genoma completo e codifica um complexo
multifuncional, cujos domínios incluem uma proteína terminal e enzimas com atividades de DNA
polimerase, transcriptase reversa (RT) e ribonuclease H. A região X codifica a proteína HBx, cuja
função está associada à regulação de promotores virais e celulares (CLARKE; BLOOR, 2002).
A proteína HBsAg é codificada pelo gene S, a partir do segundo códon interno de
iniciação, posição 155, região classicamente utilizada para discriminar genótipos virais. É um
polipeptídeo de 226 aminoácidos de comprimento, sintetizado tanto na forma glicosilada, com
carboidratos N-ligados (gp 27), quanto na forma não glicosilada (p 24). Suas propriedades
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
23
antigênicas e imunogênicas dependem da sua conformação dimérica unida por pontes
dissulfídricas (ZHENG et al., 2002).
A proteína L é codificada pelas regiões pré-S1, pré-S2 e S, iniciando pelo primeiro códon
AUG, posição 2854, da região pré-S/S. É sintetizada em duas isoformas, uma glicosilada (gp 42)
e a outra não glicosilada (p39). A proteína M é codificada pelas regiões pré-S2/S, a partir do
segundo códon AUG, posição 3211. É sintetizada em duas formas glicosiladas (gp33 e gp36) e
contém um receptor para albumina humana polimerizada, presente também, nos hepatócitos
(WONG; NATH; SNINSKY, 1985).
Um vírion contém entre 300-400 moléculas de HBsAg e 40 a 80 moléculas M e L, tendo
as formas filamentosas uma composição idêntica, enquanto as formas esféricas apresentam 20
vezes menos a proteína L (TIOLLAIS; POURCEL; DEJAN, 1985).
O HBsAg apresenta nove subtipos sorológicos, caracterizados por um determinante
antigênico de grupo (denominado a), entre os resíduos de aminoácidos 124 e 147, por pares de
determinantes alélicos, d ou y, posição 122 e r ou w, posição 160 (BANCROFT et al., 1972),
pelos
sub-determinantes de w; w1, w2, w3 e w4 (MAGNIUS; ESPMARK, 1972) e pelo
determinante q, encontrado em todas as especificidades de HBsAg, com exceção de adw4 (adwq-)
e em algumas adr (adrq-). De acordo com essas características antigênicas foram definidos como
ayw1, ayw2, ayw3, ayw4, ayr, adw2, adw4, adrq- e adrq+. As divergências intragenotípicas
variam entre 0,1 a 7,4% (ARAUZ-RUIZ et al., 2002). O determinante “a” é reconhecido pelo
anticorpo contra o HBsAg (Anti-HBs), o qual confere imunidade contra todos os subtipos,
enquanto os anticorpos para os determinantes de subtipos não conferem proteção (MAHONEY,
1999). Estes subtipos apresentam distribuições geográficas distintas e por isso são úteis como
marcadores epidemiológicos (COUROUCÉ-PAUTY et al., 1978). No Brasil, já foram
identificados ayw1, ayw2, ayw3, adw2, adw4 e adr, (MORAES et al., 1996; RIBEIRO et al.,
2006; OLIVEIRA et al., 2008).
Vários genótipos são sorotipicamente heterogêneos. Os genotipos A e B contêm os
subtipos ayw1 e adw2, o genotipo C, subtipos adw, adr e ayr, o genotipo D, subtipos ayw2, ayw3
e ayw4. Os genótipos E, F e G, foram descritos com apenas um sorotipo, correspondendo aos
subtipos ayw4, adw4 adw2, respectivamente (NORDER et al., 1992; STUYVER et al., 2000;
KIDD-LJUNGGREN; MIYAKAWA; KIDD, 2002) e o genótipo H sendo filogeneticamente
relacionado
ao
genótipo
F
(ARAUZ-RUIZ
et
al.,
2002).
A proteína HBcAg, principal componente estrutural do nucleocapsídeo viral é o
polipeptídeo mais conservado entre os hepadnavírus de mamíferos. É uma fosfoproteína
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
24
básica de 21 kd. Sua transcrição é iniciada no códon AUG mais interno, posição 1901, da região
pré-C/C, enquanto a proteína HBeAg é um produto de transcrição que se inicia no primeiro códon
AUG, posição 1814, sendo sintetizada como um precursor pré-core que é clivado durante o
processo de maturação, perdendo o sinal (pre-C) e a seqüência carboxiterminal (YEN, 1993;
NORDER; COUROUCÉ; MAGNIUS, 1994). Resultando uma proteína de 16-18 kda que é
intensamente secretada pela célula e detectada no soro como um antígeno imunologicamente
distinto associado com replicação viral ativa (BRUNETO et al., 1990; WORDL HEALTH
ORGANIZATION,2002).
A proteína P, ou polimerase viral, é uma proteína estrutural encontrada ligada ao terminal
5´ do DNA viral, atuando como um oligonucleotídeo iniciador (primer). É responsável pela
síntese da cadeia negativa do DNA viral a partir do RNA pré-genômico, atividade de transcriptase
reversa e também, pela síntese da cadeia positiva, atividade de DNA polimerase. Como essas
etapas são essenciais para o ciclo de replicação viral, a atividade dessa enzima é o principal alvo
da quimioterapia antiviral a base de análogos de nucleosídeos (CLARKE; BLOOR, 2002).
A proteína HBx não é estrutural, possui peso molecular de 17 kd e sua síntese resulta da
alta expressão do gene X. Sua função está diretamente associada ao processo de transcrição,
atuando como um regulador transcricional em geral. Seu mecanismo de ação envolve tanto
interações com fatores celulares que se ligam especificamente a elementos reguladores, presentes
no DNA como interações com componentes da via de transdução de sinal, podendo afetar
indiretamente a expressão genética do vírus e do hospedeiro. Desse modo HBx tem uma função
essencial na replicação e na carcinogênese hepatocelular (KONG; HONG; LEE, 2000; AHN et
al., 2001).
O sítio primário de replicação do HBV é o fígado. Esse tropismo é determinado pelo
elevado nível de transcrição da célula hepática. A qual disponibiliza fatores de transcrição que
interagem simultaneamente com o promotor do gene core e seqüências virais acentuadoras (E1),
favorecendo a transcrição do RNA pré-genômico, etapa central do ciclo viral, caracterizando um
processo não citolítico (ZHANG; MCLACHLAN, 1994).
A adsorção viral ocorre por meio da interação entre a proteína pré-S1 e um receptor
celular, seguido da fusão de membranas. O DNA viral é carreado para o núcleo celular, onde é
convertido em moléculas circulares covalentemente fechadas (cccDNA, covalenty closed
circular DNA), tornando-se ativo para a transcrição pela RNA polimerase II. O processo de
transcrição é controlado pelos promotores, pré-S1, pré-S2, core e X e por E1 e E2. A
ZAIDAN, A.M. E.
25
Caracterização genética do vírus da hepatite B...
transcrição das proteínas do envelope está associada aos promotores pré-S1 e pré-S2, do RNA
pré-genômico com o promotor core e da proteína X com o promotor X (MAHONEY, 1999;
KONG; HONG; LEE, 2000). O RNA pré-genômico é o mensageiro para as proteínas précore/core (HBeAg, HBcAg) e polimerase. Após ser encapsulado pelas proteínas core, junto com a
DNA polimerase, constituindo o capsídeo viral, funciona como molde para a replicação do
genoma viral pela polimerase viral, por meio de um mecanismo de transcrição reversa. Em
infecções crônicas, um pool de cccDNA é mantido no núcleo do hepatócito. Integrações
aparentemente aleatórias do genoma viral ocorrem comumente, representando uma etapa
importante no processo oncogênico (YEN, 1993; WORLD HEALTH ORGANIZATION, 2002).
As infecções pelo HBV tendem a apresentar um curso extremamente variável em função
do grau de reatividade imunológica do hospedeiro estimulado pelos antígenos virais. São descritos
três padrões clínicos distintos que se distribuem equitativamente em infecções sub-clínicas,
sintomáticas com manifestações clínicas leves, sem icterícia e doenças hepáticas severas, onde
pode ocorrer hepatite fulminante em 0,5% dos casos (BOAG, 1991). As infecções persistentes
ocorrem em 10% dos adultos e em 70 - 90% das crianças que adquiriram a infecção por via
vertical de mãe HBeAg positivas. Em geral, o aumento da idade está relacionado com infecções
sintomáticas que favorecem a cura viral (MCMAHON; ALBERTS, WAINWRIGHT, 1990;
HOLLINGER, 1996; LAI et al., 2003).
Na infecção crônica são descritas as seguintes fases: tolerância imunológica caracterizada
pela ausência de resposta imune refletida pelo HBeAg positivo, alta carga viral e histologia
hepática com tendência a normalidade; imunoeliminação, marcada pela soro-conversão do
HBeAg para antiHBe, inflamação hepática, fibrose e flutuações no nível sérico da ALT e a fase
residual, também conhecida como não replicativa, definida pela baixa viremia, ALT normal e
ausência de inflamação hepática, podendo perdurar por toda a vida. No entanto, ao longo da fase
residual, podem ocorrer reversão para o estado HBeAg positivo em decorrência do grau de
reatividade imunológica do hospedeiro ou atividade viral causada pela seleção de mutantes da
região pré-core e do HBsAg que escapam da imunovigilância (MENDONÇA; VIGANI, 2006).
A tolerância imunológica comumente é observada em crianças e adolescentes que
adquiriram a infecção no período neonatal ou perinatal, podendo perdurar por 15 a 35 anos. Essa
condição se aplica geralmente às populações asiáticas e africanas. Provavelmente é devida a
passagem transplacentária do HBeAg da mãe para o feto, durante a gestação. Enquanto nas
regiões
onde
a
infecção
é
adquirida
a
partir
da
adolescência,
geralmente
pelo
contato sexual ou pelo uso de drogas intravenosas, não ocorre a referida fase de tolerância. A
infecção evolui com soro-conversão do HBeAg e baixa concentração de DNA HBV, geralmente <
104 cópias/mL (LAI et al., 2003).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
26
Manifestações extra hepáticas associadas às infecções pelo HBV são observadas entre
10% a 20% dos pacientes e parecem ser causadas por complexos imunes circulantes. As mais
comuns incluem uma síndrome semelhante à doença do soro, poliarterite nodosa,
glomerulonefrite membranosa e uma acrodermatite papular infantil, conhecida como síndrome
Gianoti-Crosti (MCMAHON; ALBERTS; WAINWRIGHT, 1990).
Os genótipos podem influenciar as características do vírus, como mutações e carga viral e
da infecção, como o tempo de soro-conversão do HBeAg, desenvolvimento de carcinoma
hepatocelular (CHC) e resposta ao tratamento com interferon.
As infecções pelo genótipo B tem probabilidade de soroconversão do HBeAg com uma
década de antecedência e níveis mais baixos de ALT, quando comparadas às infecções pelo
genótipo C (YUEN et al., 2004), o qual apresenta maior freqüência de mutações na região basal
do promotor core (BCP) e baixa resposta à terapia com interferon em relação ao genótipo B (KAO
et al., 2000).
Na Índia, onde A e D são prevalentes, as infecções pelo genótipo A apresentaram maior
freqüência de ALT elevada, positividade HBeAg e presença de cirrose (KUMAR et al., 2005).
Embora, em outro estudo, THAKUR et al. (2002) mostraram que as infecções pelo genótipo D
estão associadas com doença hepática mais severa podendo predizer a ocorrência de CHC em
pacientes jovens.
Em um estudo envolvendo os genótipos A, D e F, a soroconversão do HBeAg não
mostrou relação com os referidos genótipos. No entanto, após a soroconversão, as infecções pelo
genótipo A apresentaram taxa de eliminação do DNA HBV mais alta e com o genótipo F a
mortalidade relacionada com doença hepática foi mais freqüente (SANCHEZ-TAPIAS et al.,
2002).
A variação genética do HBV é devida, em parte, à falta de um mecanismo de revisão e
reparo envolvendo as atividades da DNA polimerase, durante o processo de transcrição reversa do
RNA pré-genômico, favorecendo o aparecimento de mutações pontuais, deleções ou inserções
(SUMMER; MASON, 1982). Naturalmente são encontradas variantes das regiões pré-S/S, préC/C e P, resultando populações de vírus com genomas heterogêneos, denominados por
quasispecies (STUYVER et al., 2000). As mutações com substituições de nucleotídeos são mais
freqüentes nas regiões compartilhadas entre as ORFs e variam com as diferentes regiões
genômicas, estimando-se uma taxa de mutação entre 1,4 a 3,2 x 10-5 substituições por sítio/ano
(BALLARD;
BOXALL,
1997;
ARAUZ-RUIZ
et
al.,
2002;
KIDD-LJUNGGREN; MIYAKAWA; KIDD, 2002). Devido às sobreposições de seqüências
gênicas, mais de um gene do DNA viral pode ser alterado, resultando mutantes não viáveis ou
competentes para a replicação viral (GANEM, 1996; SOMMER; VAN BÖMMEL; WILL, 2000;
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
27
CLARKE; BLOOR, 2002). As mutações nas regiões pré-S/S e pré-C/C estão descritas como
fatores responsáveis pelo controle da atividade viral, secreção de vírion e expressão do HBeAg
(TONG, 2005). As mutações no gene da polimerase estão associadas com resistência aos
quimioterápicos antivirais como a lamivudina e outros análogos de nucleosídeos ( STUYVER;
VAN GEYT; DE GENDT, 2000).
A variabilidade genética do HBV, foi documentada inicialmente em estudos que
caracterizaram os subtipos do HBsAg, refletindo uma substituição de G para A nas posições 365
e 479 do gene S. No HBsAg, corresponde, respectivamente, às posições 122, para os
determinantes, d ou y e 160, para r ou w. Em ambas às posições, o aminoácido lisina (K) define os
determinantes d e w, enquanto o aminoácido arginina (R) os determinantes y e r (OKAMOTO et
al., 1988; NORDER et al., 1992).
Mutantes do HBsAg com vários tipos de substituições de aminoácidos dentro do
determinante “a” são imunogênicos, porém podem ter sua especificidade alterada e por
conseguinte são capazes de escapar do controle imune. Essas substituições reduzem a afinidade de
ligação entre o HBsAg e o anticorpo específico, tornando o HBV resistente à neutralização pelo
anti-HBs. Particularmente, a substituição de glicina por arginina no códon 145 (G145R) altera a
conformação do determinante “a” induzindo anticorpos com uma especificidade alterada que não
se ligam eficientemente ao HBsAg “selvagem”. Esses tipos de mutantes do HBV são encontrados
naturalmente em portadores crônicos, especialmente em filhos de mães HBsAg positivas, que
foram imunizados com HBsAg e em receptores de transplante hepático que receberam
imunoglobulina específica como imunoprofilaxia (ZHENG et al., 2004).
Na junção pré-C/C tem sido detectados vários pontos de mutações, com substituições de
nucleotídeos. A substituição G para A na posição 1896 (G1896A) é a mais comum. Esse tipo de
mutação dá origem a um códon de terminação prematuro na extremidade da região pré-C,
bloqueando a síntese do HBeAg. A presença de timina no nucleotídeo (nt) 1858, formando um par
de bases (A-T) com a adenina do nucleotídeo 1896, torna o sinal de encapsidação do RNA prégenômico mais forte, aumentando a eficiência da replicação, apesar da presença de anti-HBe. Nos
genótipos B, C, D e E, a presença de timina no nt 1858 é mais freqüente enquanto nos genótipos
A e H geralmente é detectado citosina. No F pode ser encontrado timina ou citosina. (LI et al.,
1993; LI et al., 2001). Justificando a maior freqüência dessa mutação nos genótipos B, C, D, E e
F, onde as infecções pelo HBV apresentam ausência de HBeAg e replicação viral ativa, apesar da
presença de anti HBe (CHU; HUSSAIN; LOK, 2002; YOTSUYANAGI et al., 2002). Sendo
frequentemente encontradas nos países do Mediterrâneo e Ásia Oriental e geralmente está
associada com doença hepática severa, remissão espontânea rara e uma pobre resposta ao
interferon (BRUNETO et al., 1990; OKAMOTO et al., 1990). O genótipo G abriga naturalmente
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
28
1896A e 1858T, e por isso as infecções por esse genótipo são incapazes de expressar HBeAg
(KATO et al., 2002).
As mutações na região basal do promotor core (BCP), A1762T e G1764A são descritas
em diferentes genótipos (SITNIK et al., 2004; CANDOTTI et al., 2006; CHAUHAN et al., 2006)
a despeito da soroconversão do HBeAg (OKAMOTO et al., 1994; BOZDAYI et al., 2001). A
ocorrência dessas mutações sozinhas ou acompanhadas da mutação pré-core G1896A, tem sido
associada com hepatite B crônica ativa em infecções HBeAg negativo/anti-HBe positivo
(OKAMOTO et al., 1994; HONDA et al., 1999). Quando associadas com outras mutações
(T1753C, C1766T e T1768A), que ocorrem naturalmente nessa região, afetam a capacidade de
replicação do HBV (SATO et al., 1995; CHANG et al., 2004; JAMMEH et al., 2008). São
consideradas um fator viral independente de risco para prognosticar o desenvolvimento do
carcinoma hepatocelular, podendo ser detectadas com nove anos ou mais de antecedência do
diagnostico histopatológico (CHOU et al., 2008; TONG et al., 2007). Em portadores
assintomáticos, que apresentam níveis elevados de ALT, porém ainda dentro da faixa de
normalidade, podem significar um marcador sensível para se prever hepatites insidiosas
(TAKAHASHI et al., 1995).
As mutações no gene da polimerase estão associadas com alterações no domínio catalítico
"YMDD" da DNA polimerase, devido principalmente, às substituições de metionina por valina no
códon 552 (M552V) ou por isoleucina (M552I) e geralmente, são acompanhadas por uma
mudança de leucina para metionina no códon 528 (L528M), conferindo aos vírus mutantes
resistência aos análogos de nucleosídeos como a lamivudina (STUYVER; VAN GEYT; DE
GENDT, 2000).
O diagnóstico da infecção pelo HBV é realizado geralmente pela pesquisa dos marcadores
sorológicos da infecção viral, HBsAg, HBeAg, anti-HBs, anti-HBe (anticorpo contra o antígeno
“e” do HBV) e anti-HBc (anticorpo contra o antígeno do capsídeo do HBV), por meio de métodos
imunológicos. Os ensaios imunoenzimáticos (ELISA) são freqüentemente empregados e baseiamse na interação entre epitopos das proteínas virais e seus respectivos anticorpos específicos. No
tecido hepático, o HBsAg e o HBcAg podem ser detectados por meio de técnicas moleculares,
como hibridização in situ (COLLIER; OXFORD, 2000).
No curso natural da infecção pelo HBV, o HBsAg pode ser detectado, ainda no período de
incubação, seguido logo depois do HBeAg. A reatividade do soro é revelada inicialmente pela
presença
de
anti-HBc
e
em
seguida
de
anti-HBe,
significando
que o processo está evoluindo para a cura, mesmo que o HBsAg ainda esteja presente. A presença
de anti-HBc IgM no soro está associada à infecção aguda ou recente, enquanto que o anti-HBs é
revelado tardiamente, indicando recuperação completa e imunidade às reinfecções (MAHONEY,
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
29
1999). No entanto, a presença de anti-HBs nem sempre indica ausência de infecção, uma vez que
o DNA viral pode ser detectado em soros anti-HBc e anti-HBs positivos (ARRAES et al., 2003).
A persistência de antígenos virais após a fase aguda e evolução para a forma crônica está
associado à variação genética do vírus e à competência imunológica do hospedeiro (COLLIER;
OXFORD, 2000).
Os métodos moleculares são importantes para avaliar clinicamente a evolução da infecção
e a resposta ao tratamento com drogas antivirais, porém, esses métodos não fazem parte da rotina
dos testes laboratoriais empregados no diagnóstico da infecção pelo HBV na maioria dos Centros
de Referências do país (LYRA et al., 2005; MELLO et al., 2007). A detecção no soro do DNA
HBV pela reação em cadeia da polimerase (PCR) é um método sensível e específico para detectar
a infecção viral, investigar genótipos, mutações e a carga viral.
A identificação dos genótipos do HBV pode ser obtida pelo estudo de uma seqüência
parcial do genoma viral, como a região pré-S ou S e os métodos mais utilizados são:
seqüenciamento direto, polimorfismo do tamanho dos fragmentos de restrição (RFLP – restriction
fragment lenght polymorphism), teste de hibridização com sondas (LIPA Line Probe Assay -) e
ELISA (CHU; HUSSAIN; LOK, 2002). As mutações são investigadas pela amplificação e
seqüenciamento das regiões pré-S/S, pré-core/core e da polimerase (P) do genoma viral (SITNIK
et al., 2004).
A carga viral pode ser estimada pela titulação do DNA HBV por meio da amplificação de
um fragmento de 270 pb da região core. A sensibilidade dos ensaios variam entre 200 a 300
cópias/mL (ANJOS et al., 2001). Resultados abaixo do limite de detecção podem ser justificados
nos pacientes que receberam tratamento com lamivudina e ou interferon (LAI et al., 2003) e
também, em infecções crônicas que apresentam as formas esféricas e tubulares em quantidade
excessiva, dez mil a um milhão de vezes o número de partículas infecciosas (TIOLLAIS;
POURCEL; DEJEAN, 1985).
Em relação ao tratamento da hepatite B crônica estão disponíveis comercialmente,
Interferon Alfa, Interferon Peguilado Alfa 2a, por sua ação antiviral, antiproliferativa e
imunomoduladora (HOU et al., 2001) e análogos de nucleosídeos, como Lamivudina, Adefovir
dipivoxil e Entecavir pela supressão viral, bloqueando a atividade de transcriptase reversa da
DNA polimerase viral, embora não erradiquem a infecção (LAI et al., 2003).
A Lamivudina é bem tolerada durante período prolongado e contínuo de terapia, porém o
principal problema é o aparecimento de variantes resistentes, devido às mutações no domínio
YMDD, responsável pela atividade de transcriptase reversa (DA SILVA et al., 2001). Com o
Adefovir e o Entecavir esse problema é menor, sendo, portanto indicados em pacientes resistentes
a Lamivudina (LEUNG et al., 2001; ARAÚJO; BARONE, 2006).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
30
Os genótipos B e A respondem melhor ao tratamento com interferon quando comparados
aos genótipos C e D (HOU et al., 2001). Enquanto as respostas com os análogos de nucleosídeos
aparentemente não mostram nenhuma relação com os genótipos (ARAÚJO; BARONE, 2006).
A erradicação mundial da infecção pelo HBV por meio de vacinas é uma possibilidade
(LAI et al., 2003). Atualmente é recomendado o uso de vacinas recombinantes produzidas a partir
da clonagem do gene S do HBV em vetores plasmidiais que são posteriormente inseridos em
células de leveduras para produção de HBsAg (TURNER et al., 2004). A administração pode ser
feita em qualquer idade e simultaneamente com outras vacinas do calendário. A transmissão
vertical pode ser reduzida em até 95% por meio da vacinação dos recém-nascidos de mães HBsAg
positivas, imediatamente após o parto (nas primeiras 12 horas), obedecendo o esquema, 0, 1 e 6
meses, associado à imunoglobulina específica contra hepatite B (IGHB) (MINISTÉRIO DA
SAÚDE, 2001).
Os portadores crônicos da infecção pelo HBV estão mundialmente distribuídos entre áreas
de baixa prevalência, com taxas de 0,1 a 2 % e áreas de alta prevalência com positividade entre 10
a 20%. O risco de evoluir para infecção crônica está relacionado com a idade em que a infecção é
adquirida (LUSIDA et al., 2003). Em regiões de baixa ou média endemicidade, a infecção ocorre
principalmente entre adolescentes e adultos jovens enquanto nas regiões de alta prevalência,
ocorre geralmente no período neonatal ou no início da infância (LAI et al., 2003; ARAÚJO et al.,
2004).
Como regiões de alta endemicidade, são considerados o Extremo Oriente (Sul da Ásia,
China, Filipinas, Indonésia), Oriente Médio, África sub-Sahariana e bacia Amazônica. As regiões
de prevalência intermediária incluem o Japão, áreas da América do Sul, Sudeste da
Europa e partes da Ásia Central. As áreas de baixa endemicidade abrangem os Estados Unidos,
Canadá, Norte da Europa, Austrália e áreas da América do Sul (PARANÁ; ALMEIDA, 2005;
TENGAN; ARAÚJO, 2006; WORLD HEALTH ORGANIZATION, 2009).
O padrão de distribuição genotípica pode variar em função da geografia, refletindo a etnia
da população. O genótipo A é mais freqüente no Noroeste Europeu, África Central e Américas
(STUYVER et al., 2000; CHU; HUSSAIN; LOK, 2002). Os genótipos B e C no Sudeste Asiático,
China e Japão (YOTSUYANAGI et al., 2002; YUEN et al., 2004; CHOU et al., 2008). O
genótipo D predomina no Sul Europeu, Oriente Médio e Índia (BOZDAYI et al., 2001; OLYAEE
et al., 2005; CHAUHAN et al., 2006), enquanto o genótipo E é encontrado principalmente na
parte Ocidental da África (CANDOTTI et al., 2006). O genótipo F é encontrado em populações
aborígenes das Américas e na Polinésia (NORDER et al., 1996; DEVESA et al., 2004). O
genótipo G foi detectado na França, nos Estados Unidos (STUYVER et al., 2000), no México
(SÁNCHEZ et al., 2002) e no Brasil (BOTTECCHIA et al., 2008), sendo encontrado
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
31
freqüentemente em co-infecção com o genótipo A (KATO et al., 2002) e o genótipo H foi descrito
na Nicarágua, México, Estados Unidos (ARAUZ-RUIZ et al., 2002; SCHAEFER, 2005) e Brasil
(BERTOLINI et al., 2004).
No Brasil, os registros dos portadores da infecção crônica, tendo como base resultado
positivo para HBsAg, mostram uma distribuição heterogênea entre baixa endemicidade,
(MIRANDA et al., 2000; MACHADO; ZURAVSKI, 2007; MIYAMOTO; BERTOLINI; 2008), a
alta endemicidade, na região Amazônica (TAVARES-NETO et al., 2004; VIANA et al., 2005;
KHOURI et al., 2005; PARANÁ; ALMEIDA, 2005).
A distribuição genotípica pode variar em função da composição étnica da população de
estudo. Refletindo o modo de colonização e expansão do território brasileiro, com redução da
população indígena. Sendo também, importante ressaltar a influência das correntes migratórias
que favoreceram novos contatos étnicos e culturais.
O genótipo A é predominante no Brasil (ARAÚJO et al., 2004; SITNIK et al., 2004;
MOTTA-CASTRO et al., 2005; OLIVEIRA et al., 2008) e o genótipo F é mais freqüente na
população indígena da região amazônica (VIANA et al., 2005). Os genótipos B e C estão
descritos, com maior freqüência, em populações de etnia asiática (SITNIK et al., 2004), enquanto
o D em indivíduos de origem italiana, freqüentes nas regiões Sudeste, Sul e Centro-Oeste do país
(TELES et al., 2002; CARRILHO et al., 2004; PARANÁ; ALMEIDA, 2005; SITNIK et al., 2004;
REZENDE et al., 2005).
De um modo geral, pelo menos dois dos genótipos A, D e F co-circulam em diferentes
regiões brasileiras (MELLO et al., 2007). O genótipo H foi detectado no Paraná em 2004 sendo
também a primeira vez na América do Sul (BERTOLINI et al., 2004) e junto com o genótipo F
são autóctones das Américas (DEVESA et al., 2004). O genótipo B foi detectado em pacientes
asiáticos por Sitnik et al. (2004) em estudo envolvendo pacientes de várias regiões do país e por
Ribeiro et al. (2006) em Salvador. O genótipo C foi identificado em alta freqüência em pacientes
asiáticos por Sitnik et al. (2004) e em baixa freqüência por Bottecchia et al. (2008), no Rio de
Janeiro e por Oliveira et al. (2008), na região amazônica. O único caso de infecção pelo genótipo
E foi identificado em um paciente angolano residente em São Paulo (SITNIK et al., 2007).
Diante do exposto e devido à ausência de pesquisas no Estado de Alagoas, este trabalho
investigou a caracterização genética do HBV focalizando genótipos, mutações e carga viral.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
32
2.0 FORMULAÇÃO DA QUESTÃO DA PESQUISA
Qual o perfil genético do vírus da hepatite B detectado em pacientes atendidos nos
Centros de Referências em Hepatites Virais do Estado de Alagoas, durante o período de setembro
de 2006 a abril de 2008?
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
33
3.0 OBJETIVOS
3.1 Objetivo geral
Identificar o padrão genético do vírus da hepatite B em pacientes, com sorologia positiva
para HBsAg e anti-HBc, atendidos nos Centros de Referências em Hepatites Virais do Estado:
Hospital Universitário Prof. Dr. Alberto Antunes/Universidade Federal de Alagoas HUAA/UFAL e Hospital Escola Prof. Dr. Hélvio Auto/Universidade de Ciências da Saúde do
Estado de Alagoas – HEHA/UNCISAL, durante o período de setembro de 2006 a abril de 2008.
3.2 Objetivos específicos
¾ Detectar a infecção pelo HBV por meio da pesquisa do DNA viral em pacientes HBsAg e
anti-HBc reagentes e investigar a carga viral.
¾ Identificar os genótipos do HBV que estão circulando em Alagoas
¾ Detectar as mutações pré-core G1896A e BCP A1762T / G1764A e descrever sua
distribuição entre os genótipos identificados.
¾ Caracterizar as infecções quanto ao genótipo, as mutações, a carga viral, o perfil
HBeAg/anti-HBe e nível sérico de alanina aminotransferase (ALT), entre os portadores
assintomáticos e pacientes com hepatites aguda e crônica.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
34
4.0 METODOLOGIA
4.1 Desenho do estudo
Foi realizado um estudo transversal descritivo envolvendo pacientes dos Centros de
Referências em hepatites virais do Estado, durante o período de setembro-2006 a abril-2008. A
pesquisa foi aprovada pelo Comitê de Ética em pesquisa da UFAL segundo protocolo de pesquisa
nº. 000906/2005-98 em 16/03/2005.
Os estudos transversais são colocados de uma maneira geral como de baixo custo, porém,
este estudo revelou dados primários que foram obtidos por meio de investigações envolvendo
técnicas moleculares, como extração viral, amplificação por PCR, eletroforese de fragmentos
genômicos, reação de seqüenciamento e ferramentas de bioinformática para análises das
seqüências obtidas e por isso teve um custo elevado.
4.2 Definição do tamanho amostral
Para o cálculo do tamanho amostral foi utilizado o programa Epi Info versão 6, com os
seguintes dados: a menor taxa de positividade entre os genótipos mais freqüentes no país (Tabela
1) e o número de infecções pelo HBV notificadas em 2004 pelo Sistema de Informação de
Agravos de Notificação do Programa Estadual de Controle das Hepatites da Secretaria de Saúde
de Alagoas – SINAN/PROVEP/SEAU/AL, que foi de 214. Com base nessas informações foi
definido um tamanho amostral mínimo de 119 a um nível de confiança de 95%.
Tabela 1. Taxa de positividade dos genótipos do HBV mais freqüentes no Brasil
Genótipos
Taxa de positividade (%) / Estado
Menor
Maior
A
9,8 - Paraná
88,6 – Pará
D
8,6 - Pará
85,9 – Paraná
F
1,6 - Paraná
29,2 – Pernambuco
(Bertolini et al., 2004; Mello et al., 2007)
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
35
4.3 População de estudo
Foram selecionados 119 pacientes com resultados positivos para os marcadores
sorológicos HBsAg e anti-HBc, procedentes da capital e do interior. Os pacientes foram
categorizados em três grupos: infecção aguda, pela presença de anti-HBc IgM; portador
assintomático, positividade para HBsAg por mais de seis meses e hepatite crônica confirmada
pelo diagnóstico histopatológico.
4.4 Coleta de dados e amostras
Após o preenchimento de um questionário com os dados demográficos (sexo, idade e
cor/raça), foram coletados 10mL de sangue, por meio de punção venosa e centrifugados para a
obtenção de três alíquotas de soro visando à dosagem de ALT, pesquisa dos marcadores
sorológicos e estudo molecular. A partir dos prontuários foram obtidas informações sobre
resultados anteriores dos marcadores sorológicos para hepatite B, exame histopatológico e
tratamento com interferon e/ou lamivudina.
4.5 Dosagem de alanina aminotransferase
A dosagem de ALT foi realizada por meio da metodologia NADH (NicotinamidaAdenina-Dinucleotídio na sua forma reduzida) de acordo com o protocolo do fabricante (Abbott
Laboratórios do Brasil). Foi considerado valor normal (N) quando a concentração foi menor que
1,5 vezes o limite normal superior (LNS, 55U/L) e elevado (E) quando maior ou igual a 1,5 vezes
LNS (Lai et al., 2003).
4.6 Marcadores sorológicos
Foram pesquisados os marcadores (HBsAg, anti-HBc, HBeAg e anti-HBe) pelo método
imunoenzimático utilizando kits comerciais (ELISA, Symbiosis Diagnóstica Ltda, São Paulo,
Brasil), de acordo com as instruções do fabricante.
4.7 Extração do DNA viral
O DNA viral foi extraído do soro utilizando-se uma solução de isotiocianato de guanidinafenol
(Brasol,
LGC
Biotecnologia).
O
procedimento
técnico
envolveu
as
ZAIDAN, A.M. E.
36
Caracterização genética do vírus da hepatite B...
seguintes etapas: em tudos de 1,5 mL foi adicionado 300 µL da solução de isotiocianato de
guanidina-fenol mais 200 µL de soro e em seguida agitação vigorosa por inversão, adição de 50
µL de clorofórmio gelado e centrifugação a 13000xg a 4ºC por 8 minutos.
Para a precipitação do DNA, o sobrenadante foi tratado com 300 µL de etanol absoluto
gelado e após agitação por um minuto, foi centrifugado a 13000xg a 4ºC por 15 minutos. O
precipitado obtido (DNA-HBV) foi retratado com etanol gelado, centrifugado a 13000xg a 4ºC
por 10 min e ressuspendido em 50 µL de água livre de RNASE e DNASE (água para PCR,
Ludwig Biotec).
4.8 Amplificação do gene S e regiões pré-core e core - PCR nested
A amplificação parcial do gene S (fragmento de 417pb) e regiões pré-core (fragmento de
307pb) e core (fragmento de 270pb) foi realizada segundo protocolo desenvolvido por Kaneko et
al. (1989). As seqüências dos oligonucleotídeos iniciadores (primers) (Operon Colônia,
Alemanha) utilizados estão apresentadas na tabela 2.
Tabela 2. Relação dos Primers utilizados nas amplificações do gene S e regiões pré-core e core.
Primer
Posição
Seqüência 5` → 3`
Referência
REGIÃO S
FHBS1
244
GAGTCTAGACTCGTGGTGGACTTC
Sitnik
RHBS1
668
AAATKGCACTAGTAAACT
2004
FHBS2
255
CGTGGTGGACTTCTCTCAATTTTC
RHBS2
648
GCCARGAGAAACGGRCTGAGGCCC
et
al.,
REGIÃO PRÉ-CORE
F EP1-1
1606
TCATGGAGACCACCG TGAAG
Takahashi et al.,
REP1-2
1955
GGAAAGAAGCAGAGGCAA
1995
FEP2-1
1653
CATAAGAGGCTCTGGACT
REP2-2
1940
GGCAAAAAAGAGAGTAACTC
REGIÃO CORE
F1763
1763
GCTTTGGGGCATGGACATTGACCCGTATAA
Kaneko et al.,
R2032
2032
CTGACTACTAATTCCCTGGATGCTGGGTCT
1989
F1778
1778
GACGAATTCCATTGACCCGTATAAAGAATT
R2017
2017
ATGGGATCCCTGGATGCTGGGTCTTCCAAA
F, forward; R, reverse
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
37
4.9 Amplificação parcial do gene S
Em cada tubo de PCR foi adicionado 10 µL de DNA HBV mais 90 µL de uma solução
pré-mix (10mM tampão taq polimerase, 50mM KCl, 1,5mM MgCl2, 150µM de cada dNTP, 20
pmol/µL de cada primer e 2,5U taq polimerase). A reação de amplificação foi realizada em um
termociclador PTC 100 programado nas seguintes condições: 94ºC, 20s, seguido por 30 ciclos de
94ºC, 20s; 56ºC, 20s; 72ºC, 30s e uma etapa final de extensão a 72ºC, 7 min. Para o primeiro ciclo
de amplificação foram empregados os primers FHBS1(F, forward) e RHBS1 (R, reverse) e para a
reamplificação foi utilizado 10 µL do produto de amplificação primária e os primers FHBS2 e
RHBS2.
4.10 Amplificação parcial da região pré-core
Para o primeiro ciclo de amplificação foram empregados os primers F-EP1.1 e R-EP1.2 e
para o segundo ciclo, F-EP2.1 e REP2.2. Na reação foram ulilizadas as mesmas concentrações da
PCR do gene S, porém, as condições de amplificação foram as seguintes: 94ºC, 30s, seguido por
30 ciclos de 94ºC, 30s; 56ºC, 30s; 72ºC, 40s e uma etapa final de extensão a 72ºC, 5min.
4.11 Carga viral - Titulação do DNA HBV
Para estimar a carga viral, amostras de soro, puros e diluídos, foram submetidas ao
protocolo de extração do DNA viral com NAOH 0,5M seguido diretamente de PCR da região
core (KANEKO; FEINSTONE; MILLER, 1989), utilizando os primers 1763F, e 2032R, para o
primeiro ciclo e 1778-F, e 2017R, para o segundo ciclo. Em tubos contendo 10 µL de amostras de
soro puros e diluídos (10-2, 10-4, 10-6, 10-8 e 10-10) com água milli Q autoclavada, foram
adicionados 2,5µl de NAOH 0,5M. Após uma hora a 37ºC foram acrescentados 2,5 µL de HCL
0,5M e 85 µL de pré-mix contendo10mM tampão taq polimerase, 50mM KCl, 1,5mM MgCl2,
150µM de cada um dos quatro dNTP, 20 pmol/µL de cada primer e 2,5U taq polimerase. A reação
de amplificação foi realizada sob as seguintes condições: 94ºC, 60s; seguido por 30 ciclos de
94ºC, 60s; 45ºC, 60s; 72ºC, 90s e ao final uma etapa de extensão a 72ºC, 7 min.
A carga viral (genomas/mL) foi calculada multiplicando-se o título da reação,
correspondendo a mais alta diluição do soro com PCR positiva pelo limite de detecção do método
(3 x 102 genomas/mL) como descrito por ANJOS et al. (2000).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
38
4.12 Eletroforese em gel de agarose dos fragmentos genômicos
Para a identificação dos fragmentos genômicos amplificados, foram realizadas corridas
eletroforéticas em gel de agarose a 2%, contendo como corante bromento de etídio a 1%. Foi
aplicada uma mistura constituída de 8 µL do produto da PCR mais 2µL do corante azul de
bromofenol. Como controle da eficiência da corrida eletroforética e referência para identificar o
tamanho
do
fragmento
amplificado,
um
padrão
de
peso
molecular
de
100
pb
(DNA ladder, invitrogen, Califórnia USA) foi aplicado junto com as amostras. O tempo de corrida
foi de 40 minutos, sob voltagem de 100 V. Os padrões eletroforéticos gerados foram fotografados
por meio de um sistema digital sob luz ultravioleta.
4.13 Reação de seqüenciamento
Os produtos de reamplificação do gene S e da região pré-core, foram submetidos a um
ciclo de PCR linear visando a incorporação dos dideoxinucleotídeos associados a uma
fluorescência, princípio do método de seqüenciamento direto (SANGER; COULSON, 1975).
Foram utilizados os primers específicos para cada tipo de seqüência investigada e reagentes
disponíveis comercialmente, DYEnamic EDTye Terminator Cicle Sequencing kit de acordo com
instruções do fabricante (GE Healthcare, Inglaterra), adaptado para o seqüenciador automático
MegaBace 500®.
4.14 Análise das seqüências
A análise dos genótipos foi realizada pela comparação entre o alinhamento das seqüências
de nucleotídeos obtidas com as 54 seqüências já conhecidas dos diferentes genótipos de HBV
depositadas no Genbank. As mutações foram identificadas pelo alinhamento das seqüências de
nucleotídeos obtidas no estudo e comparadas com uma seqüência do vírus selvagem. Para estas
análises foram utilizados os programas EditSeq e Megalign do pacote DNAstar (Lasergene Inc.,
Madison, WI, EUA). A classificação dos genótipos foi confirmada pela ferramenta Genotyping
disponível no site do NCBI (The National Center for Biotechnology Information)
(http://www.ncbi.nlm.nih.gov/projects/genotyping/formpage.cgi).
A identificação dos genótipos e mutações só foi possível nas seqüências cujo esferograma
apresentou índex de qualidade superior a 80%, obtido no algoritmo FHRED.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
39
4.15 Análise dos dados
A análise dos dados foi realizada de forma descritiva por meio de medidas de freqüências,
sendo calculada média e desvio padrão da variável quantitativa.
4.16 Limitação metodológica do estudo
O número de portadores assintomáticos da infecção pelo HBV poderia ter sido
subestimado, levando a um viés de seleção, uma vez que a procura pelo serviço de hepatologia
geralmente vem acompanhada de alguma queixa relacionada com doença hepática. Porém foi
minimizado pelo encaminhamento de pacientes procedentes de hemocentros, dos serviços de prénatal, unidades de hemodiálise e centros de triagem anônima (CTA), representando 61,3% da
população de estudo.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
40
5.0 ARTIGO I
Caracterização genotípica do vírus da hepatite B em Alagoas, Brasil
Alba M. X. Eloy1, Marcílio L. Figueiredo2, Arliete R. S. M. de Barros3, Jéfferson LA Silva4,
Regina C. Moreira2 , Maria Rosângela C. D. Coêlho4,5
1
Instituto de Ciências Biológicas e da Saúde-ICBS/UFAL
2
Setor de Hepatites Virais do Instituto Adolfo Lutz – São Paulo
3
Laboratório de Análises Clínicas do Hospital Universitário Prof. Alberto Antunes/UFAL
4
Setor de Virologia do Laboratório de Imunopatologia Keizo Asami (LIKA)-UFPE
5
Departamento de Fisiologia e Farmacologia da Universidade Federal de Pernambuco (UFPE)
1
Endereço: Rua Barão José Miguel nº 249/601 Farol, Maceió-AL
CEP 57055-160
Tel. 82 99684084
e-mail: [email protected]
RESUMO
O vírus da hepatite B está classificado em oito genótipos, A – H, com prevalências distintas em
diferentes áreas geográficas. As divergências inter-genotípicas são baseadas em uma diferença
superior a 8% na seqüência do genoma viral. O objetivo do estudo foi investigar os genótipos do
HBV circulantes em Alagoas e caracterizar a infecção quanto à carga viral, perfil HBeAg/antiHBe e nível sérico da alanina aminotransferase (ALT). Foi realizado um estudo transversal
descritivo envolvendo pacientes encaminhados pelos Centros de Referências em hepatites virais
do Estado de Alagoas, Nordeste/Brasil, durante o período de setembro 2006 a abril 2008. Foram
selecionados 119 pacientes com sorologia positiva para HBsAg e anti-HBc, entre os quais, 2,5 %
(3) tinham o diagnóstico de hepatite aguda, 69,7 % (83) de portador assintomático e 27,8 % (33)
de hepatite crônica. As amostras de sangue foram submetidas aos procedimentos de extração e
amplificação parcial do gene S visando à caracterização genotípica. O DNA HBV foi detectado
em 70,6% (84/119) dos pacientes. Foram identificados os seguintes genótipos: A em 92,5%, C em
5,0% e 1,25% para os genótipos D e F. A pesquisa demonstrou que o genótipo A foi
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
41
predominante em Alagoas, Brasil e a maioria das infecções apresentou carga viral reduzida,
concentração sérica normal da ALT e soro-conversão do HBeAg para o anti-HBe, caracterizando
a fase residual da infecção crônica pelo HBV.
Palavras chaves: vírus da hepatite B, genótipos, hepatite B crônica.
INTRODUÇÃO
O vírus da hepatite B (HBV) está classificado em oito genótipos, A-H, com prevalências
distintas em diferentes áreas geográficas. As divergências inter-genotípicas foram definidas
arbitrariamente com base em uma diferença superior a 8% na seqüência do genoma viral
(Okamoto et al. 1988; Noder et al. 1992).
O genótipo A é mais freqüente no Noroeste Europeu, África Central e Américas (Stuyver
et al. 2000; Chu; Hussain; Lok 2002). Os genótipos B e C no Sudeste Asiático, China e Japão
(Yotsuyanagi et al. 2002; Yuen et al. 2004; Chou et al. 2008). O genótipo D predomina no Sul
Europeu, Oriente Médio e Índia (Bozdayi et al. 2001; Olyaee et al. 2005; Chauhan et al. 2006),
enquanto o genótipo E é encontrado principalmente na parte ocidental da África (Candotti et al.
2006). O genótipo F é encontrado em populações aborígenes das Américas e na Polinésia (Norder
et al. 1996; Devesa et al. 2004). O genótipo G foi detectado na França, nos Estados Unidos
(Stuyver et al. 2000), no México (Sánchez et al. 2002) e no Brasil (Bottecchia et al. 2008), sendo
encontrado freqüentemente em co-infecção com o genótipo A (Kato et al. 2002). O genótipo H foi
descrito na Nicarágua, México e Estados Unidos (Arauz-Ruiz et al. 2002; Schaefer 2005).
No Brasil, a distribuição genotípica é heterogênea, refletindo a diversidade da população
brasileira. O genótipo A é predominante (Araújo et al. 2004; Sitnik et al. 2004; Motta-Castro et al.
2005; Oliveira et al. 2008) e o F é mais freqüente na população indígena da região amazônica
(Viana et al. 2005). Os genótipos B, C estão descritos, com maior freqüência, em populações de
etnia asiática (Sitnik et al. 2004), enquanto o D em indivíduos de origem italiana, encontrados
freqüentemente nas regiões Sudeste, Sul e Centro-Oeste do país (Teles et al. 2002; Carrilho et al.
2004; Paraná & Almeida 2005; Sitnik et al. 2004; Rezende et al. 2005). De um modo geral, pelo
menos dois dos genótipos A, D e F co-circulam em diferentes regiões brasileiras (Mello et al.
2007).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
42
Os genótipos podem influenciar as características virais e conseqüentemente o curso
clínico da infecção. Nas regiões onde os genótipos A e D são prevalentes, as infecções pelo A
apresentaram maior freqüência de ALT elevada (Kumar et al. 2005), embora a doença hepática
mais severa foi associada ao genótipo D (Thakur et al. 2002). Estudo envolvendo os genótipos A,
D e F, a soroconversão do HBeAg não mostrou relação com os referidos genótipos. No entanto,
após a soroconversão, as infecções pelo genótipo A apresentaram taxa de eliminação do DNA
HBV mais alta e com o genótipo F a mortalidade relacionada com doença hepática foi mais
freqüente (Sanchez-Tapias et al. 2002).
Devido à ausência de estudos moleculares envolvendo o HBV em Alagoas, o presente
estudo investigou os genótipos do referido vírus e caracterizou as infecções quanto a carga viral,
perfil HBeAg/anti-HBe e nível sérico de ALT.
MATERIAL E MÉTODOS
Desenho do estudo e seleção dos pacientes
Foi realizado um estudo transversal descritivo envolvendo pacientes atendidos nos centros
de referências em hepatites virais do Estado de Alagoas durante o período de setembro de 2006 a
abril de 2008. Essa pesquisa foi aprovada pelo Comitê de Ética em pesquisa da Universidade
Federal de Alagoas (UFAL).
Foram selecionados 119 pacientes com resultados positivos para os marcadores
sorológicos HBsAg e anti-HBc, procedentes da capital e do interior. Os pacientes foram
categorizados em três grupos: infecção aguda, pela presença de anti-HBc IgM; portador
assintomático, pela positividade para HBsAg por mais de seis meses e hepatite crônica
confirmada pelo diagnóstico histopatológico.
Coleta de dados e amostras
Após o preenchimento de um questionário com os dados demográficos (sexo, idade e
cor/raça), 10 mL de sangue foram coletados e centrifugados para a obtenção de três alíquotas de
soro visando a dosagem de ALT, pesquisa dos marcadores sorológicos e estudo molecular. A
partir dos prontuários foram obtidas informações referentes ao diagnóstico histopatológico e
resultados anteriores dos marcadores sorológicos, HBsAg e anti-HBc.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
43
Dosagem de alanina aminotransferase
Foi realizada por meio da metodologia NADH (Nicotinamida-Adenina-Dinucleotídio na
sua forma reduzida) de acordo com o protocolo do fabricante (Abbott Laboratórios do Brasil). Foi
considerado valor normal (N) quando a concentração foi menor que 1,5 vezes o limite normal
superior (LNS, 55U/L) e elevado (E) quando maior ou igual a 1,5 vezes LNS (Lai et al. 2003).
Marcadores sorológicos
Foram pesquisados os marcadores (HBsAg, anti-HBc, HBeAg e anti-HBe) pelo ensaio
imunoenzimático (ELISA) utilizando kits comerciais (Symbiosis Diagnóstica Ltda, São Paulo,
Brasil).
Extração e amplificação parcial do gene S – fragmento de 417 pb
A extração do DNA HBV e amplificação parcial do gene HBsAg foram realizadas
segundo protocolo descrito por Kaneko et al. (1989), empregando-se os oligonucleotídeos
iniciadores (primers) (Operon, Colônia, Alemanha) selecionados por Sitnik et al. 2004), FHBS1,
posição 244-267 (5’GAGTCTAGACTCGTGGTGGACTTC–3’), RHBS1, posição 668-691
(5’AAATKGCACTAGTAAACT3’) para o primeiro ciclo (PCR I). Para a reamplificação (nestedPCR), FHBS2, posição 255-278 (5’CGTGGTGGACTTCTCTCAATTTTC3’), RHBS2, posição
648-671 (5’GCCARGAGAAACGGRCTGAGGCCC3’).
O DNA HBV foi extraído por meio do tratamento do soro com isotiocianato de guanidinafenol (LGC Biotecnologia), precipitado com etanol absoluto gelado e ressuspendido em água livre
de RNASE e DNASE (Ludwig Biotec). Em cada tubo de PCR foi adicionado 10 µL de DNA
HBV mais 90 µL de uma solução pré-mix (10mM tampão Taq DNA polimerase, 50mM KCl,
1,5mM MgCl2, 150µM de cada dos quatro dNTP, 20 pmol/µL de cada primer e 2,5U taq
polimerase). A reação de amplificação foi realizada nas seguintes condições: 94ºC, 30s, seguido
por 30 ciclos de 94ºC, 20s; 56ºC, 20s; 72ºC, 30s e uma etapa final de extensão a 72ºC, 7 min.
Carga viral - Titulação do DNA HBV
Para estimar a carga viral, amostras de soro, puros e diluídos, foram submetidas ao
protocolo de extração do DNA viral com NAOH 0,5M seguido diretamente de PCR da região
core
como
descrito
por
Kaneko
et
al.
(1989),
utilizando
os
primers
1763F(
2032R
5`GCTTTGGGGCATGGACATTGACCCGTATAA3`),
(5`CTGACTACTAATTCCCTGGATGCTGGGTCT3`), para o primeiro ciclo e 1778-F
(5`GACGAATTCCATTGACCCGTATAAAGAATT
3`)
e
2017R(
5`ATGGGATCCCTGGATGCTGGGTCTTCCAAA3`), para o segundo ciclo. Em tubos contendo
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
44
10 µL de amostras de soro puros e diluídos a 10-2, 10-4, 10-6, 10-8 e 10-10, com água milli Q
autoclavada, foram adicionados 2,5µl de NAOH 0,5M. Após uma hora a 37ºC foram
acrescentados 2,5 µL de HCL 0,5M e 85 µL de pré-mix (10mM tampão taq polimerase, 50mM
KCl, 1,5mM MgCl2, 150µM de cada um dos quatro dNTP, 20 pmol/µL de cada primer e 2,5U taq
polimerase). A reação de amplificação foi realizada sob as seguintes condições: 94ºC, 60s;
seguido por 30 ciclos de 94ºC, 60s; 45ºC, 60s; 72ºC, 90s e ao final uma etapa de extensão a 72ºC,
7 min.
A carga viral (genomas/mL) foi calculada multiplicando-se o título da reação,
correspondendo a mais alta diluição do soro com PCR positiva pelo limite de detecção do método
(3 x 102 genomas/mL) como descrito por Anjos (1999).
Identificação dos fragmentos genômicos
Os fragmentos genômicos amplificados foram visualizados por meio de corridas
eletroforéticas em gel de agarose a 2% contendo brometo de etídio a 1%, como corante. Os
padrões eletroforéticos gerados foram fotografados por meio de um sistema digital sob luz
ultravioleta.
Reação de seqüenciamento
Os produtos de reamplificação do gene S de ambas as fitas foram submetidos a um ciclo
de PCR linear utilizando os primers do segundo ciclo (FHBS2, RHBS2). Para a reação de
seqüenciamento direto (Sanger & Coulson 1975) foram empregados reagentes DYEnamic EDTye
Terminator Cicle Sequencing kit, de acordo com as instruções do fabricante (GE Healthcare,
Buckinghamshire, Inglaterra), adaptado para o seqüenciador automático MegaBace 500® .
Análise das seqüências
A classificação dos genótipos foi realizada pela comparação dos alinhamentos entre as
seqüências de nucleotídeos obtidas com as 54 seqüências já conhecidas dos diferentes genótipos
do HBV depositadas no Genbank. Para estas análises foram utilizados os programas EditSeq e
Megalign do pacote DNAstar (Lasergene Inc., Madison, WI, EUA). A classificação dos genótipos
foi
confirmada
pela
ferramenta
Genotyping
disponível
(http://www.ncbi.nlm.nih.gov/projects/genotyping/formpage.cgi).
no
site
do
NCBI
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
45
Análise dos dados
A análise dos dados foi realizada de forma descritiva por meio de medidas de freqüências,
sendo calculada média e desvio padrão da variável quantitativa.
RESULTADOS
Entre os 119 pacientes que constituíram a população de estudo, a média de idade e o
desvio padrão (DP) foi de 35±10,9. O gênero masculino contribuiu com 62,2% (74) e os pacientes
de etnia asiática com 2,5% (3).
Quanto à condição clínica, 2,5 % (3) tinham hepatite aguda, 69,7 % (83) eram portadores
assintomáticos e 27,8 % (33) apresentavam hepatite crônica.
O fragmento da região S do DNA-HBV foi detectado em 70,6% (84/119) e os genótipos
identificados em 95,2% (80/84) das seqüências. Os genótipos encontrados foram: A em 92,5%
(74), C em 5,0% (4) e 1,25% (1) para os tipos D e F. A etnia asiática foi identificada em um
paciente com infecção pelo genótipo A e em dois pelo C.
Em relação às características clínicas, as infecções pelo genótipo C foram detectadas em
três portadores assintomáticos e em um paciente com hepatite crônica, os quais apresentaram
soro-conversão do HBeAg e carga viral ≥ 3,104 cópias/mL. Um portador assintomático apresentou
ALT elevada. Os dois casos de infecção pelo HBV genótipos D e F foram identificados em
portadores assintomáticos, com ALT normais, HBeAg negativos e anti-HBe positivos e cargas
virais de 3 x 1010 e 3 x 102 cópias/mL, respectivamente.
A tabela 1 apresenta as características clínicas e laboratoriais das infecções pelo genótipo
A do HBV.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
46
Tabela 1. Dados laboratoriais das infecções pelo HBV genótipo A segundo a condição clínica.
Alagoas, Nordeste/ Brasil. Setembro 2006 a Abril 2008.
Dados laboratoriais
Portadores
Hepatite
Hepatite aguda
Assintomáticos (n=48)
crônica
(n=2)
(n=24)
Carga viral (cópias/mL)
≤ 3x102
39 (81,3%)
13(54,2%)
3x104
6(12,5%)
3(12,5%)
≥3x106
3(6,3%)
8(33,3%)
Normal
45(93,7%)
18(75,0%)
Elevada
3 (6,3%)
6(25,0%)
Negativo/positivo
45(93,7%)
18(75,0%)
Positivo/negativo
1(2,1%)
4(16,7%)
Negativo/negativo
2(4,2%)
2(8,3%)
Dosagem
de
2 (100%)
alanina
aminotransferase (U/L)
Marcadores
2(100%)
sorológicos
(HBeAg/anti-HBe)
1(50,0%)
1(50,0%)
DISCUSSÃO
No Brasil, as infecções pelos genótipos A, D e F são as mais freqüentes, embora com um
padrão de distribuição diferente em função da composição da população de estudo (Mello et al.
2007).
A maior freqüência de infecções pelo genótipo A encontrada na pesquisa foi também
demonstrada em Salvador (Lyra et al. 2005; Ribeiro et al. 2006), Pernambuco (Mello et al. 2007)
e região amazônica (Viana et al. 2005; Oliveira et al. 2008). Nos estudos brasileiros o genótipo A
é sempre encontrado e dependendo da composição da população estudada ora predomina com o
genótipo D (Teles et al. 2002; Carrilo et al. 2004; Rezende et al. 2005) ora com o tipo F (Ribeiro
et al. 2006; Mello et al. 2007). Entretanto, em Alagoas o A foi seguido do genótipo C.
Ressaltando que a infecção pelo genótipo A foi também encontrada em um paciente asiático,
concordando com o relato de Sitnik et al (2004).
Em relação ao genótipo C, no Brasil as infecções por esse genótipo foram relatadas por
Bottecchia et al. (2007) e Oliveira et al. (2008) em baixa freqüência e por outro lado, por Sitnik et
al. (2004) em alta freqüência, porém, em pacientes asiáticos. Considerando que o mesmo
predomina na Ásia e que a população de asiáticos residentes em Alagoas é de apenas 0,1%
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
47
segundo o Instituto Brasileiro de Geografia e Estatística (IBGE, 2000), sua identificação foi um
resultado não esperado.
A identificação do genótipo D em Alagoas foi também um resultado não esperado, uma
vez que em Salvador-BA Ribeiro et al. (2006) não identificaram nenhuma infecção por esse
genótipo em 76 pacientes investigados. Todavia, com relação à freqüência identificada, demonstra
uma concordância com o padrão de distribuição no país. Predomínio no Sul e Sudeste, regiões
onde ocorreram imigrações italianas (Rezende et al. 2005; Carrilho et al. 2004; Mello et al. 2007)
e freqüências menores no Nordeste (Lyra et al.2005; Mello et al. 2007).
O genótipo F não seguiu o padrão de distribuição nacional, onde as infecções por esse tipo
são mais freqüentes nas regiões Norte e Nordeste (Viana et al.2005; Ribeiro et al.2006; Mello et
al. 2007). Contudo, concordaram com os achados de Rezende et al. (2005) em São Paulo e Mello
et al.( 2007) em Santa Catarina que o encontraram em baixa freqüência.
A maioria das infecções pelo genótipo A apresentou a condição clínica de portador
assintomático, com baixa concentração de DNA HBV (≤ 300 cópias/mL) e soroconversão do
HBeAg, resultados que concordaram com a descrição clássica de Hoofnalge et al (1987). Em
comunidades afrodescendentes do Mato Grosso do Sul, Motta-Castro et al. (2005) encontraram
resultados semelhantes. Este perfil segundo Lai et al (2003) é comumente observado em regiões
de baixa e média endemicidade, onde a infecção é adquirida durante a adolescência ou início da
vida adulta, caracterizando a fase residual ou não replicativa da infecção pelo HBV.
O estudo marcou o primeiro registro da circulação dos genótipos A, C, D e F em Alagoas,
Nordeste brasileiro. O genótipo A foi predominante e a maioria das infecções foi identificada em
portadores assintomáticos.
REFERÊNCIAS
Anjos LC. Marcadores de replicação do vírus da hepatite B: comparação de métodos de biologia
molecular, de sorologia e imunohistoquímuca. São Paulo, 1999. (Dissertação de Mestrado –
Facultade de Medicina da Universidade de São Paulo).
Araujo NM, Mello FCA, Yoshida CFT, Niel C, Gomes SA 2004. High proportion of subgroup A’
(genotype A) among Brazilian isolates of hepatitis B virus. Archives of Virology 49:1383-1395.
Arauz-Ruiz P, Norder H, Robertson BH, Magnius LO 2002. Genotype H: a new ameridian genotype
of hepatitis B virus revealed in Central America. Journal of General Virology 83:2059-2073.
Bottecchia M, Souto FJD, Ó KMR, Amendola M, Brandão CE, Niel C, Gomes SA 2008. Hepatitis B
virus genotypes and resistance mutations in patients under long term lamivudine therapy:
characterization of genotype G in Brazil. BMC Microbiology 8: (11)1471-1480.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
48
Bozdayi AM, Bozkaya H, TürkylLmaz AR, Saýodlu M, Cetinkaya H, Karayalçin S, Yurdaydin C,
Uzunalimoğlu Ö 2001. Nucleotide divergences in the core promoter and precore region of genotype D
hepatitis virus in patients with persistently elevated or normal ALT levels. Journal of Clinical Viroloy
21: 91-101.
Candotti D, Opare-sem O, Rezvan H, Sarkodie F, Allain JP 2006. Molecular and serological
characterization of hepatitis B virus in deferred Ghanaian blood donors with and without elevated
alanine aminotransferase. Journal of viral hepatology 13: 715-24.
Carrilho FJ, Moraes CR, Pinho JRR, Mello IMVGC, Bertolini DA, Lemos MF, Moreira RC,
Bassit LC, Cardoso RA, Santos GR, Silva LC 2004. Hepatitis B vírus infection in haemodilysis
centres from Santa Catarina state, Southern Brazil. Predictive risk factors for infection and
molecular epidemiology. BMC Public Health 4:13.
Chauhan R, Kazim SNBhattacharjee J, Sakhuja P, Sarin SK 2006. Basal core promoter, precore
region mutations of HBV and their association with e antigen, genotype, and severity of liver
disease in patients with chronic hepatitis B in India. Journal of Medical Virology 78: 1047-54.
Chou YC,Yu MW,Wu CF,Yang, SY,Lin CL,Liu CJ, Shih WL, Chen PL, Liaw YF, Chen CJ
2008. Temporal relationship between hepatitis B vírus enhancer II/basal core promoter sequence
variation and risk of hepatocellular carcinoma. Gut 57:91–97.
Chu CJ, Hussain M, Lok ASF 2002. Hepatitis B virus genotype B is associated with earlier
HBeAg seroconversion compared with hepatitis B virus genotype C. Gastroenterology 122: 17561762.
Devesa M, Rodriguez C, Lei NG, Liprandi F, Pujol FH 2004. Clade analysis and surface antigen
polymorphism of hepatitis B vírus American genotypes. Journal of Medical Virology 72: 377-84.
Genotyping. Disponível em: <www.ncbi.nlm.nih.gov/projects/genotyping/formpage.cgi>. Acesso:
31jul2008.
Instituto
Brasileiro
de
Geografia
e
Estatística.
Disponível
<http://www.sidra.ibge.gov.br/bda/tabela/listabl.asp?z=t&c=136>. Acesso: 27fev2009.
em:
Kaneko S. Feinstone SM. Miller RH 1989. Rapid and sensitive method for the detection of serum
hepatitis B virus DNA using the polymerase chain reaction technique. Journal of Clinical
Microbiology 27:1930-1933.
Kato H, Orito E, Gisg RG, Bzowej N, Newsom M, Sugauchi F, Susuki S, Ueda R, Miyakawa Y,
Mizokami M 2002. Hepatitis B e antigen in sera from individuals infected with hepatitis B virus of
genotype G. Hepatology 35:(4) 922-929.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
49
Kumar A, Kumar SI, Pandey R, Naik S, Aggarwal R 2005. Hepatitis B virus genotype A is more
often associated with severe liver disease in northern India than is genotype D. Indian J
Gastroenterol 24:19-22.
Lai CL, Ratziu V, Yuen M-F, Polynard T 2003. Viral hepatitis B. The Lancet 362: 2089-2094.
Lyra AC, Pinho JRR, Mello IMVGC, Malta FM, Gomes MMS, Bisceglie AMD, Lyra LGC 2005.
Distribution of hepatitis B virus genotypes among patients with acute viral hepatitis. J Clin
Gastroenterol 39: 81.
Mello FCA, Souto FJD, Nabuco LC, Nogueira CAV, Coelho HSM, Franz LCF, Saraiva JCP,
Virgolino HA, Motta-Castro AR 2007. Hepatitis B vírus circulating in Brazil: Molecular
characterization of genotype F isolates. BMC Microbiology 7:103.
Motta-Castro ARC, Martins RMB, Yoshida CFT, Teles AS, Paniago AM, Lima KMB, Gomes AS
2005. Hepatitis B virus infection in isolated Afro-Brasilian communites. Journal of Medical
Virology 77: 188-193.
Norder H, Hammas B, Löfdahl S, Couroucé A-M, Magnius 1992. Comparison of the amino acid
sequences of nine different serotypes of hepatitis B surface antigen and genomic classification of the
corresponding hepatitis B virus strains. Journal of general Virology 73: 1201-1208.
Norder H, Ebert JW, Fields HA, Mushahwar IK, Magnius LO 1996. The complete nucleotide
sequence of a pre-core mutant of hepatitis B virus implicated in fulminant hepatitis and its biological
characterization in chimpanzes. Virology 218: 214-223.
Olyaee ABS, Forooshani SR, Adeli A, Sabahi F, Abachi M, Azizi M, Mahboudi F 2005.
Complete genomic sequence and phylogenetic relatedness of hepatitis B vírus isolates from Iran.
Journal of Medical Virology 76: 318-26.
Oliveira CM, Farias IP, Fonseca JC, Brasil LM, Souza R, Astolfi-Filho S. 2008. Phylogeny and
molecular genetic parameters of different stages of hepatitis B virus infection in patients from the
Brazilian Amazon. Arch Virol May 153: 823-30.
Paraná R, Almeida D 2005. HBV epidemiology in Latin América. Journal of Clinical Virology,
34:130-133.
Rezende REF, Fonseca BAL, Ramalho LNZ, Zucoloto S, Pinho JRR, Bertolini DA, Martinelli
ALC 2005. The precore mutation is associated with severity of liver damage in Brazilian patients
with chronic hepatitis B. Journal of Clinical Virology 32: 53-9.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
50
Ribeiro NRC, Campos GS, Ângelo ALD, Braga EL, Santana N, Gomes MMS, Pinho JRR, De
Carvalho WA, Lyra LGC, Lyra AC 2006. Distribution of hepatitis B vírus genotypes among
patients with chronic infection. Liver International 26: 636-642.
Sanchez-Tapias JM, Costa J, Mas A, Bruguera M, Rodes M 2002. Influence of hepatitis B virus
genotype on the long-term outcome of chronic hepatitis B in Western patients. Gastroenterology
123: 1848-56.
Sanger F, Coulson AR 1975. A rapid method for determining sequences in DNA by primed synthesis
with DNA polymerase. Journal of Molecular Biology 94: 441-448.
Schaefer S 2005. Hepatitis B vírus: significance of genotypes. Journal of viral hepatitis 12: 111124.
Sitnitk R, Pinho JRR, Bertolini DA, Bernadini AP, da Silva LC, Carrilho FJ 2004. Hepatitis B
virus genotypes and precore and core mutants in brasilian patients. Journal of Clinical
Microbiology 42: 2455-2460.
Stuyver L. De Gendt S, Geyt C, Zoulim F, Fried M, Schinazi RF, Rossau R 2000. A new genotype of
hepatitis B virus: complete genome and phylogenetic relatedness. Journal of General virology 81: 6774.
Thakur V, Guptan RC, Kazim SN, Malhotra V, Sarin SK. Profile, spectrum and significance of
HBV genotypes in chronic liver disease patients in the Indian subcontinent. Journal of
Gastroenterology and Hepatology, v. 17, n. 2, p. 113-115, Feb. 2002.
Teles AS, Martins RMB, Gomes AS, Gaspar AMC, Araújo NM, Souza KP, Carneiro MAS, Yoshida
CFT 2002. Hepatitis B virus transmission in Brazilian hemodialysis units: Serological and molecular
follow-up. Journal of Medical Virology 68: 41-49.
Viana S, Paraná R, Moreira RC, Compri AP, Macedo V 2005. High prevalence of hepatitis B vírus
and hepatitis D vírus in the western brasilian amazon. Am J Trop Med Hyg 73: 808-814.
Yotsuyanagi H, Hino K, Tomita E, Toyoda J, Yasuda K, Iino S 2002. Precore and core promoter
mutations, hepatitis B virus DNA levels and progressive liver injury in chronic hepatitis B. Journal of
Hepatology 37: 355-363.
Yuen MF, Lai CL 2001. Treatment of chronic hepatitis B. Lancet Infect Dis 1: 232-241.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
51
6.0 VERSÃO EM INGLÊS DO ARTIGO I
Genotypic characterization of the hepatitis B virus in Alagoas, Brazil
Alba MX Eloy1,3, Marcílio L Figueiredo2, Arliete RSM. de Barros3, Jéfferson LA Silva4
Regina C. Moreira2, Maria Rosângela CD Coêlho4, 5
1
Institute of Biological and Health Sciences (ICBS), Federal University of Alagoas
2
Viral Hepatitis Sector, Adolfo Lutz Institute, São Paulo
3
Clinical Analysis Laboratory, Prof. Alberto Antunes University Hospital, Federal University of
Alagoas
4
Virology Sector, Keizo-Asami Immunopathology Laboratory (LIKA), Federal University of
Pernambuco
5
1
Department of Physiology and Pharmacology, Federal University of Pernambuco
Address: Alba Maria Xavier Eloy
Rua Barão José Miguel nº 249/601,
Farol, Maceió-AL, CEP 57055-160
Tel. 82 99684084
e-mail: [email protected]
ABSTRACT
The hepatitis B virus is classified into eight genotypes (A to H), with different prevalences in
different geographical areas. The aim of this study was to investigate the genotypes of HBV that
are in circulation in Alagoas and to characterize the infection regarding viral load, HBeAg/antiHBe profile and serum level of alanine aminotransferase (ALT). This was a cross-sectional
descriptive study involving patients sent to viral hepatitis referral centers in the State of Alagoas,
Brazil, between September 2006 and April 2008. One hundred and nineteen patients serologically
positive for HBsAg and anti-HBc were selected. Among these, 2.5% (3) were diagnosed as
presenting acute hepatitis, 69.7% (83) as asymptomatic and 27.8% (33) as cases of chronic
hepatitis. Blood samples were subjected to procedures for extracting and amplifying a fragment of
the S gene, for genotyping. HBV DNA was detected in 70.6% of the patients. The following
genotypes were identified: A in 92.5%, C in 5.0% and D and F in 1.3% each. The study
demonstrated that genotype A was predominant in Alagoas, Brazil, and that most infections
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
52
presented a low viral load, normal serum concentration of ALT and seroconversion of HBeAg,
thus characterizing the residual phase of chronic HBV infection.
Key words: hepatitis B virus, genotypes, chronic hepatitis B
INTRODUCTION
Hepatitis B virus (HBV) has been classified into eight genotypes (A to H), with distinct
geographical distributions. The divergences between the genotypes have been defined arbitrarily,
based on a difference of more than 8% in the virus genome sequence (Okamoto et al. 1988; Noder
et al. 1992).
Genotype A is most frequent in northwestern Europe, central Africa and the Americas
(Stuyver et al. 2000; Chu; Hussain; Lok 2002). Types B and C are found mainly in southeastern
Asia, China and Japan (Yotsuyanagi et al. 2002; Yuen et al. 2004; Chou et al. 2008). Type D
predominates in southern Europe, Middle East and India (Bozdayi et al. 2001; Olyaee et al. 2005;
Chauhan et al. 2006). Type E is found mainly in western Africa (Candotti et al. 2006). Type F is
found in aboriginal populations of the Americas and Polynesia (Norder et al. 1994; Devesa et al.
2004). Type G has been detected in France and the United States (Stuyver et al. 2000), Mexico
(Sánchez et al. 2002) and Brazil (Bottecchia et al. 2008), and is frequently found as a coinfection
with type A (Kato et al. 2002). Type H has been described in Nicaragua, Mexico and the United
States (Arauz-Ruiz et al. 2002; Shaefer 2005).
In Brazil, the genotype distribution is heterogeneous, reflecting the diversity of the
Brazilian population. Type A is predominant (Araújo et al. 2004; Sitnik et al. 2004; Motta-Castro
et al. 2005; Oliveira et al. 2008), while type F is most frequent among the indigenous population
of the Amazon region (Viana et al. 2005). Types B and C have been described in Brazil most
frequently among populations of Asian ethnicity (Sitnik et al. 2004), while type D has been
described among individuals of Italian descent, most frequently in the southeastern, southern and
central-western regions of the country (Teles et al. 2002; Carrilho et al. 2004; Paraná & Almeida,
2005; Sitnik et al. 2004; Rezende et al. 2005). Generally, at least two out of the genotypes A, D
and F co-circulate in different regions of Brazil (Mello et al. 2007).
The genotypes may influence the characteristics of the virus and consequently of the infection. In
regions where the genotypes A and D are prevalent, the infections by A had the highest frequency
of elevated ALT (Kumar et al. 2005), although the more severe liver disease was associated with
genotype D (Thakur et al. 2002).
Study with the genotypes A, D and F, the seroconversion of HBeAg showed no relation with these
genotypes. However, after seroconversion, infection by genotype A showed higher rate of
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
53
elimination of HBV DNA and with F the mortality related to liver disease was more frequent
(Sanchez-Tapias et al., 2002) .
Because of the lack of studies on HBV genotyping Alagoas, the present study investigated
HBV genotypes and characterized infections in terms of viral load, HBeAg/anti-HBe profile and
serum ALT level.
MATERIAL AND METHODS
Study design and patient selection
A descriptive cross-sectional study on patients attended at viral hepatitis referral centers in
the State of Alagoas between September 2006 and April 2008 was conducted. This study was
approved by the Research Ethics Committee of the Federal University of Alagoas (UFAL).
One hundred and nineteen patients from both the state capital and elsewhere in the state were
selected. All of them had been found to be positive for the serological markers HBsAg and antiHBc. They were categorized in three groups: acute infection, when anti-HBc IgM was present;
asymptomatic, when positive for HBsAg for more than six months; and chronic hepatitis, when
confirmed by histopathological diagnosis.
Data and sample collection
A questionnaire seeking demographic data was applied (sex, age and color/race) and then
blood samples were obtained by means of venous puncture (without anticoagulant). These
samples were centrifuged to obtain three aliquots of serum, with the aims of assaying for alanine
aminotransferase (ALT), investigating serological markers and conducting a molecular analysis.
Information on the patients’ previous results regarding serological markers for HBV and
histological examinations was obtained from their medical files.
Alanine aminotransferase assay
Was performed using the methodology NADH (nicotinamide adenine dinucleotide in its reduced
form Dinucleotídio) in accordance with the manufacturer’s instructions (Abbott Laboratories,
Brazil). The assay result was considered normal (N) when the concentration was less than 1.5
times the normal upper limit (55 U/l) and high (H) when the concentration was greater than or
equal to 1.5 times the normal upper limit (Lai et al. 2003).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
54
Serological markers
The serological markers (HBsAg, anti-HBc, HBeAg and anti-HBe) were investigated by means of
the immunoenzymatic assay (ELISA), using commercial kits (Symbiosis Diagnóstica Ltda, São
Paulo, Brazil).
Extraction and S gene partial amplification - DNA fragment of 417 bp
The extraction of the viral genome and S gene partial amplification were performed in
accordance with the protocol of Kaneko et al. (1989), using external primers (Operon, Cologne,
Germany)
FHBS1,
(5’GAGTCTAGACTCGTGGTGGACTTC–3’,
RHBS1(5’AAATKGCACTAGTAAACT3’,
nt
(5’CGTGGTGGACTTCTCTCAATTTTC3’,
668-691)
nt
and
nt
internal
255-278)
244-267)
primers
and
and
FHBS2
RHBS2
(5’GCCARGAGAAACGGRCTGAGGCCC3’, nt 648-671), selected by Sitnik et al. (2004). HBV
DNA was extracted from serum using guanidine isothiocyanate-phenol (Brasol, LGC
Biotecnologia) and chloroform and precipitated with cold absolute ethanol. A 10 µL sample of
viral DNA extracted was amplified in a 100 µL reaction volume containing 10mM Taq DNA
polymerase buffer, 50mM KCl, 1.5mM MgCl2, 150µM each of the four dNTP, 20 pmol/µL of
each of the primer and 2.5 U Taq DNA polymerase. The reaction for the two rounds of the nested
PCR was performed under the following conditions: initial denaturation at 94°C, 20s followed by
30 cycles at 94°C, 20s; 56°C, 20s; 72 ºC, 30s and a final extension step at 72 ° C , 7 min.
Viral load - Titration of the HBV DNA
To estimate the viral load, serum samples pure and diluted, were incubated at 37oC for 1 h in the
presence of 2,5 µL NaOH 0.5 M followed directly of core region amplification by nested PCR as
described by Kaneko et al. (1989). Was added 2.5 µL of HCl 0.5 M and 85 µL of pre-mix
containing 10mM Taq DNA polymerase buffer, 50mM KCl, 1.5mM MgCl2, 150µM each of the
four dNTP, 20 pmol/µL of each of the primer and 2.5 U Taq DNA polymerase. Primers used were
as follows: external 1763F(5`GCTTTGGGGCATGGACATTGACCCGTATAA3`) and 2032R(5
`CTGACTACTAATTCCCTGGATGCTGGGTCT3`)
GACGAATTCCATTGACCCGTATAAAGAATT
and
internal
and
1778-F,
5
`3`
2017R(
5`ATGGGATCCCTGGATGCTGGGTCTTCCAAA3`). The amplification conditions for the two
rounds were as follows: 94 º C, 60s and 30 cycles at 94 ° C, 60s; 45oC, 60s; 72 º C, 90s with a
final elongation at 72 ° C, 7 min.
Viral load (copies / mL) was calculated by multiplying the title of the reaction with the
highest dilution of serum positive by PCR with detection limit of the method which corresponds
to 3 x 102 copies/mL as described by Anjos (1999).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
55
Identification of genomic fragments
The amplified genomic fragments were fractionated by 2% agarose gel electrophoresis
stained with ethidium bromide and visualized under UV light.
Sequencing reaction
The amplification products from the HBsAg gene were subjected to a linear PCR cycle using the
second round primers. For the direct sequencing reaction (Sanger & Coulson 1975), commercially
available reagents were used (DYEnamic EDTye Terminator Cycle Sequencing kit,
Buckinghamshire, England), adapted for the MegaBace 500 (GE Healthcare) automated
sequencer.
Analysis of the sequences
The genotypes were classified by comparing the alignments between the nucleotide
sequences with the 54 sequences of different HBV genotypes that are already known and
deposited in GenBank. For these analyses, the EditSeq and Megalign programs in the DNAstar
software package were used (Lasergene Inc., Madison, WI, USA). The genotype classification
was
confirmed
using
the
genotyping
tool
on
the
NCBI
website
(http://www.ncbi.nlm.nih.gov/projects/genotyping/formpage.cgi).
Data analysis
The data analysis was performed descriptively by means of frequency measurements.
Means and standard deviations were calculated for the quantitative variables.
RESULTS
Among the 119 patients who formed the study population, the mean age was 35 years and
the standard deviation (SD) was ± 10.9. Male gender accounted for 62.2% (74) and patients of
Asian ethnicity with 2.5% (3).
With regard to clinical condition, 2.5 % (3) had acute hepatitis, 69.7 % (83) were asymptomatic
and 27.8 % (33) presented chronic hepatitis.
The S gene fragment of HBV DNA was detected in 70.6% (84/119) and the genotype was
identified in 95.2% (80/84) of the sequences. The types found were: A in 92.5% (74), C in 5.0%
(4) and D and F in 1.3% (1) each. Asian ethnicity was identified in one patient with infection due
to genotype A and two of C.
With regard to clinical characteristics, infections due to genotype C were detected in three
asymptomatic individuals and in one with chronic hepatitis. These four presented seroconversion
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
56
of HBeAg and a viral load ≥ 3.104 copies/ml. One asymptomatic individual presented high ALT.
The two cases with HBV infection due to genotypes D and F were identified in asymptomatic
individuals with normal ALT, who were HBeAg-negative and anti-HBe-positive and had viral
loads of 3 x 1010 and 3 x 102 copies/ml respectively.
Table 1 presents the clinical and laboratory characteristics of the HBV infections due to genotype
A.
Table 1. Laboratory data on HBV infections due to genotype A, according to clinical condition.
Alagoas, northeastern Brazil. September 2006 to April 2008.
Laboratory data
Asymptomatic
Chronic
Acute hepatitis
individuals (n = 48)
hepatitis
(n = 2)
(n = 24)
Viral load (copies/ml)
≤ 3 x 102
39 (81.3%)
13 (54.2%)
3 x 104
6 (12.5%)
3 (12.5%)
≥ 3 x 106
3 (6.3%)
8 (33.3%)
45 (93.7%)
18 (75.0%)
3 (6.3%)
6 (25.0%)
Negative/positive
45 (93.7%)
18 (75.0%)
Positive/negative
1 (2.1%)
4 (16.7%)
Negative/negative
2 (4.2%)
2 (8.3%)
2 (100%)
Alanine aminotransferase
assay (U/l)
Normal
High
2 (100%)
Serological markers
(HBeAg/anti-HBe)
1 (50.0%)
1 (50.0%)
DISCUSSION
In Brazil, HBV infections due to genotypes A, D and F are the most frequent types,
although the distribution pattern varies according to the composition of the study population
(Mello et al. 2007). The greater frequency of infection due to genotype A that was found in the
present study has also been demonstrated in Salvador (Lyra et al. 2005; Ribeiro et al. 2006),
Pernambuco (Mello et al. 2007) and the Amazon region (Viana et al. 2005; Oliveira et al. 2008).
Genotype A is always found in Brazilian studies and, depending on the composition of the study
population, it is sometimes predominantly found with genotype D (Telles et al. 2002; Carrilo et al.
2004; Rezende et al. (2005) and sometimes with type F (Ribeiro et al. 2006; Mello et al. 2007).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
57
However, in Alagoas, genotype A was accompanied by genotype C. It is emphasized that
infection due to genotype A was also found in a patient of Asian ethnicity, concordant with the
report by Stinik et al (2004).
The finding of type C was an unexpected result, considering that this type predominates in
Asia and that the population of Asian ethnicity living in Alagoas is only 0.1% of the whole
population, according to the Brazilian Institute for Geography and Statistics (IBGE, 2000). In
Brazil, infections due to this genotype have been reported by Bottecchia et al (2007) and Oliveira
et al. (2008) at low frequencies and by Stinik et al. (2004) at a high frequency, but among patients
of Asian descent.
The identification of genotype D in Alagoas was a result not expected, since in Salvador-BA
Ribeiro et al. (2006) did not identify any infection that genotype in 76 patients investigated.
However, demonstrates concordance with the distribution pattern for this genotype in Brazil with
respect to the frequency identified. It predominates in the southern and southeastern regions,
which are the regions where Italian immigration took place (Rezende et al. 2005; Carrilho et al.
2004; Mello et al. 2007), and its frequency is lower in the northeastern region (Lyra et al. 2005;
Mello et al. 2007).
The genotype F did not follow the national distribution pattern, in which infections due to
this
type
are
most
frequent
in
the
northern
and
northeastern
regions
(Viana et al. 2005; Ribeiro et al. 2006; Mello et al. 2007). However, the present result is
concordant with Rezende et al. (2005) in São Paulo and Mello et al. (2007) in Santa Catarina that
found at low frequency.
The majority of the infections due to genotype A presented an asymptomatic clinical condition,
with low concentrations of HBV DNA (≤ 300 copies/ml) and seroconversion of HBeAg. These
results agree with the classical description from Hoofnalge et al (1987). Among communities of
descendents from Africans in Mato Grosso do Sul, Motta-Castro et al. (2005) also reported similar
results in relation to the HBeAg/anti-HBe system. According to Lai et al. (2003), this profile is
commonly observed in regions with low to medium endemicity, when the infection is acquired
during adolescence or at the start of adulthood, and is characterized by the residual or nonreplicating phase of HBV infection.
This study provides the first record of the circulation of genotypes A, C, D and F in
Alagoas, Northeastern Brazil. Genotype A was predominant and most of the cases of infection
were identified in asymptomatic individuals.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
58
REFERENCES
Anjos LC. Marcadores de replicação do vírus da hepatite B: comparação de métodos de biologia
molecular, de sorologia e imunohistoquímuca. São Paulo, 1999. (Dissertação de Mestrado –
Facultade de Medicina da Universidade de São Paulo).
Araújo NM, Mello FCA, Yoshida CFT, Niel C, Gomes SA 2004. High proportion of subgroup
A’(genotype A) among Brazilian isolates of hepatitis B virus. Archives of Virology 49:1383-1395.
Arauz-Ruiz P, Norder H, Robertson BH, Magnius LO 2002. Genotype H: a new ameridian
genotype of hepatitis B vírus revealed in Central America. Journal of General Virology 83:20592073.
Bottecchia M, Souto FJD, Ó KMR, Amendola M, Brandão CE, Niel C, Gomes SA 2008.
Hepatitis B virus genotypes and resistance mutations in patients under long term lamivudine
therapy: characterization of genotype G in Brazil. BMC Microbiology 8: (11)1471-1480.
Bozdayi AM, Bozkaya H, Türkyilmaz AR, Saýodlu M, Cetinkaya H, Karayalçin S, Yurdaydin C,
Uzunalimoğlu Ö 2001. Nucleotide divergences in the core promoter and precore region of
genotype D hepatitis virus in patients with persistently elevated or normal ALT levels. Journal of
Clinical Viroloy 21: 91-101.
Brazilian Institute of Geography and Statistics 2000 [cited 2009 Feb 27].Available from
<http://www.sidra.ibge.gov.br/bda/tabela/listabl.asp?z=t&c=136>.
Candotti D, Opare-sem O, Rezvan H, Sarkodie F, Allain JP 2006. Molecular and serological
characterization of hepatitis B virus in deferred Ghanaian blood donors with and without elevated
alanine aminotransferase. Journal of viral hepatology 13: 715-24.
Carrilho FJ, Moraes CR, Pinho JRR, Mello IMVGC, Bertolini DA, Lemos MF, Moreira RC,
Bassit LC, Cardoso RA, Santos GR, Silva LC 2004. Hepatitis B virus infection in haemodialysis
Centres from Santa Catarina State, Southern Brazil. Predictive risk factors for infection and
molecular epidemiology. BMC Public Health 4:13.
Chauhan R, Kazim SNBhattacharjee J, Sakhuja P, Sarin SK 2006. Basal core promoter, precore
region mutations of HBV and their association with e antigen, genotype, and severity of liver
disease in patients with chronic hepatitis B in India. Journal of Medical Virology 78: 1047-54.
Chou YC, Yu MW, Wu CF, Yang, SY, Lin CL, Liu CJ, Shih WL, Chen PL, Liaw YF, Chen CJ
2008. Temporal relationship between hepatitis B vírus enhancer II/basal core promoter sequence
variation and risk of hepatocellular carcinoma. Gut 57:91–97.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
59
Chu CJ, Hussain M, Lok ASF 2002. Hepatitis B virus genotype B is associated with earlier
HBeAg seroconversion compared with hepatitis B virus genotype C. Gastroenterology 122: 17561762.
Devesa M, Rodriguez C, Lei NG, Liprandi F, Pujol FH 2004. Clade analysis and surface antigen
polymorphism of hepatitis B vírus American genotypes. Journal of Medical Virology 72: 377-84.
Hoofnagle JH, Shafritz DA, Popper H 1987. Chronic type B hepatitis and the "healthy" HBsAg
carrier state. Hepatology 7: 758-763.
ICTVdb-The Universal Virus Database, version 4. 2006. [cited 2008 Jul 31]. Available from:
<www.ncbi.nlm.nih.gov/projects/genotyping/formpage.cgi>.
Kaneko S. Feinstone SM. Miller RH 1989. Rapid and sensitive method for the detection of serum
hepatitis B virus DNA using the polymerase chain reaction technique. Journal of Clinical
Microbiology 27(9):1930-1933.
Kato H, Orito E, Gish RG, Bzowej N, Newsom M, Sugauchi F, Suzuki S, Ueda R, Miyakawa Y,
Mizokami M 2002. Hepatitis B e antigen in sera from individuals infected with hepatitis B virus
of genotype G. Hepatology 35:(4) 922-929.
Kumar A, Kumar SI, Pandey R, Naik S, Aggarwal R 2005. Hepatitis B virus genotype A is more
often associated with severe liver disease in northern India than is genotype D. Indian J
Gastroenterology 24(1):19-22.
Lai CL, Ratziu V, Yuen M-F, Polynard T. 2003. Viral hepatitis B. The Lancet 362: 2089-2094.
Lyra AC, Pinho JRR, Mello IMVGC, Malta FM, Gomes MMS, Bisceglie AMD, Lyra LGC 2005.
Distribution of hepatitis B virus genotypes among patients with acute viral hepatitis..J Clin
Gastroenterol 39(1): 81.
Mello FCA, Souto FJD, Nabuco LC, Nogueira CAV, Coelho HSM, Franz HCF, Saraiva JCP,
Virgolino HA, Motta-Castro ARC 2007. Hepatitis B virus circulating in Brazil: Molecular
characterization of genotype F isolates. BMC Microbiology 7:103.
Motta-Castro ARC, Martins RMB, Yoshida CFT, Teles SA, Paniago AM, Lima KMB, Gomes SA
2005. Hepatitis B virus infection in isolated Afro-Brazilian communites. Journal of Medical
Virology 77(2): 188-193.
Norder H, Hammas B, Löfdahl S, Couroucé A-M, Magnius LO. 1992. Comparison of the amino
acid sequences of nine different serotypes of hepatitis B surface antigen and genomic
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
60
classification of the corresponding hepatitis B virus strains. Journal of general Virology 73: 12011208.
Norder H, Couroucé A-M, Magnius LO 1994. Complete genomes, phylogenetic relatedness, and
structural proteins of six strains of the hepatitis B virus, four of which represent two new
genotypes. Virology 198: 489-503.
Okamoto H, Tsuda F, Sakugawa H, Sastrosoewignjo RI, Imai M, Miyakawa Y, Mayumi M 1988.
Typing Hepatitis B vírus by homology in nucleotide sequence: comparison of surface antigen
subtypes. Journal of general Virology 69:2575-2583.
Oliveira CM, Farias IP, Fonseca JCF, Brasil LM, Souza R, Astolfi-Filho S. 2008. Phylogeny and
molecular genetic parameters of different stages of hepatitis B virus infection in patients from the
Brazilian Amazon. Arch Virol May 153: 823-30.
Olyaee ASB, Forooshani RS, Adeli A, Mahboudi F , Sabahi F, Nafisi,H, Zali, MR, Azizi M 2005.
Complete genomic sequence and phylogenetic relatedness of hepatitis B vírus isolates from Iran.
Journal of Medical Virology 76: 318-26.
Paraná R, Almeida D 2005. HBV epidemiology in Latin America. Journal of Clinical Virology,
34(1):130-133.
Rezende REF, Fonseca BAL, Ramalho LNZ, Zucoloto S, Pinho JRR, Bertolini DA, Martinelli
ALC 2005. The precore mutation is associated with severity of liver damage in Brazilian patients
with chronic hepatitis B. Journal of Clinical Virology 32: 53-59.
Ribeiro NRC, Campos GS, Ângelo ALD, Braga EL, Santana N, Gomes MMS, Pinho JRR, De
Carvalho WA, Lyra LGC, Lyra AC 2006. Distribution of hepatitis B virus genotypes among
patients with chronic infection. Liver International. 26: 636-642.
Sánchez LV, Maldonado M, Bastidas-Ramírez BE, Norder H, Panduro A 2002. Genotypes and Sgene variability of Mexican hepatitis B vírus strains. Journal of Medical Virology 68: 24-32.
Sanchez-Tapias JM, Costa J, Mas A, Bruguera M, Rodes M 2002. Influence of hepatitis B virus
genotype on the long-term outcome of chronic hepatitis B in Western patients. Gastroenterology
123: 1848-56.
Sanger F, Coulson AR 1975. A rapid method for determining sequences in DNA by primed
synthesis with DNA polymerase. Journal of Molecular Biology 94: 441-448.
Schaefer S 2005. Hepatitis B virus: significance of genotypes. Journal of Viral Hepatitis 12: 111124.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
61
Sitnitk R, Pinho JRR, Bertolini DA, Bernardini AP, da Silva LC, Carrilho FJ 2004. Hepatitis B
Virus Genotypes and Precore and Core Mutants in Brazilian Patients. Journal of Clinical
Microbiology 42: 2455-2460.
Stuyver L. De Gendt S, Geyt CV, Zoulim F, Fried M, Schinazi RF, Rossau R 2000. A new
genotype of hepatitis B virus: complete genome and phylogenetic relatedness. Journal of General
virology 81: 67-74.
Teles SA, Martins RMB, Gomes AS, Gaspar AMC, Araújo NM, Souza KP, Carneiro MAS,
Yoshida CFT 2002. Hepatitis B virus transmission in Brazilian hemodialysis units: Serological
and molecular follow-up. Journal of Medical Virology 68(1): 41-49.
Viana S, Paraná R, Moreira RC, Compri AP, Macedo V 2005. High prevalence of hepatitis B
virus and hepatitis D virus in the western Brazilian amazon. Am J Trop Med Hyg 73: 808-814.
Yotsuyanagi H, Hino K, Tomita E, Toyoda J, Yasuda K, Iino S 2002. Precore and core promoter
mutations, hepatitis B virus DNA levels and progressive liver injury in chronic hepatitis B.
Journal of Hepatology 37: 355-363.
Yuen MF, Sablon E, Tanaka Y, Kato T, Mizokami M, Doutreloigne J, Yuan HJ, Wong DKH,
Sum SM, Lai CL 2004. Epidemiological study of hepatitis B virus genotypes, core promoter and
precore mutations of chronic hepatitis B infection in Hong Kong. Journal of Hepatology 41: 119125.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
62
7.0 ARTIGO II
Mutações pré-core (G1896A) e BCP (A1762T/G1764A) no vírus da hepatite B em pacientes
de Alagoas, Brasil)
Alba M.X. Eloy1,2; Marcílio L. Figueiredo3; Regina C. Moreira3; Jéfferson L.A. Silva4, Maria
R.C.D. Coêlho4,5
1
Instituto de Ciências Biológicas e da Saúde (ICBS) da Universidade Federal de Alagoas (UFAL)
2
Laboratório de Análises Clínicas do Hospital Universitário Prof. Alberto Antunes (UFAL)
3
Setor de Hepatites Virais do Instituto Adolfo Lutz de São Paulo (IAL-SP)
4.
Setor de Virologia do Laboratório de Imunopatologia Keizo-Asami (LIKA) da Universidade Federal de
Pernambuco (UFPE)
5
Departamento de Fisiologia e Farmacologia da Universidade Federal de Pernambuco (UFPE)
Endereço correspondência para Alba Maria Xavier Eloy:
Rua Barão José Miguel nº 249/601 Farol ,Maceió-AL
CEP 57055-160
Tel. 82 99684084
e-mail: [email protected]
RESUMO
A mutação da região pré-core, G1896A é detectada com maior freqüência nos genótipos B,C,D,E
e F, enquanto que, as mutações na região basal do promotor core (BCP) A1762T e G1764A são
descritas em todos os genótipos. O objetivo do estudo foi investigar os genótipos e as mutações
pré-core e BCP em pacientes HBsAg e anti-HBc positivos, acompanhados pela carga viral, perfil
HBeAg/anti-HBe e nível de alanina aminotransferase (ALT). Foram analisados 17 portadores
assintomáticos e 16 pacientes com hepatite B crônica. Os genótipos identificados foram: A
(84,4%), C (9,4%), D (3,1%) e F (3,1%). No genótipo A, a mutação pré-core foi detectada em
3,8% (1/26) e as BCP em 52,4% (11/21). No genótipo C foi identificada apenas a mutação BCP
em 33,3% (1/3) e não foram identificadas mutações nos genótipos D e F. O estudo identificou
pela primeira vez a presença destas mutações no genótipo A no Estado de Alagoas, Brasil. As
mutações BCP foram detectadas equitativamente nos portadores assintomáticos e com hepatite
crônica, independentemente da carga viral e nível sérico de ALT. Os resultados da pesquisa
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
63
contribuíram para ampliar as informações envolvendo o genótipo A, servindo de referência para
novas investigações.
Palavras chaves: Mutação pré-core, Mutação no promotor core, vírus da hepatite B.
INTRODUÇÃO
A variação genética do HBV é devida em parte, à falta de um mecanismo de revisão
envolvendo as atividades da DNA polimerase durante o processo de transcrição reversa do RNA
pré-genômico, favorecendo o aparecimento de mutações pontuais, deleções ou inserções1.
Naturalmente são encontradas variantes das regiões pré-S/S, pré-C/C e P, resultando uma
população de vírus com genomas heterogêneos, denominados por quasispecies2.
A transição de G para A no nucleotídeo (nt) 1896 cria um códon de terminação prematuro
na região pré-core que previne a síntese do antígeno e do vírus da hepatite B (HBeAg), reduzindo
a replicação viral3. Por outro lado, a presença de timina no nt 1858, formando um par de base (AT) com a adenina do nt 1896, torna o sinal de encapsidação do RNA pré-genômico mais forte,
aumentando a eficiência da replicação, apesar da presença de anti-HBe. Os genótipos B, C, D e E,
possuem timina no nt 1858, o F possui citosina ou timina e o A geralmente apresenta citosina. O
que justifica a maior freqüência, dessa mutação nos genótipos B, C, D, E e F4.
As mutações na região basal do promotor core (BCP) A1762T e G1764A são descritas
independentemente da soroconversão do HBeAg5,6 e são comuns em diferentes genótipos7,8. A
ocorrência dessas mutações isoladas ou acompanhadas da mutação pré-core G1896A, tem sido
associada com hepatite B crônica ativa em infecções HBeAg negativo/anti-HBe positivo5.
O objetivo desse estudo foi investigar os genótipos e a presença de mutações pré-core
G1896A e BCP A1762T/G1764A em pacientes com infecção crônica pelo HBV, caracterizando-a
pela carga viral, perfil HBeAg/anti-HBe e nível sérico da ALT.
ZAIDAN, A.M. E.
64
Caracterização genética do vírus da hepatite B...
PACIENTES E MÉTODOS
Pacientes
Durante o período de setembro de 2006 a outubro de 2007 foram selecionados 33
pacientes (20 homens e 13 mulheres) com sorologia positiva para
HBsAg e
anti-HBc,
provenientes dos centros de referência em hepatites virais do Estado de Alagoas. Foram 17
portadores assintomáticos e 16 pacientes com hepatite B crônica, confirmada histologicamente.
Após o preenchimento de um questionário com os dados demográficos e assinatura do
termo de consentimento livre e esclarecido, a coleta de sangue foi realizada por meio de punção
venosa, sem anticoagulante.
Dosagem de alanina aminotransferase
Foi utilizado kit comercial (Abbott Laboratórios do Brasil) executado de acordo com as
instruções do fabricante. Considerou-se como valor normal (N) quando a concentração de ALT
foi menor que 1,5 vezes o limite normal superior (LNS, 55U/L) e de elevado (E) quando maior ou
igual a 1,5 x LNS 9.
Marcadores sorológicos
Os marcadores HBeAg/anti-HBe (Symbiosis Diagnóstica Ltda São Paulo, Brasil) foram
pesquisados por ensaio imunoenzimático (ELISA).
Extração e amplificação parcial do gene S e região pré-core
O DNA viral foi extraído por meio do tratamento do soro com isotiocianato de guanidinafenol (LGC Biotecnologia), precipitado com etanol absoluto gelado e ressuspendido em 50 µL de
água livre de RNASE e DNASE (Ludwig Biotec)7.
A amplificação parcial do gene S e região pré-core foram realizadas segundo protocolo de
Sitnik et al.7, utilizando para o gene S, os primers: FHBS1 (5’GAGTCTAGACTCGTGGTGGACTTC3’),
RHBS1 (5’AAATKGCAC TAGTAAACT3’) no primeiro ciclo de amplificação (PCR I) e FHBS2
(5’CGTGGTGGACTTCTCTCAATTTTC3’),
RHBS2
(5’GCCARGAGAAACGGRCTGAGGCCC3’),
para
reamplificação. Para a região pré-core foram utilizados os primers descritos por Takahashi et al.10
EP1.1 (5’TCATGGAGACCACCG TGAAG3’) e EP1.2 (5’GGAAAGAAGCAGAGGCAA3’) para o primeiro
ciclo e EP2.1 (5’CATAAGAGGCTCTGGACT3’) e EP2.2 (5’GGCAAAAAAGAGAGTAACTC3’) para o
segundo ciclo. Em cada tubo de PCR foi adicionado 10 µL de DNA viral extraído mais 90 µL de
uma solução pré-mix (10mM tampão Taq DNA polimerase, 50mM KCl, 1,5mM MgCl2, 150µM
de cada dNTP, 20 pmol/µL de cada primer e 2,5U taq polimerase). A reação de amplificação dos
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
65
dois ciclos de PCR foi realizada nas seguintes condições: 94ºC, 20s, seguido por 30 ciclos de
94ºC, 20s; 56ºC, 20s; 72ºC, 30s e uma etapa final de extensão a 72ºC, 7 min, para o gene S e
94ºC, 30s, seguido por 30 ciclos de 94ºC, 30s; 56ºC, 30s; 72ºC, 40s e uma etapa final de extensão
a 72ºC, 5 min, para a região pré-core.
Carga viral - Titulação do DNA HBV
Para estimar a carga viral, amostras de soro, puros e diluídos, foram submetidas ao
protocolo de extração do DNA viral com NAOH 0,5M seguido diretamente de PCR da região
core
como
descrito
por
Kaneko
et
al.11,
utilizando
os
primers1763F(5`GCTTTGGGGCATGGACATTGACCCGTATAA3`),2032R(5`CTGACTACTAATTCCCTGG
ATGCTGGGTCT3`),
para o primeiro ciclo e 1778-F(5`GACGAATTCCATTGACCCGTATAAAGAATT3`) e
2017R
(5`ATGGGATCCCTGGATGCTGGGTCTTCCAAA3`),
para o segundo ciclo. Em tubos contendo 10 µL
de amostras de soro puros e diluídos (10-2, 10-4, 10-6, 10-8 e 10-10), com água milli Q autoclavada,
foram adicionados 2,5µl de NAOH 0,5M. Após uma hora a 37ºC foram acrescentados 2,5 µL de
HCL 0,5M e 85 µL de pré-mix contenco10mM tampão taq polimerase, 50mM KCl, 1,5mM
MgCl2, 150µM de cada um dos quatro dNTP, 20 pmol/µL de cada primer e 2,5U taq polimerase.
A reação de amplificação foi realizada sob as seguintes condições: 94ºC, 60s; seguido por 30
ciclos de 94ºC, 60s; 45ºC, 60s; 72ºC, 90s e ao final uma etapa de extensão a 72ºC, 7 min.
A carga viral (genomas/mL) foi calculada multiplicando-se o título da reação,
correspondendo a mais alta diluição do soro com PCR positiva pelo limite de detecção do método
(3 x 102 genomas/mL), como descrito por Anjos12.
Identificação dos fragmentos genômicos
Os fragmentos genômicos amplificados foram visualizados por meio de corridas
eletroforéticas em gel de agarose a 2% contendo brometo de etídio a 1%, como corante.
Reação de seqüenciamento
Para o seqüenciamento direto13, os produtos de amplificação foram submetidos a uma
nova amplificação, utilizando os primers FHBS2 e RHBS2, para o gene S e EP2.1 e EP2.2, para a
região pré-core e o “DYEnamic EDTye Terminator Cicle Sequencing kit”, adaptado para o
seqüenciador automático MegaBace 500® (GE Healthcare).
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
66
Análise das seqüências
A análise dos genótipos foi realizada por comparação entre as seqüências obtidas com as
seqüências de diferentes genótipos de HBV depositadas no Genbank. A classificação dos genótipos
foi
confirmada
pela
ferramenta
Genotyping
disponível
no
site
do
NCBI
(http://www.ncbi.nlm.nih.gov/projects/genotyping/formpage.cgi). As mutações foram identificadas
pelo alinhamento das seqüências de nucleotídeos obtidas no estudo e comparadas com uma
seqüência do vírus selvagem. Para estas análises foram utilizados os programas EditSeq e
Megalign do pacote DNAstar (Lasergene Inc., Madison, WI, EUA).
RESULTADOS
A tabela 1 mostra as características demográficas, perfil HBeAg/Anti-HBe, nível sérico da
ALT, carga viral, genótipos e mutações, em 17 portadores assintomáticos e 16 com hepatite B
crônica.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
67
Tabela 1. Dados demográficos e características da infecção pelo vírus da hepatite B em portadores
assintomáticos e hepatite crônica. Alagoas-Brasil, Setembro 2006 a Outubro 2007.
Pacientes
Idade
ALT
HBeAg /
Carga viral
(n = 33)
(Sexo)
(U/L)
anti-HBe
(cópias/mL)
Portador
43 (M)
E2
-/+
3 x 102
-/+
4
8
10
2
assintomático
(n = 17)
14 (M)
18 (F)
31 (F)
32 (F)
49 (F)
21 (M)
28 (F)
+/-
N
-/+
N
N
N
3 x 10
3 x 10
3 x 10
2
27 (M)
31 (M)
C
-
-
C
-
-
D
-
-
A
nd
-
+/-
A
nd
-
3 x 10
2
-/-
≤ 3 x 10
A
+
-
2
A
+
nd1
A
+
-
A
+
-
A
+
-
-/+
3 x 10
4
3 x 10
8
2
-/+
≤ 3 x 10
A
-
-
-/+
3 x 10
2
A
-
-
3 x 10
4
A
-
nd
3 x 10
4
A
-
-
8
A
-
-
-/+
E
-
-
-/+
N
-
nd
≤ 3 x 102
N
F
A
-/+
N
Pré-core
4
N
N
BCP
≤ 3 x 10
31 (F)
E
Mutação
-/+
3 x 10
41 (F)
-/+
32 (M)
N
-/+
3 x 10
36 (M)
E
+/-
3 x 102
A
+
-
+/-
4
A
+
-
6
A
+
-
3x0
10
A
+
-
3x0
10
A
+
-
3 x 10
6
A
+
-
3 x 10
8
A
-
-
12
A
-
-
A
-
+
54 (F)
29 (M)
38 (M)
31 (M)
33 (F)
30 (M)
24 (M)
14 (M)
38 (M)
32 (M)
30 (M)
28 (M)
46 (M)
46 (F)
47 (F)
1
N
-/+
-/+
41 (F)
(n = 16)
N
3 x 10
N
32 (M)
Crônica
3
26 (M)
25 (F)
Hepatite
E
Genótipo
2
N
N
-/+
E
-/+
N
-/+
N
-/+
E
-/+
E
-/+
-/+
N
N
N
N
E
N
N
3
3 x 10
3x0
3 x 10
12
2
-/+
≤ 3 x 10
A
-
-
-/+
2
A
-
-
3 x 10
2
-/+
≤ 3 x 10
C
+
-
-/+
4
A
Nd
-
10
A
Nd
-
2
+/-
N
3 x 10
3 x 10
3 x 10
-/+
≤ 3 x10
A
Nd
-
-/+
2
nd
Nd
-
nd = não determinada; E= Elevada; N= Normal.;
3 x 10
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
68
Os genótipos foram investigados em 32 seqüências. Sendo identificado em 84,4% (27/32)
o genótipo A, em 9,4% (3/32) o C, em 3,1% (1/32) para ambos os genótipos D e F (Figura 1). A
presença de timina na posição 1858 foi identificada em 50% (13/26) das seqüências do genótipo
A e em 33,3% (1/3) do genótipo C, sendo ausente nos genótipos D e F.
3.1%
3.1%
9.4%
A (n=27)
C (n=3)
D (n=1)
F (n=1)
84.4%
Figura 1 Genótipos Identificados em Alagoas-Brasil. Setembro 2006 a Outubro 2007.
A mutação pré-core G1896A foi pesquisada em 31 seqüências, sendo identificada em um
paciente com hepatite crônica pelo HBV genótipo A, que apresentou carga viral de
3x1012cópias/mL, concentração sérica normal de ALT e HBeAg-negativo e anti-HBe-positivo. As
mutações BCP A1762T e G1764A foram investigadas em 26 seqüências, sendo 21 do genótipo A,
três do C, uma do D e uma do F. Foram identificadas em 52,4% (11/21) das infecções pelo
genótipo A, 50% (5/10) em portadores assintomáticos e 54,5% (6/11) em pacientes com hepatite
crônica. No genótipo C foram detectadas em 33,3% (1/3).
DISCUSSÃO
O polimorfismo nucleotídico que ocorre naturalmente ao longo do curso das infecções
pelo HBV é responsável pelo aparecimento de mutações pontuais no genoma viral. As
combinações dessas mutações podem ter uma pluralidade de significados clínicos em infecções
por diferentes genótipos.
As mutações pré-core G1896A/C1899A e BCP A1762T/G1764A são as mais freqüentes e
por isso vêm sendo investigadas intensivamente
4,6,10,13-19
. Porém, a maioria destes estudos
envolve pacientes asiáticos com infecções pelos genótipos B e C do HBV
9,20
. No Brasil, a
literatura contemplando os genótipos A, D e F, ainda é escassa, sendo este o primeiro trabalho
descrevendo mutações em pacientes portadores da infecção pelo HBV em Alagoas, Brasil.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
69
O genótipo A geralmente possui citosina (C) na posição 1858 de acordo com os estudos de
De Castro et al.21 e Sitnik et al. 7, que encontraram citosina em 100% e 90% dos isolados deste
genótipo, respectivamente. No entanto, em nosso estudo a presença da citosina foi observada em
50% dos isolados. Essa freqüência foi próxima a 68,4%, encontrada por Rezende17.
A circulação do mutante pré-core G1896A do genótipo A é rara e mostra uma relação com
a presença de citosina no nt 1858
7,13,17,21
. Em nossa pesquisa, também encontramos uma baixa
freqüência dessa mutação, embora a presença de timina tenha sido encontrada em 50% das
seqüências do genótipo A investigadas.
A timina forma um par de base com a adenina na posição 1896, tornando o sinal de
encapsidação do RNA pré-genômico mais forte, favorecendo a replicação viral13. A presença de
mutação pré-core em um paciente com carga viral alta pode ser justificada pela substituição de
citosina por timina no nt 1858, embora não tenha sido possível identificar a referida substituição.
.
A freqüência da mutação BCP A1762T/G1764A encontrada no genótipo A, mostra uma
concordância com os achados de Sitnik et al.7, em relação à taxa de positividade de 62% (31/50).
Porém, difere dos resultados encontrados por De Castro et al.21 cuja freqüência foi de 20% (2/10).
Sua distribuição de forma equitativa entre os portadores assintomáticos e com hepatite crônica
independentemente do nível sérico de ALT e carga viral, parece não interferir no curso clínico das
infecções pelo HBV. No entanto, em estudos com outros genótipos as mutações BCP foram
relacionadas com maior atividade e freqüência da hepatite B crônica. Sendo consideradas um dos
fatores virais preditores e independentes, de risco para o desenvolvimento do carcinoma
hepatocelular (HCC) 6,18,19, 21.
A identificação da única mutação A1762T/G1764A no genótipo C em paciente de origem
não asiática difere do estudo de Sitnik et al.7 que encontraram esta mutação em 76,9% em
pacientes asiáticos. Ressaltando que no Brasil a maioria dos estudos não detectou esse genótipo
17,22-29
, sendo detectado apenas por Bottecchia et al.30 e Oliveira et al.31.
O estudo identificou pela primeira vez em Alagoas/Brasil a presença das mutações pré-
core G1896A e BCP A1762T/G1764A no genótipo A em infecções pelo HBV. A freqüência de
citosina na posição 1858 não apresentou relação com a baixa freqüência da mutação pré-core no
genótipo A. As mutações BCP foram detectadas equitativamente nos portadores assintomáticos e
com hepatite crônica, a despeito da carga viral e nível sérico de ALT. Os resultados da pesquisa
contribuíram para ampliar as informações envolvendo o genótipo A, servindo de referência para
novas investigações.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
70
Contribuição dos autores
(1) Contribuiu substancialmente para a concepção e planejamento, (2) Contribuí na análise e
interpretação dos dados (3) Contribuí significativamente na elaboração do rascunho ou na revisão
crítica do conteúdo; e (4) Participei da aprovação da versão final do manuscrito.
(1) Alba M.X. Eloy, Regina C. Moreira, Maria R.C.D. Coêlho.
(2) Alba M.X. Eloy, Regina C. Moreira, Marcílo L. Figueiredo, Maria R.C.D. Coêlho.
(3) Alba M.X. Eloy, Regina C. Moreira, Marcílo L. Figueiredo, Jéfferson L.A. Silva, Maria
R.C.D. Coêlho.
(4) Alba M.X. Eloy, Regina C. Moreira, Marcílo L. Figueiredo, Jéfferson L.A. Silva, Maria
R.C.D. Coêlho.
Agradecimentos
Laboratório de Biotecnologia do Centro de Ciências Agrárias/Universidade Federal de Alagoas,
Setor de Biologia Molecular do Laboratório de Imunopatologia Keizo Asami da Universidade
Federal de Pernambuco, Laboratório de Hepatites Virais do Instituto Adolfo Lutz.
Financiamento
FAPEAL por meio da concessão de uma bolsa de doutorado.
Conflito de interesses
Os autores declaram não haver interesses pessoais, comerciais, políticos, acadêmicos ou
econômicos relacionados ao conteúdo deste artigo científico.
Aprovação ética
A pesquisa foi aprovada pelo Comitê de Ética em pesquisa da Universidade Federal de Alagoas
(UFAL) segundo protocolo de pesquisa n 000906/2005-98.
REFERÊNCIAS
1.Summers J, Mason WS. Replication of the genome of a hepatitis B-like virus by reverse
transcription of an RNA intermediate. Cell 1982, 29: 403-15.
2.Ballard Al, Boxall EH. Colourimetric point mutation assay: for detection of precore mutants of
hepatitis B. J Virol Methods 1997, 67: 143-52.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
71
3.Carman WF et al. Mutation preventing formation of hepatitis B virus (HBV) e antigen in
patients with chronic hepatitis B infection. Lancet 1989, 9 (8663): 588-91.
4.Yotsuyanagi H, Hino K, Tomita E, Toyoda J, Yasuda K, Iino S. Precore and core promoter
mutations, hepatitis B virus DNA levels and progressive liver injury in chronic hepatitis B. J
Hepatol 2002, 37: 355-63.
5.Okamoto H et al. Hepatitis B virus with mutations in the core promoter for an e antigennegative phenotype in carriers with antibody to e antigen. J Virol 1994, 68 (12): 8102-10.
6.Bozdayi AM et al. Nucleotide divergences in the core promoter and precore region of genotype
D hepatitis virus in patients with persistently elevated or normal ALT levels. J Clin Virol 2001,
21: 91-101.
7.Sitnik R, Pinho JRR, Bertolini DA, Bernardini AP, Silva LC, Carrilho FJ. Hepatitis B virus
genotypes and precore and core mutants in brasilian patients. J Clin Microbiol 2004, 42: 6, 2455460.
8.Candotti D, Opare-Sem O, Rezvan H, Sarkodie F, Allain JP. Molecular and serological
characterization of hepatitis B virus in deferred Ghanaian blood donors with and without elevated
alanine aminotransferase. J Viral Hepat 2006, 13 (11):715-24.
9.Lai CL, Ratziu V, Yuen M-F, Polynard T. Viral hepatitis B. Lancet 2003, 362: 2089-94.
10.Takahashi K et al. The precore/core promoter mutant (T1762A1764) of hepatitis B virus: clinical
significance and an easy method for detection. J Gen Virol 1995, 76: 3159-164.
11.Kaneko S, Feinstone SM, Miller RH. Rapid and sensitive method for the detection of serum
hepatitis B virus DNA using the polymerase chain reaction technique. J Clin Microbiol 1989, 27
(9): 1930-33.
12. Anjos LC. Marcadores de replicação do vírus da hepatite B: comparação de métodos de
biologia molecular, de sorologia e imunohistoquímuca. São Paulo, 1999. (Dissertação de
Mestrado – Facultade de Medicina da Universidade de São Paulo).
13.Sanger F, Coulson AR. A rapid method for determining sequences in DNA by primed
synthesis with DNA polymerase. J Mol Biol 1975, 94: 441-48.
14.Li JS, Tong SP, Wen YM, Vitvitski L, Zhang Q Trepo C. Hepatitis B virus genotype A rarely
circulates as an HBe-minus mutant: possible contribution of a single nucleotide in the precore
region. J Virol 1993, 67(9): 5402-410.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
72
15.López JL et al. Deteccion y caracterizacion de mutantes pre-core del virus de la hepatitis B
(HBV) en pacientes cronicamente infectados. Acta Gastroenter Latinoamer 1995, 25: 85-90.
16.Yuen MF et al. Epidemiological study of hepatitis B virus genotypes, core promoter and
precore mutations of chronic hepatitis B infection in Hong Kong. J Hepatol 2004, 41: 119-25.
17.Rezende REF et al. The precore mutation is associated with severity of liver damage in
Brazilian patients with chronic hepatitis B. J Clin Virol 2005, 32: 53-59.
18.Tong S. Mechanism of HBV genome variability and replication of HBV mutants. J Clin Virol
2005, 34: 134-38.
19.Tong MJ, Blatt LW, Kao J-H, Cheng JT, Corey GW. Basal core promoter T1762/A1764 and
precore A1896 gene mutations in hepatitis B surface antigen-positive hepatocellular carcinoma: a
comparison with chronic carriers. Liver Int 2007, 1356-363.
20.Chou YC et al. Temporal relationship between hepatitis B virus enhancer II/basal core
promoter sequence variation and risk of hepatocellular carcinoma. Gut 2008, 57:91–97.
21.Schaefer S. Hepatitis B virus: significance of genotypes. J Viral Hepat 2005, 12: 111-14.
22.De Castro L, Niel C, Gomes SA. Low frequency of mutations in the core promoter and precore
regions of hepatitis B virus in anti-HBe positive Brazilian carriers. BMC Microbiol 2001, 1:10.
23.Teles AS et al. Hepatitis B virus transmission in Brazilian hemodialysis units: Serological and
molecular follow-up. J Med Virol 2002, 68: 41-49.
24.Araujo NM, Mello FCA, Yoshida CFT, Niel C, Gomes SA. High proportion of subgroup A’
(genotype A) among Brazilian isolates of hepatitis B virus. Arch Virol 2004, 149:1383-95.
25.Carrilho FJ et al. Hepatitis B virus infection in Haemodilysis Centres from Santa Catarina
State, Southern Brazil. Predictive risk factors for infection and molecular epidemiology. BMC
Public Health 2004, 4:13.
26.Motta-Castro ARC et al. Hepatitis B virus infection in isolated Afro-Brazilian communities. J
Med Virol 2005, 77(2): 188-93.
27.Ribeiro NRC et al. Distribution of hepatitis B virus genotypes among patients with chronic
infection. Liver Int 2006, 26: 636-42.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
73
28.Mello FCA et al. Hepatitis B virus circulating in Brazil: Molecular characterization of
genotype F isolates. BMC Microbiol 2007, 7:103.
29.Gomes-Gouvêa MS et al. Hepatitis D e B virus genotypes in chronically infected patients from
the Eastern Amazon Basin. Acta Trop 2008, 106 (3): 149-55.
30.Bottecchia M et al. Hepatitis B virus genotypes and resistance mutations in patients under long
term lamivudine therapy: characterization of genotype G in Brazil. BMC Microbiol 2008, 8: (11).
31.Oliveira CM, Farias IP, Fonseca JCF, Brasil, LM, Souza R, Astolfi-Filho S. Phylogeny and
molecular genetic parameters of different stages of hepatitis B virus infection in patients from the
Brazilian Amazon. Arch Virol 2008, 153: 823-
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
74
8.0 VERSÃO EM INGLÊS DO ARTIGO II
Pre-core mutation (G1896A) and BCP (A1762T/G1764A) in the hepatitis B virus in patients
of Alagoas, Brazil)
Alba M.X. Eloy1,2; Marcílio L. Figueiredo3; Regina C. Moreira3; Jéfferson L.A. Silva4, Maria
R.C.D. Coêlho4,5
1
Institute of Biological and Health Sciences (ICBS), Federal University of Alagoas
2
Clinical Analysis Laboratory, Prof. Alberto Antunes University Hospital, Federal University of
Alagoas
3
Viral Hepatitis Sector, Adolfo Lutz Institute, São Paulo
4
Virology Sector, Keizo Asami Immunopathology Laboratory (LIKA), Federal University of
Pernambuco
5
Department of Physiology and Pharmacology, Federal University of Pernambuco
Address for correspondence:
Alba Maria Xavier Eloy:
Rua Barão José Miguel nº 249/601
Farol, Maceió-AL, CEP 57055-160
Tel. +55 82 99684084
e-mail: [email protected]
ABSTRACT
Mutation of the precore region (G1896A) is most frequently detected in genotypes B, C, D, E and
F, while mutations in the basal region core promoter (BCP) (A1762T/G1764A) have been
described in all genotypes. The aim of this study was to investigate the genotypes and precore and
BCP mutations in HBsAg and anti-HBc positives patients, monitored according to their viral load,
HBeAg/anti-HBe profile and alanine aminotransferase (ALT) level. Seventeen asymptomatic
carriers and sixteen chronic hepatitis B were analyzed. The genotypes identified were: A (84.4%),
C (9.4%), D (3.1%) and F (3.1%). In the genotype A, precore mutation was detected in 3.8%
(1/26) and BCP in 52.4% (11/21). In genotype C, only the BCP mutation was identified in 33.3%
(1/3) and no mutations were identified in genotypes D and F. This study provided the first
identification of the these mutations in genotype A in the State of Alagoas, Brazil. BCP mutations
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
75
were found equally in asymptomatic carriers and patients with chronic hepatitis B, independently
the viral load and serum ALT level. The results from this study contribute towards expanding the
information on genotype A, and serve as a reference point for new investigations.
Key words: Precore mutation, basal core promoter mutation, hepatitis B virus.
INTRODUCTION
The genetic variation in the hepatitis B virus (HBV) is partially due to the lack of a
revision mechanism involving DNA polymerase activity during the process of reverse
transcription of pre-genomic RNA. This favors the appearance of specific mutations, deletions or
insertions1. Natural variants of the pre-S/S, pre-C/C and P regions are found, and these result a
virus population with heterogeneous genomes known as quasispecies2.
The transition from G to A in the nucleotide (nt) 1896 creates a premature stop codon in
the precore region that prevents synthesis of the HBV e antigen (HBeAg), thereby reducing virus
replication3. On the other hand, the presence of thymine in nt 1858, forming a base pair (A-T)
with the adenine in nt 1896, makes the encapsidation signal of the pre-genomic RNA stronger.
This increases the efficiency of the replication, despite the presence of anti-HBe. The genotypes
B, C, D and E have thymine in nt 1858, F has cytosine or thymine and A generally has cytosine.
This explains the greater frequency of this mutation in the genotypes B, C, D, E and F4.
Mutations in the basal core promoter (BCP) region (A1762T and G1764A) have been
described independently of seroconversion of HBeAg5,6 and are common in different genotypes7,8.
Occurrences of these mutations alone or accompanied by the precore mutation G1896A have been
associated with active chronic hepatitis B, in HBeAg-negative/anti-HBe-positive infections5.
The aim of the present study was to investigate the genotypes and the presence of precore
mutation G1896A and BCP mutations A1762T/G1764A among patients with chronic HBV
infection at viral hepatitis referral centers in the State of Alagoas, Brazil, characterizing these
cases in terms of the viral load, HBeAg/anti-HBe profile and serum alanine aminotransferase
(ALT) level.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
76
PATIENTS AND METHODS
Patients
Between September 2006 and October 2007, 33 patients at viral hepatitis referral centers
in the State of Alagoas (20 men and 13 women) who were serologically positive for HBsAg and
anti-HBc were selected. There were 17 asymptomatic carriers and 16 with histologically
confirmed chronic hepatitis B.
The patients signed a consent statement and filled out a questionnaire to provide
demographic data. Blood was then collected by means of venous puncture, without anticoagulant.
Alanine aminotransferase assay
A commercial kit (Abbott Laboratories, Brazil) was used in accordance with the
manufacturer’s instructions. Assays were considered normal (N) when the concentration of ALT
was less than 1.5 times the normal upper limit (55 U/l) and high (H) when it was greater than or
equal to 1.5 times the normal upper limit9.
Serological markers
The HBeAg/anti-HBe markers were investigated by means of an immunoenzymatic assay
(Symbiosis Diagnóstica Ltda, São Paulo, Brazil).
Extraction and amplification of the S gene and precore region
Extraction of HBV-DNA and nested PCR of the S gene and precore region were
performed in accordance with the protocol described by Kaneko et al. (1989)11. The viral DNA
was extracted by treating the serum with guanidine isothiocyanate and phenol (GT) (Brasol, LGC
Biotecnologia), precipitated with cold absolute ethanol and resuspended in water-free RNAs and
DNAS (PCR water, Ludwig Biotec). The HBsAg gene was amplified using external primers
(Operon, Cologne, Germany) FHBS1, (5’GAGTCTAGACTCGTGGTGGACTTC–3’, nt 244-267) and
RHBS1(5’AAATKGCACTAGTAAACT3’,
(5’CGTGGTGGACTTCTCTCAATTTTC3’,
nt
668-691)
and
nt
255-278)
(5’GCCARGAGAAACGGRCTGAGGCCC3’, nt 648-671),
internal
primers
and
FHBS2
RHBS2
as described by Sitnik et al. (2004). For the
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
77
precore region, HBV-DNA-positive samples were amplified by using the external primers EP1.1
(5'TCATGGAGACCACCGTGAAG3 'nt 1606-1625)
and
internal
primers
EP2.1
and EP1.2 (5'GGAAAGAAGCAGAGGCAA3' nt 1955-1972)
(5'CATAAGAGGCTCTGGACT3
(5'GGCAAAAAAGAGAGTAACTC3', nt 1940-1959),
',
nt
1653-1670)
and
EP2.2
as described by Takahashi et al. (1995)10. A 10 µL
sample of viral DNA extracted was amplified in a 100 µL reaction volume containing 10mM Taq
DNA polymerase buffer, 50mM KCl, 1.5mM MgCl2, 150µM each of the four dNTP, 20 pmol/µL
of each of the primer and 2.5 U Taq DNA polymerase. The reaction for the two rounds of the
nested PCR was performed in a programmable thermocycler PTC 100, under the following
conditions: initial denaturation at 94°C, 20s followed by 30 cycles at 94°C, 20s; 56°C, 20s; 72 ºC,
30s and a final extension step at 72 ° C , 7 min. For the precore region: 94 º C, 30s and 30 cycles
at 94 ° C, 30s; 56oC, 30s; 72 º C, 40s with a final elongation at 72 ° C, 5 min.
Viral load - Titration of the HBV DNA
To estimate the viral load, serum samples pure and diluted, were incubated at 37oC for 1 h in the
presence of 2,5 µL NaOH 0.5 M followed directly of core region amplification by nested PCR as
described by Kaneko et al.11. Was added 2.5 µL of HCl 0.5 M and 85 µL of pre-mix containing
10mM Taq DNA polymerase buffer, 50mM KCl, 1.5mM MgCl2, 150µM each of the four dNTP,
20 pmol/µL of each of the primer and 2.5 U Taq DNA polymerase. Primers used were as follows:
external
1763F(5`GCTTTGGGGCATGGACATTGACCCGTATAA3`)
`CTGACTACTAATTCCCTGGATGCTGGGTCT3`)
and
internal
and
GACGAATTCCATTGACCCGTATAAAGAATT3`)
5`ATGGGATCCCTGGATGCTGGGTCTTCCAAA3`).
and
1778-F,
2032R(5
(5
`
2017R(
The amplification conditions for the two rounds
were as follows: 94 º C, 60s and 30 cycles at 94 ° C, 60s; 45oC, 60s; 72 º C, 90s with a final
elongation at 72 ° C, 7 min.
Viral load (copies / mL) was calculated by multiplying the title of the reaction with the
highest dilution of serum positive by PCR with detection limit of the method which corresponds
to 3 x 102 copies / mL as described by Anjos12.
Identification of genomic fragments
The amplified genomic fragments were fractionated by 2% agarose gel electrophoresis
stained with ethidium bromide and visualized under UV light.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
78
Sequencing reaction
The reamplification products were subjected to a linear PCR cycle using the primers FHBS2 and
RHBS2 for the HBsAg gene and EP2.1 and EP2.2 for the precore region For the direct sequencing
reaction (Sanger & Coulson 1975), commercially available reagents were used (DYEnamic
EDTye Terminator Cycle Sequencing kit, Buckinghamshire, England), adapted for the MegaBace
500 (GE Healthcare) automated sequencer.
Analysis of the sequences
Analysis of the genotypes was performed by comparing the sequences obtained with the
sequences of different HBV genotypes deposited in Genbank. The classification of the genotypes
was
confirmed
using
the
genotyping
tool
available
from
the
NCBI
website
(http://www.ncbi.nlm.nih.gov/projects/genotyping/formpage.cgi). Mutations were identified by
aligning the nucleotide sequences obtained from the study and making comparisons with a sequence
for the wild virus. For these analyses, the EditSeq and Megalign programs from the DNAstar
software package were used (Lasergene Inc., Madison, WI, USA).
RESULTS
Table 1 shows the demographic characteristics, HBeAg/anti-HBe profile, serum ALT
level, viral load, genotypes and mutations of the 17 asymptomatic carriers and 16 with chronic
hepatitis B.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
79
Table 1. Demographic data and characteristics of infections due to hepatitis B virus among asymptomatic
carriers and those with chronic hepatitis. Alagoas, Brazil, September 2006 to October 2007.
Patients
Age
ALT
HBeAg/
Viral load
Genotype
Mutation
BCP
Pre-core
(n = 33)
(Sex)
(U/l)
anti-HBe
(copies/mL)
Asymptomatic
43 (M)
E2
-/+
3 x 102
F
-
-
-/+
4
C
-
-
8
C
-
-
10
D
-
-
2
A
nd
-
carrier
(n = 17)
14 (M)
E
3
18 (F)
N
31 (F)
N
32 (F)
N
49 (F)
N
21 (M)
N
28 (F)
N
2
-/+
≤ 3 x 10
A
nd
-
+/-
4
A
nd
-
3 x 10
2
-/-
≤ 3 x 10
A
+
-
2
A
+
Nd1
A
+
-
A
+
-
A
+
-
3 x 10
31 (F)
N
-/+
≤ 3 x 102
E
N
N
41 (F)
N
27 (M)
N
31 (M)
E
-/+
-/+
3 x 10
4
3 x 10
8
2
-/+
≤ 3 x 10
A
-
-
-/+
3 x 10
2
A
-
-
3 x 10
4
A
-
Nd
4
A
-
-
8
A
-
-
-/+
-/+
3 x 10
32 (M)
N
-/+
3 x 10
36 (M)
E
+/-
3 x 102
A
+
-
+/-
3 x 10
4
A
+
-
3 x 10
6
A
+
-
10
A
+
-
10
A
+
-
6
A
+
-
8
A
-
-
12
A
-
-
A
-
+
54 (F)
N
29 (M)
N
38 (M)
E
31 (M)
N
33 (F)
N
30 (M)
E
24 (M)
E
14 (M)
N
38 (M)
N
32 (M)
N
30 (M)
N
28 (M)
E
46 (M)
N
46 (F)
N
47 (F)
1
3 x 10
-/+
41 (F)
(n = 16)
-/+
3 x 10
N
32 (M)
hepatitis
+/-
3 x 10
26 (M)
25 (F)
Chronic
-/+
3 x 10
2
N
3
nd = not determined; E = Elevated, N = Normal.
-/+
-/+
-/+
-/+
-/+
-/+
-/+
3x0
3x0
3 x 10
3 x 10
3x0
3 x 10
12
2
-/+
≤ 3 x 10
A
-
-
-/+
2
A
-
-
≤ 3 x 10
C
+
-
4
A
Nd
-
10
A
Nd
-
2
≤ 3 x10
A
Nd
-
2
nd
Nd
-
-/+
-/+
+/-/+
-/+
3 x 10
2
3 x 10
3 x 10
3 x 10
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
80
The genotypes were investigated in 32 sequences. Genotype A was identified in 84.4%
(27/32), C in 9.4% (3/32), D in 3.1% (1/32) and F in 3.1% (1/32) (Figure 1). The presence of
thymine at position 1858 was identified in 50% (13/26) of the sequences of genotype A and in
33.3% (1/3) of the sequences of genotype C. Thymine was absent from the genotypes D and F.
3.1%
3.1%
9.4%
A (n=27)
C (n=3)
D (n=1)
F (n=1)
84.4%
Figure 1 Genotypes identified in Alagoas, Brazil. September 2006 to October 2007.
The precore mutation G1896A was investigated in 31 sequences and was identified in one
patient with chronic hepatitis B genotype A. This individual presented a viral load of 3x1012
copies/mL, normal serum ALT concentration and was HBeAg-negative and anti-HBe-positive.
The BCP mutations A1762T and G1764A were investigated in 26 sequences, of which 21 were
genotype A, three were C, one was D and one was F. These mutations were identified in 52.4%
(11/21) of the infections due to genotype A, 50% (5/10) of the asymptomatic carriers and 54.5%
(6/11) of the patients with chronic hepatitis B. They were identified in 33.3% (1/3) of the
infections due to genotype C.
DISCUSSION
The nucleotide polymorphism that occurs naturally over the course of HBV infectons is
responsible for the appearance of punctual mutations in the viral genome. The combinations of
these mutations may have a wide variety of clinical significance in infections caused by different
genotypes.
The precore mutations G1896A/C1899A and BCP mutations A1762T/G1764A are the
most frequent types and, for this reason, they have been intensively investigated4,6,10,13-20.
However, most of these studies have involved Asian patients with genotypes B and C of HBV
infections9,20. In Brazil, the literature on the genotypes A, D and F is still sparse, and the present
study is the first to describe mutations among patients with HBV infection in Alagoas, Brazil.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
81
The genotype A generally has cytosine (C) at position 1858, according to the studies by
De Castro et al.22 and Sitnik et al.7, which found cytosine in 100% and 90% of the isolates of this
genotype, respectively. However, in our study, cytosine was found to be present in 50% of the
isolates. This is close to the frequency of 68.4% found by Rezende et al.17.
Circulation of the precore mutation G1896A of genotype A is rare and shows a
relationship with the presence of cytosine in nt 1858
7,14,17,22
. In our study, we also found a low
frequency of this mutation, although thymine was found to be present in 50% of the sequences of
genotype A that were investigated.
Thymine forms a base pair with adenine at position 1896, thereby making the
encapsidation signal of pre-genomic RNA stronger and favoring virus replication14. The presence
of a precore mutation in one patient with high viral load can be explained in terms of replacement
of cytosine by thymine in nt 1858, although this substitution could not be identified.
The frequency of the BCP mutation A1762T/G1764A found in genotype A, was
concordant with the findings of Sitnik et al.7, i.e. a positive rate of 62% (31/50). However, this
rate differs from the results found by De Castro et al.22, who found a frequency of 20% (2/10).
This mutation was distributed equally among the asymptomatic carriers and those with chronic
hepatitis, independently the serum ALT level and viral load.
So the BCP mutation
A1762T/G1764A seemed doesn’t interfere with the clinical course of HBV infection.
However, in studies on other genotypes, BCP mutations have been correlated with greater
activity and frequency of chronic hepatitis B. They are considered to be one of the independent
predictive viral factors for the risk of developing hepatocellular carcinoma 6,19,20,22.
The identification of a single A1762T/G1764A mutation in genotype C in a patient of
non-Asian origin differed from the findings of Sitnik et al.7, who found this mutation in 76.9% of
the Asian patients. It is emphasized that most studies in Brazil did not detect this genotype 17,22-29,
it was only detected by Bottecchia et al.30 and Oliveira et al.31.
This study provides the first identification in Alagoas, Brazil, of the presence of the
precore mutation G1896A and the BCP mutations A1762T/G1764A in genotype A of HBV
infections. The frequency of cytosine at position 1858 did not present any relationship with the
low frequency of precore mutation in genotype A. BCP mutations were detected equally among
asymptomatic carriers and those with chronic hepatitis, despite the viral load and serum ALT
levels. The results from this study contribute towards expanding the information on genotype A
and serve as a reference point for new investigations.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
82
The authors’ contributions
(1) Contributed substantially towards the conception and planning, (2) Contributed towards the
data analysis and interpretation (3) Contributed significantly towards preparing the draft and
critically reviewing the content; and (4) Participated in preparing the final manuscript.
(1) Alba M.X. Eloy, Regina C. Moreira, Maria R.C.D. Coêlho.
(2) Alba M.X. Eloy, Regina C. Moreira, Marcílo L. Figueiredo, Maria R.C.D. Coêlho.
(3) Alba M.X. Eloy, Regina C. Moreira, Marcílo L. Figueiredo, Jéfferson L.A. Silva, Maria
R.C.D. Coêlho.
(4) Alba M.X. Eloy, Regina C. Moreira, Marcílo L. Figueiredo, Jéfferson L.A. Silva, Maria
R.C.D. Coêlho.
Ethical approval
This research project using human beings was approved by the Research Ethics Committee of the
Federal University of Alagoas (UFAL), under research protocol No. 000906/2005-98.
Acknowlegments
Biotechnology Laboratory of the Center for Agricultural Sciences / Federal
University of
Alagoas, Division of Molecular Biology of the Laboratory of Immunopathology Keizo / Federal
University of Pernambuco and Laboratory of Viral Hepatitis of the Institute Adolfo Lutz
Funding: FAPEAL through the award of a PhD fellow.
Conflicts of interest: none declared
REFERENCES
1.Summers J, Mason WS. Replication of the genome of a hepatitis B-like virus by reverse
transcription of an RNA intermediate. Cell 1982, 29: 403-15.
2.Ballard Al, Boxall EH. Colourimetric point mutation assay: for detection of precore mutants of
hepatitis B. J Virol Methods 1997, 67: 143-52.
3.Carman WF et al. Mutation preventing formation of hepatitis B virus (HBV) e antigen in
patients with chronic hepatitis B infection. Lancet 1989, 9 (8663): 588-91.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
83
4.Yotsuyanagi H, Hino K, Tomita E, Toyoda J, Yasuda K, Iino S. Precore and core promoter
mutations, hepatitis B virus DNA levels and progressive liver injury in chronic hepatitis B. J
Hepatol 2002, 37: 355-63.
5.Okamoto H et al. Hepatitis B virus with mutations in the core promoter for an e antigennegative phenotype in carriers with antibody to e antigen. J Virol 1994, 68 (12): 8102-10.
6.Bozdayi AM et al. Nucleotide divergences in the core promoter and precore region of genotype
D hepatitis virus in patients with persistently elevated or normal ALT levels. J Clin Virol 2001,
21: 91-101.
7.Sitnik R, Pinho JRR, Bertolini DA, Bernardini AP, Silva LC, Carrilho FJ. Hepatitis B virus
genotypes and precore and core mutants in brasilian patients. J Clin Microbiol 2004, 42: 6, 2455460.
8.Candotti D, Opare-Sem O, Rezvan H, Sarkodie F, Allain JP. Molecular and serological
characterization of hepatitis B virus in deferred Ghanaian blood donors with and without elevated
alanine aminotransferase. J Viral Hepat 2006, 13 (11):715-24.
9.Lai CL, Ratziu V, Yuen M-F, Polynard T. Viral hepatitis B. Lancet 2003, 362: 2089-94.
10.Takahashi K et al. The precore/core promoter mutant (T1762A1764) of hepatitis B virus: clinical
significance and an easy method for detection. J Gen Virol 1995, 76: 3159-164.
11.Kaneko S, Feinstone SM, Miller RH. Rapid and sensitive method for the detection of serum
hepatitis B virus DNA using the polymerase chain reaction technique. J Clin Microbiol 1989, 27
(9): 1930-33.
12. Anjos LC. Marcadores de replicação do vírus da hepatite B: comparação de métodos de
biologia molecular, de sorologia e imunohistoquímuca. São Paulo, 1999. (Dissertação de
Mestrado – Facultade de Medicina da Universidade de São Paulo).
13.Sanger F, Coulson AR. A rapid method for determining sequences in DNA by primed
synthesis with DNA polymerase. J Mol Biol 1975, 94: 441-48.
14.Li JS, Tong SP, Wen YM, Vitvitski L, Zhang Q Trepo C. Hepatitis B virus genotype A rarely
circulates as an HBe-minus mutant: possible contribution of a single nucleotide in the precore
region. J Virol 1993, 67(9): 5402-410.
15.López JL et al. Deteccion y caracterizacion de mutantes pre-core del virus de la hepatitis B
(HBV) en pacientes cronicamente infectados. Acta Gastroenter Latinoamer 1995, 25: 85-90.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
84
16.Yuen MF et al. Epidemiological study of hepatitis B virus genotypes, core promoter and
precore mutations of chronic hepatitis B infection in Hong Kong. J Hepatol 2004, 41: 119-25.
17.Rezende REF et al. The precore mutation is associated with severity of liver damage in
Brazilian patients with chronic hepatitis B. J Clin Virol 2005, 32: 53-59.
18.Tong S. Mechanism of HBV genome variability and replication of HBV mutants. J Clin Virol
2005, 34: 134-38.
19.Tong MJ, Blatt LW, Kao J-H, Cheng JT, Corey GW. Basal core promoter T1762/A1764 and
precore A1896 gene mutations in hepatitis B surface antigen-positive hepatocellular carcinoma: a
comparison with chronic carriers. Liver Int 2007, 1356-363.
20.Chou YC et al. Temporal relationship between hepatitis B virus enhancer II/basal core
promoter sequence variation and risk of hepatocellular carcinoma. Gut 2008, 57:91–97.
21.Schaefer S. Hepatitis B virus: significance of genotypes. J Viral Hepat 2005, 12: 111-14.
22.De Castro L, Niel C, Gomes SA. Low frequency of mutations in the core promoter and precore
regions of hepatitis B virus in anti-HBe positive Brazilian carriers. BMC Microbiol 2001, 1:10.
23.Teles AS et al. Hepatitis B virus transmission in Brazilian hemodialysis units: Serological and
molecular follow-up. J Med Virol 2002, 68: 41-49.
24.Araujo NM, Mello FCA, Yoshida CFT, Niel C, Gomes SA. High proportion of subgroup A’
(genotype A) among Brazilian isolates of hepatitis B virus. Arch Virol 2004, 149:1383-95.
25.Carrilho FJ et al. Hepatitis B virus infection in Haemodilysis Centres from Santa Catarina
State, Southern Brazil. Predictive risk factors for infection and molecular epidemiology. BMC
Public Health 2004, 4:13.
26.Motta-Castro ARC et al. Hepatitis B virus infection in isolated Afro-Brazilian communities. J
Med Virol 2005, 77(2): 188-93.
27.Ribeiro NRC et al. Distribution of hepatitis B virus genotypes among patients with chronic
infection. Liver Int 2006, 26: 636-42.
28.Mello FCA et al. Hepatitis B virus circulating in Brazil: Molecular characterization of
genotype F isolates. BMC Microbiol 2007, 7:103.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
85
29.Gomes-Gouvêa MS et al. Hepatitis D e B virus genotypes in chronically infected patients from
the Eastern Amazon Basin. Acta Trop 2008, 106 (3): 149-55.
30.Bottecchia M et al. Hepatitis B virus genotypes and resistance mutations in patients under long
term lamivudine therapy: characterization of genotype G in Brazil. BMC Microbiol 2008, 8: (11).
31.Oliveira CM, Farias IP, Fonseca JCF, Brasil, LM, Souza R, Astolfi-Filho S. Phylogeny and
molecular genetic parameters of different stages of hepatitis B virus infection in patients from the
Brazilian Amazon. Arch Virol 2008, 153: 823-
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
86
9.0 CONCLUSÕES
O fragmento da região S do DNA-HBV foi detectado com maior freqüência em pacientes com
hepatite crônica e na maioria dos portadores assintomáticos a carga viral foi baixa.
O genótipo A foi predominante, seguido dos genótipos C, D e F.
Independente do genótipo apresentado, a maioria das infecções foi identificada com
soroconversão do HBeAg e nível sérico normal de ALT.
Houve baixa freqüência da mutação pré-core (G1896A) no genótipo A, não sendo detectada nos
demais genótipos.
Houve alta freqüência das mutações BCP (A1762T/G1764A) no genótipo A e baixa no tipo C,
não sendo identificadas nos demais genótipos.
No genótipo A, as mutações BCP foram detectadas equitativamente nos portadores assintomáticos
e com hepatite crônica, a despeito da carga viral e nível sérico de ALT.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
87
10.0 RECOMENDAÇÕES
O polimorfismo nucleotídico do HBV, resultando quasispecies virais ao longo do curso da
infecção demonstra a necessidade de se conhecer as características genéticas do genoma viral.
Portanto, de acordo com os resultados da pesquisa, recomendamos o diagnóstico molecular da
infecção pelo VHB, visando:
¾ Identificar genótipos para investigação epidemiológica e avaliação do curso clínico da
infecção.
¾ Investigar mutações nas regiões pré-core e BCP para avaliação da atividade viral e
expressão do HBeAg.
¾ Quantificar a carga viral, para indicação de terapia anti-viral.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
88
REFERÊNCIAS
AHN, J.Y. et al. Transcriptional repression of p21waf1 promoter by hepatitis B virus x proteinvia a
p53-independent pathway. Gene, v. 275, p. 163-168, 2001.
ANJOS, L.C. et al. Hepatitis B virus replication markers: comparison of molecular biological
serological and immunohistochemical methods. In 101 st Annual Meeting of the American
Gastroenterological Association, San Diego, 2000.
ARAUJO, N.M. et al. High proportion of subgroup A’ (genotype A) among Brazilian isolates of
hepatitis B virus. Archives of Virology, v.149, p.1383-1395, 2004.
ARAÚJO, E.S.A.; BARONE, A.A. Terapia da hepatite B crônica: como e quando? Pacientes
virgens de terapia. The Brasilian Journal of Infectius Diseases, v. 10, p. 53-56, 2006.
Supplement 1-Aug.
ARAUZ-RUIZ, P. et al. Genotype H: a new Ameridian genotype of hepatitis B virus revealed in
Central America. Journal of General Virology, v. 83, p. 2059-2073, 2002.
ARRAES, L.C. et al. The biological meaning of anti-HBc positive result in blood donors: relation
to HBV-DNA and to other serological markers. Revista do Instituto de Medicina Tropical de
São Paulo, v. 45, n. 3, p. 137-140, May-June, 2003.
BALLARD, A.L.; BOXALL E.H. Colourimetric point mutation assay: for detection of precore
mutants of hepatitis B. Journal of Virological Methods, v. 67, p. 143-152, 1997.
BANCROFT, W.H.; MUNDON F.K.; RUSSELL P.K. Detection of additional antigenic
determinants of hepatitis B antigen. The Journal of Immunology, 109: 842-848, 1972.
BERTOLINI, D.A. et al. Hepatitis B virus genotype H in Paraná State, Southern Brazil. [abstract].
In Virus: Reviews and Research, São Lourenço-MG: SBV; v. 9, 2004, p. 144.Supplement 1.
BOTTECCHIA, M. et al. Hepatitis B virus genotypes and resistance mutations in patients under
long term lamivudine therapy: characterization of genotype G in Brazil. BMC Microbiology, v.
8, p. 11, 2008.
BOAG, F. Hepatitis B: heterosexual transmission and vaccination strategies. International
Journal of STD & AIDS, v. 2, p. 318-324, 1991.
ZAIDAN, A.M. E.
89
Caracterização genética do vírus da hepatite B...
BOZDAYI, A.M. et al. Nucleotide divergences in the core promoter and precore region of
genotype D hepatitis B virus in patients with persistently elevated or normal ALT levels. Journal
of Clinical Virology, v. 21, p. 91-101, 2001.
BRUNETO, M.R. et al. A new hepatitis B virus strain in patients with severe anti-HBe positive
chronic hepatitis B. Journal of Hepatology, v. 10, p. 258-261, 1990.
CANDOTTI, D. et al. Molecular and serological characterization of hepatitis B virus in deferred
Ghanaian blood donors with and without elevated alanine aminotransferase. Journal of Viral
Hepatology, v. 13, n. 11, p. 715-724, 2006.
CARRILHO, F.J. et al. Hepatitis B virus infection in haemodialysis Centres from Santa Catarina
State, Southern Brazil. Predictive risk factors for infection and molecular epidemiology. BMC
Public Health, v. 4, p. 13, 2004.
CHANG, S-F. et al. Characterization of nonconventional hepatitis B viruses lacking the core
promoter. Virology, v. 330, n. 2, p. 437-446, 2004.
CHAUHAN, R. et al. Basal core promoter, precore region mutations of HBV and their association
with e antigen, genotype, and severity of liver disease in patients with chronic hepatitis B in India.
Journal of Medical Virology, v. 78, n. 8, p. 1047-1054, 2006.
CHOU, Y.C. et al. Temporal relationship between hepatitis B virus enhancer II/basal core
promoter sequence variation and risk of hepatocellular carcinoma. Gut, v. 57, p.91-97, 2008.
CHU, C.J.; HUSSAIN, M.; LOK, A.S.F. Hepatitis B virus genotype B is associated with earlier
HBeAg seroconversion compared with hepatitis B virus genotype C. Gastroenterology, v. 122, p.
1756-1762, 2002.
CLARKE, B.; BLOOR, S.. Molecular genotyping of hepatitis B virus. Journal of Clinical
Virology, v. 25, p. S41-S45, 2002.
COLLIER, L; OXFORD, J. Introduction to the hepatitis viruses. In:______ Human Virology. 2th
ed. New York: Oxford University, 2000, p.153-154.
COUROUCÉ-PAUTY, A.M.; LEMAIRE, J.M.; ROUX, J.F. New hepatitis B surface antigen subt
rum hepatitis B virus DNA using the polymerase chain reaction technique. Journal of Clinical
Microbiology, v. 27, n. 9, p. 1930-1933, Sept. 1989.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
90
DA SILVA, L.C. et al. Efficacy and tolerability of long-term therapy using high lamivudine doses
for the treatment of chronic hepatitis B. Journal of Gastroenterology, v. 36, p. 476-485, 2001.
D EVESA, M. et al. Clade analysis and surface antigen polymorphism of hepatitis B virus
American genotypes. Journal of Medical Virology, v. 72, n. 3, p. 377-384, 2004.
GANEM, D. Hepadnaviridae and their replication. In: FIELDS, B.N. et al. Fundamental Virology.
3th ed. Philadelphia: Raven, 1996, p.1199-1233.
HOLLINGER, F.B. Hepatitis B virus. In: FIELDS, B.N. et al. Fields Virology. 3th ed. P
hiladelphia: Raven, 1996, p. 2739-2807.
HONDA, A. et al. Detection of mutations in the enhancer 2/core promoter region of hepatitis B
virus in patients with chronic hepatitis B virus infection: Comparison with mutations in precore
and core regions in relation to clinical status. Journal of Medical Virology, v. 57, n. 4, p. 337-344,
1999.
HOU, J. et al. Prevalence of naturally occurring surface gene variants of hepatitis B virus in
nonimmunized surface antigen-negative Chinese carriers. Hepatology,v. 34, n. 5, p. 1027-1034,
2001.
JAMMEH, S. et al. Effect of basal core promoter and pre-core mutations on hepatitis B virus
replication. Journal of General Virology, v. 89, p. 901-909, 2008.
KANEKO, S.; FEINSTONE, S.M.; MILLER, R.H. Rapid and sensitive method for the detection
of serum hepatitis virus DNA using the polymerase chain reaction technique. Journal of Clinical
Microbiology, v. 27, n. 9, p. 1930-1933, Sept. 1989.
KAO, J.H. et al. Hepatitis B genotypes and response to interferon therapy. Journal of
Hepatology, v. 33, p. 998-1002, 2000.
KATO, H. et al. Hepatitis B e antigen in sera from individuals infected with hepatitis B virus of
genotype G. Hepatology, v. 35, n. 4, p. 922-929, 2002.
KHOURI, M.E. et al. Seroprevalence of hepatitis B virus and hepatitis C virus in Monte Negro in
the Brazilian western Amazon region. Clinics, v. 60, n. 1, p. 29-36, 2005.
KIDD-LJUNGGREN, K.; MIYAKAWA, Y.; KIDD, A.H. Genetic variability in hepatitis B
viruses. Journal of General Virology, v. 83, p. 1267-1280, 2002.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
91
KONG, H.J. et al. Direct binding of hepatitis B virus X protein and retinoid X receptor contributes
to phosphoenolpyruvate carboxykinase gene transactivation. FEBS Letters, v. 483, p. 114-118,
2000.
KUMAR, A. et al. Hepatitis B virus genotype A is more often associated with severe liver disease
in northern India than is genotype D. Indian Journal of Gastroenterology, v. 24, n. 1, p. 19-22,
2005.
LAI, C.L. et al. Viral hepatitis B. Lancet, v. 362, p. 2089-2094, 2003.
LEUNG, N.W.Y. et al. Extended lamividine treatment in patients with chronic hepatitis B
enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology,
v. 33, n. 6, p. 1527-1532, 2001.
LI, J.S. et al. Hepatitis B virus genotype A rarely circulates as an HBe-minus mutant: possible
contribution of a single nucleotide in the precore region. Journal of Virology, v. 67, n. 9, p.
5402-5410, 1993.
LI, K.S. et al. Hepatitis B virus harboring nucleotide deletions in the core promoter region and
genotype B correlate with low viral replication activity in anti-HBe positive carriers. Journal of
Clinical Virology, v. 23, p. 96-106, 2001.
LUSIDA, M.I. et al. Genotype and subtype analyses of hepatitis B virus (HBV) and possible coinfection of HBV and hepatitis C virus (HCV) or hepatitis D virus (HDV) in blood donors,
patients with chronic liver disease and patients on hemodialysis in Surabaya, Indonesia.
Microbiology and Immunology, v. 47, n. 12, p. 969-975, 2003.
LYRA, A.C. et al. Distribution of hepatitis B virus (HBV) genotypes among patients with acute
viral hepatitis. Journal of Clinical Gastroenterology, v. 39, n. 1, p. 81, 2005.
MACHADO; ZURAVSKI. Soroprevalência em doadores de sangue do Hospital universitário de
Santa Maria/RS no ano de 2005. NewsLab, ed. 80, p. 108-112, 2007
MAGNIUS, L.O.; ESPMARK, L.Å. New specificities in Australia antigen positive sera distinct
from the Le Bouvier determinants. The Journal of Immunology, v. 109, p. 1017-1021, 1972.
MCMAHON, B.J.; ALBERTS, S.R.; WAINWRIGHT, R.B. Hepatitis B related sequelae:
prospective study in 1400 hepatitis B surface antigen-positive Alaska native carriers. Archives of
Internal Medicine, v. 150, p. 1051-1054, 1990.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
92
MAHONEY, F.J. Update on Diagnosis, management, and prevention of hepatitis B virus
infection. Clinical Microbiology Reviews, v. 12, n. 2, p. 315-366, 1999.
MENDONÇA, J.S.; VIGANI, A.G. História natural da hepatite B aguda e crônica. The Brazilian
Journal of Infectious Diseases, v. 10, p. 15-18, 2006, Suplement 1-Aug.
MELLO, F.C.A. et al. Hepatitis B virus genotypes circulating in Brazil: molecular
characterization of genotype F isolates. BMC Microbiology, v. 7, p. 103, 2007.
MIRANDA et al. Marcadores sorológicos de hepatite B em indivíduos submetidos a exames de
sngue em unidades de saúde. Rev Saúde Pública, v. 34, n. 3, p. 286-291, 2000.
MIYAMOTO; BERTOLINI. Estudo da soroprevalência do AgHBs em gestantes da 15a Regional
de Saúde e da imunoproxilaxia para os recém-nascidos das gestantes AgHBs positivo. Acta Sci.
Health Sci, v. 30, n. 1, p. 1-6, 2008.
MORAES, M.T.; GOMES, S.A.; NIEL, C. Sequence analysis of pre-S/S gene of hepatitis B virus
strains of genotypes A, D, and F isolated in Brazil. Archives of Virology, v. 141, n. 9, p. 17671773, 1996.
MINISTÉRIO DA SAÚDE 2001. Manual de normas de vacinação. Disponível em:
<http://portal.saude.gov.br/portal/arquivos/pdf/manu_normas_vac1.pdf>.
Acesso
em:
28mar.2009.
MOTTA-CASTRO, A.R.C. et al. Hepatitis B virus infection in isolated Afro-Brasilian
communites. Journal of Medical Virology, v. 77, n. 2, p. 188-193, 2005.
MURRAY; ROSENTHAL; PFALLER. Vírus da Hepatite. In: _______. Microbiologia Médica.5
ed. Rio de Janeiro: Elsevier, 2006, p. 659-673.
NORDER, H. et al. Comparison of the amino acid sequences of nine different serotypes of
hepatitis B surface antigen and genomic classification of the corresponding hepatitis B virus
strains. Journal of general Virology, v. 73, p. 1201-1208, 1992.
NORDER, H.; COUROUCÉ, A-M.; MAGNIUS, L.O. Complete genomes, phylogenetic
relatedness, and structural proteins of six strains of the hepatitis B virus, four of which represent
two new genotypes. Virology, v. 198, p. 489-503, 1994.
NORDER, H. et al. Complete sequencing of a gibbon hepatitis B virus genome reveals a unique
genotype distantly related to the chimpanzee hepatitis B virus. Virology, v. 218, p. 214-223,
1996.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
93
OKAMOTO, H. et al. Typing Hepatitis B virus by homology in nucleotide sequence: comparison
of surface antigen subtypes. Journal of General Virology, v. 69, p. 2575-2583, 1988.
OKAMOTO, H. et al. Hepatitis B viruses with pre-core region defects prevail in persistently
infected hosts along with seroconversion to the antibody against e antigen. Journal of Virology,
v. 64, n. 3, p. 1298-1303, Mar. 1990.
OKAMOTO, H. et al. Hepatitis B virus with mutations in the core promoter for an e antigennegative phenotype in carriers with antibody to e antigen. Journal of Virology, v. 68, n.12, p.
8102-8110, Dec. 1994.
OLIVEIRA, C.M. et al. Phylogeny and molecular genetic parameters of different stages of
hepatitis B virus infection in patients from the Brazilian Amazon. Archives of Virology, v. 153,
p. 823-830, 2008.
OLYAEE, S.A.B. et al. Complete genomic sequence and phylogenetic relatedness of hepatitis B
virus isolates from Iran. Journal of Medical Virology, v. 76, n. 3, p. 318-326, 2005.
PARANÁ, R.; ALMEIDA, D. HBV epidemiology in Latin America. Journal of Clinical
Virology, v. 34, n. 1, p. S130-S133, 2005.
REZENDE, R.E.F. et al. The precore mutation is associated with severity of liver damage in
Brazilian patients with chronic hepatitis B. Journal of Clinical Virology, v. 32, p. 53-59, 2005.
RIBEIRO, N.R.C. et al. Distribution of hepatitis B virus genotypes among patients with chronic
infection. Liver International, v. 26, p. 636-642, 2006.
SÁNCHEZ, L.V. et al. Genotypes and S-gene variability of Mexican hepatitis B virus strains.
Journal of Medical Virology, v. 68, n. 1, p. 24-32, 2002.
SANCHEZ-TAPIAS, J.M. et al. Influence of hepatitis B virus genotype on the long-term outcome
of chronic hepatitis B in Western patients. Gastroenterology, v. 123, n. 6, p. 1848-1856, 2002.
SANGER, F.; COULSON, A.R. A rapid method for determining sequences in DNA by primed
synthesis with DNA polymerase. Journal of Molecular Biology, v. 94, p. 441-448, 1975.
SATO, S. et al. Hepatitis B virus strains with mutations in the core promoter in patients with
fulminant hepatitis. Annals of Internal Medicine, v. 122, n. 4, p. 241-248, 1995.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
94
SCHAEFER, S. Hepatitis B virus: significance of genotypes. Journal of Viral Hepatitis, v. 12,
p. 111-124, 2005.
SITNIK, R. et al. Hepatitis B virus genotypes and precore and core mutants in brasilian patients.
Journal of Clinical Microbiology, v. 42, n. 6, p. 2455-2460, 2004.
SITNIK, R. et al. Hepatitis B virus genotype E detected in Brazil in an african patient who is a
frequent traveler. Brazilian Journal of Medical and Biological Research, v. 40, n. 12, p. 16891692, Dec. 2007.
SOMMER, G.; VAN BÖMMEL, F.; WILL, H. Genotype-specific synthesis and secretion of
spliced hepatitis B virus genomes in hepatoma cells. Virology, v. 271,
p. 371-381, 2000.
STUYVER, L. et al. A new genotype of hepatitis B virus: complete genome and phylogenetic
relatedness. Journal of General Virology, v. 81, p. 67-74, 2000a.
STUYVER, L. et al. Line probe assay for monitoring drug resistance in hepatitis B virus-infected
patients during antiviral therapy. Journal of Clinical Microbiology, v. 38, 2, p. 702-707, Feb.
2000b.
SUMMERS, J.; MASON W.S. Replication of the genome of a hepatitis B-like virus by reverse
transcription of an RNA intermediate. Cell, v. 29, p. 403-415, 1982.
TAKAHASHI, K. et al. The precore/core promoter mutant (T1762A1764) of hepatitis B virus:
clinical significance and an easy method for detection. Journal of General Virology, v.76, p.
3159-3164, 1995.
TAVARES-NETO et al. Seroprevalence of hepatitis B and C in the Western Brazilian Amazon
Region (Rio Branco, Acre): a pilot study carried out during a hepatitis B vaccination program.
The Brazilian Journal of Infectious Diseases, v. 8, n. 2, p. 133-139, 2004.
THAKUR, V. et al. Profile, spectrum and significance of HBV genotypes in chronic liver disease
patients in the Indian subcontinent. Journal of Gastroenterology and Hepatology, v. 17, n. 2, p.
113-115, Feb. 2002.
TENGAN, F.M. ARAÚJO, E.S.A.2006. Epidemiologia da hepatite B e D e seu impacto no
sistema de saúde. The Brasilian Journal of Infectious Diseases, v. 10, p. 6-10, 2006.
Supplement 1-Aug.
ZAIDAN, A.M. E.
95
Caracterização genética do vírus da hepatite B...
TELES, S.A. et al. Hepatitis B virus transmission in Brazilian hemodialysis units: serological and
molecular follow-up. Journal of Medical Virology, v. 68, n. 1, p. 41-49, 2002.
TIOLLAIS, P.; POURCEL, C.; DEJEAN, A. The hepatitis B virus. Nature v. 317,
p. 489-495, Oct. 1985.
TONG, S. Mechanism of HBV genome variability and replication of HBV mutants. Journal of
Clinical Virology, v. 34, n. 1, p. S134-S138, 2005.
TONG M.J. et al. Basal core promoter T1762/A1764 and precore A1896 gene mutations in
hepatitis B surface antigen-positive hepatocellular carcinoma: a comparison with chronic carriers.
Liver International, 1356-363, 2007.
TURNER, P.C. et al. Clonagem do DNA: uma visão geral. In: ______. Biologia Molecular. 2 ed.
Rio de Janeiro: Guanabara Koogan, 2004, p. 89-91.
VIANA, S. et al. High prevalence of hepatitis B virus and hepatitis D virus in the western
brasilian amazon. American Journal of Tropical Medicine and Hygiene, v.73, n. 4, p. 808814, 2005.
WORLD
HEALT
ORGANIZATION.
Hepatitis
<http://www.who.int.emc>. Acesso em: 20 dez.2004.
B
2002.
Disponível
WORLD
HEALT
ORGANIZATION.
Hepatitis
B.
Disponível
<http://www.who.int/mediacentre/factsheets/fs204/en/>Acesso em: 05 maio2009.
em:
em:
WONG, D.T.; NATH, N.; SNINSKY, J.J. Identification of hepatitis B virus polypeptides encoded
by the entire pre-S open reading frame. Journal of Virology, v. 55, n. 1, p. 223-231, 1985.
YEN, T.S.B. Regulation of hepatitis B virus gene expression. Virology, v. 4, p.33-42, 1993.
YOTSUYANAGI, H. et al. Precore and core promoter mutations, hepatitis B virus DNA levels
and progressive liver injury in chronic hepatitis B. Journal of Hepatology, v. 37, p. 355-363,
2002.
YUEN, M.F. et al. Epidemiological study of hepatitis B virus genotypes, core promoter and
precore mutations of chronic hepatitis B infection in Hong Kong. Journal of Hepatology, v. 41,
p. 119-125, 2004.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
96
ZHANG, P.; McLACHLAN, A. Differentiation-specific transcriptional regulation of the hepatitis
B virus nucleocapsid gene in human hepatoma cell lines. Virology, v. 202, p. 430-440, 1994.
ZHENG, X. et al. Characterization of complex B cell epitopes on woodchuck hepatitis virus
surface antigens by using plasmids encoding chimeric proteins and DNA immunization.
Virology, v. 294, n. 2, p. 342-353, Mar. 2002.
ZHENG, X. et al. Mutant hepatitis B virus surface antigens (HBsAg) are immunogenic but may
have a changed specifity. Virology, v. 329, p. 454-464, 2004.ypes inside the ad category. Vox
Sanguinis, v. 35, n. 5, p. 304-308, 1978.
ZAIDAN, A.M. E.
APÊNDICES
Caracterização genética do vírus da hepatite B...
97
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
98
Apêndice A
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
Eu,..................................................................................., tendo sido convidad(o,a) a participar
como voluntári(o,a) do estudo Caracterização Genética do Vírus da Hepatite B em Alagoas,
recebi da profa. Alba Maria Eloy Zaidan, Farmacêutica Bioquímica do Laboratório de Análises
Clínicas do Hospital Universitário e professora Assistente do Departamento de Patologia do
Centro de Ciências |Biológicas da UFAL, responsável por sua execução as seguintes informações
que me fizeram entender sem dificuldades e sem dúvidas os seguintes aspectos:
1. Que o estudo se destina a detectar o DNA do vírus da Hepatite B e identificar o tipo de
genoma, pois já foram identificados 8 tipos diferentes de genoma deste vírus.
2. A importância deste estudo é detectar ao mesmo tempo a infecção viral e conhecer o genótipo
do vírus e assim contribuir para um diagnóstico laboratorial mais completo.
3 Com essas informações o médico vai poder acompanhar melhor a evolução da infecção e
também a resposta aos medicamentos específicos para o vírus.
4. Que esse estudo começará em agosto/2006 e terminará em dezembro/2008.
5.Que o estudo será feito da seguinte maneira: Será aproveitado o procedimento de coleta de
sangue dos pacientes que estiverem portando solicitação médica para pesquisa de HBsAg e ou
AntiHBc total.
6. Que eu participarei dando permissão para que o sangue coletado para os exames de rotina,
possa também ser utilizado no estudo, não sendo necessário que eu retorne ao laboratório para
outro procedimento de coleta de sangue.
7. Que os resultados serão encaminhados ao prontuário ou entregues pessoalmente pelo próprio
laboratório aos pacientes que não tiverem prontuário no hospital. Ou ainda pela professora Alba
Maria Eloy Zaidan pelo contato: Rua Barão José Miguel Nº 249/601, Farol. Telefones:
(082)30321495 / (082)99684084.
8. Que os benefícios que deverei esperar com a minha participação, mesmo que não diretamente
são: contribuir para a realização de um novo tipo de exame para completar o diagnóstico
laboratorial da infecção pelo vírus da hepatite B
9. Que as informações conseguidas através da minha participação não permitirão a identificação
da minha pessoa, exceto aos responsáveis pelo estudo, e que a divulgação das mencionadas
informações só será feita entre os profissionais estudiosos do assunto.
10. Finalmente, tendo eu compreendido perfeitamente tudo o que me foi informado sobre a minha
participação no mencionado estudo e estando consciente do meu direito, de conhecer o resultado
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
99
do exame e dos benefícios que a minha participação implicam, concordo em dele participar e
autorizo ser procurado para participar de outros projetos dentro dessa linha de pesquisa. Para isso
eu DOU O MEU CONSENTIMENTO SEM QUE PARA ISSO EU TENHA SIDO FORÇADO
OU OBRIGADO.
.............................................................................................................................................................
...
Assinatura do paciente ou responsável
Endereço d(o,a) participante-voluntári(o,a):
.............................................................................................................................................................
.............................................................................................................................................................
......
Data: __________/___________/___________
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
100
Apêndice B
QUESTIONÁRIO
CARACTERIZAÇÃO GENÉTICA DO VÍRUS DA HEPATITE B EM ALAGOAS
1. Nome do paciente
4. Unidade de Saúde
..........................................................................................
2. Mãe
1. HUAA
...........................................................................................
2. HEHA
3. Outras
3. Data da coleta ______ / _______ / __________
5. Nº do prontuário
____________________________
6. Onde mora atualmente?
Rua ________________________________________________________ Nº ______
Apto. _________ Bloco ___________
Bairro ______________________ Cidade ________________________
Estado ________ CEP _____________________
Telefone ________________________ Há quanto tempo? _____________________
7. Qual a sua idade?
9. Qual o local de nascimento?
________________ ANOS
.......................................................................
10. Qual a sua origem familiar?
8. Qual a data do seu nascimento?
______ / _______ / __________
1. Brasileiro
2. Outro. Especificar: ___________________
11. Sexo
12. Em que grupo de cor/raça se enquadra?
1. Branca
1. Masculino
2. Preta
2. Feminino
3. Amarela
4. Indígena
5. Parda
9. Não sabe informar
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
101
DADOS LABORATORIAIS
13. Marcadores sorológicos (atual)
1. Reagente
HBsAg
HBeAg
2. Não reagente
Anti-HBc Total
Anti-HBe
3. Inconclusivo
Anti-HBc IgM
Anti-HBe
4. Não realizado
14. Marcadores sorológicos (resultados anteriores)
1. Reagente
HBsAg
HBeAg
2. Não reagente
Anti-HBc Total
Anti-HBe
3. Inconclusivo
Anti-HBc IgM
Anti-HBe
4. Não realizado
15. Dosagem bioquímica (atual)
16. Dosagem bioquímica (resultados anteriores)
ALT (TGP) ____________ U/L
ALT (TGP) ____________ U/L
Data: ____________________
Ref. Até _____________ U/L
ALT (TGP) ____________ U/L
Data: ____________________
Ref. Até _____________ U/L
INFORMAÇÕES CLÍNICAS
17. Forma clínica da infecção pelo HBV
1. Infecção assintomática aguda
3. Hepatite crônica
2. Hepatite aguda
4. Portador assintomático
18. Tratamento
1. Lamivudina
1. Sim 2. Não
Há quanto tempo? ................................................
2.Interferon
1. Sim 2. Não
Há quanto tempo? ................................................
19. Motivo pelo qual o exame está sendo solicitado
1. Avaliar indicação de tratamento
2. Monitorar o tratamento
3. Falha ou troca de terapêutica
ZAIDAN, A.M. E.
ANEXOS
Caracterização genética do vírus da hepatite B...
102
ZAIDAN, A.M. E.
Anexo A
Caracterização genética do vírus da hepatite B...
103
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
104
Anexo B
INSTRUCTIONS TO AUTHORS
•
•
Scope and policy
Format style
ISSN 0074-0276 printed version
ISSN 1678-8060 online version
Scope and policy
The Memórias do Instituto Oswaldo Cruz is a multidisciplinary journal which publishes
original research throughout the fields of tropical medicine (including pathology, field
epidemiology and clinical studies) medical and veterinary parasitology (including protozoology,
helminthology, entomology and malacology), and medical microbiology (virology, bacteriology
and mycology). It particularly welcomes basic and applied research in biochemistry, immunology,
molecular and cell biology, physiology, pharmacology and genetics related to these fields. Short
communications are also considered. Review articles are invited. The journal publishes eight
issues constituting one volume per year. Occasionally papers presented at symposia or congresses
are published as supplements.
Submitted papers must be written in Portuguese or English. English of low quality is a major
cause of delay in publication and we strongly advise authors with English as a foreign language to
have their manuscripts checked by someone with English as a first language, preferably a scientist.
Submission of a paper to the Memórias is understood to imply that is has not previously been
published (except in an abstract form), and that it is not being considered for publication
elsewhere. Responsibility for the accuracy of the material in the manuscript, including
bibliographic citations, lies entirely with the authors.
Manuscripts will be peer-reviewed; acceptance will be based on scientific content and presentation
of the material.
Submission of manuscripts will only be accepted when submitted electronically using the
following link: http://submission.scielo.br/index.php/mioc/login.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
105
With this service you can submit manuscripts, you will be able to check the content of your
submission, the electronic file will be used for editorial assessment and online refereeing, and the
editorial decision on the manuscript will be communicated to you.
By using this service you will guarantee fast and safe submission of your manuscript, and speed
the assessment process.
The manuscript should be prepared according to Author Guidelines
Authors submitting a manuscript do so on the understanding that if accepted for publication,
copyright of the article, including the right to reproduce the article in all form and media, shall be
assigned exclusively to the Memórias. The journal will not refuse any reasonable request by
authors for permission to reproduce any contribution.
For other instructions the authors should consult and follow the most recent number of the
Memórias or consult the home-page of the Memórias (http://memorias.ioc.fiocruz.br/), or contact
the Editorial Office by phones (+55-21-2598.4335/2561-1442), Fax (+55-21-2280.5048), or emails ([email protected] /[email protected]).
Format style
The manuscript should be prepared using standard word processing software and should
be printed (font size 12) double-spaced throughout the text, figure captions, and references, with
margins of at least 3 cm. The figures should come in the extension tiff, with a minimum resolution
of
300
dpi.
Tables
and
figures
should
come
in
separate
documents.
The manuscript should be arranged in the following order:
Running title: with up to 40 characters (letters and spaces)
Title: with up to 250 characters
Author's names: without titles or graduations
Intitutional affiliations: full address of the corresponding author only
Summary: up to 200 words (100 words in case of short communications). It should emphasize
new and important aspects of the study or observations.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
106
Key words: 3-6 items must be provided. Terms from the Medical Subject Headings (Mesh) list of
Index Medicus should be used.
Sponsorships: indicating the sources of financial support and change of address
Introduction: should set the purpose of the study, give a brief summary (not a review) of
previous relevant works, and state what new advance has been made in the investigation. It should
not include data or conclusions from the work being reported.
Materials and Methods: should briefly give clear and sufficient information to permit the study
to be repeated by others. Standard techniques need only be referenced.
Ethics: when reporting experiments on human subjects, indicate whether the procedures followed
were in accordance with the ethical standards of the responsible committee on human
experimentation (institutional or regional) and with the Helsinki Declaration of 1975, as revised in
1983. When reporting experiments on animals, indicate whether the institution's or a national
research council's guide for, or any national law on the care and use of laboratory animals was
followed.
Results: should be a concise account of the new information discovered, with the least personal
judgement. Do not repeat in text all the data in the tables and illustrations.
Discussion: should be limited to the significance of the new information and relate the new
findings to existing knowledge. Only unavoidable citations should be included.
Acknowledgements: should be short and concise, and restricted to those absolutely necessary.
References: must be accurate. Only citations that appear in the text should be referenced.
Unpublished papers, unless accepted for publication, should not be cited. Work accepted for
publication should be referred to as "in press" and a letter of acceptance of the journal must be
provided. Unpublished data should only be cited in the text as "unpublished observations", and a
letter of permission from the author must be provided. The references at the end of the paper
should be arranged in alphabetic order according to the surname of the first author.
The titles of journals should be abbreviated according to the style used in the Index Medicus.
Consult:
http://www.ncbi.nlm.nih.gov/sites/entrez?db=journals&TabCmd=Limits
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
107
• In the text use authors' surname and date:
Lutz (1910) or (Lutz 1910)
With two authors it is:
(Lutz & Neiva 1912) or Lutz and Neiva (1912)
When there are more than two authors, only the first is mentioned:
Lutz et al. (1910) or (Lutz et al. 1910).
• At the end of the paper use the following styles:
Journal article
Chagas C, Villela E 1922. Forma cardiaca da tripanosomiase americana. Mem Inst Oswaldo Cruz
14: 15-61.
Book and Thesis
Forattini OP 1973. Entomologia Médica. Psychodidae, Phlebotominae, Leishmaniose,
Bartonelose, Vol. IV, Edgard Blucher, São Paulo, 658 pp.
Morel CM 1983. Genes and Antigens of Parasites. A Laboratory Manual, 2nd ed., Fundação
Oswaldo Cruz, Rio de Janeiro, xxii + 580 pp.
Mello-Silva CC 2005. Controle alternativo e alterações fisiológicas em Biomphalaria glabrata
(Say, 1818), hospedeiro intermediário de Schistosoma mansoni Sambom, 1907 pela ação do látex
de Euphorbia splendens var. hislopii N.E.B (Euphorbiaceae), PhD Thesis, Universidade Federal
Rural do Rio de Janeiro, Seropédica, 85 pp.
Chapter in book
Cruz OG 1911. The prophylaxis of malaria in central and southern Brasil. In R Ross, The
Prevention of Malaria, John Murray, London, p. 390-398.
Journal article on the Internet
Abood S. Quality improvement initiative in nursing homes: the ANA acts in an advisory role.
Am J Nurs [serial on the Internet]. 2002 Jun [cited 2002 Aug 12];102(6):[about 3 p.]. Available
from:
http://www.nursingworld.org/AJN/2002/june/Wawatch.htm
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
108
Monograph on the Internet
Foley KM, Gelband H, editors. Improving palliative care for cancer [monograph on the Internet].
Washington: National Academy Press; 2001 [cited 2002 Jul 9]. Available from:
http://www.nap.edu/books/0309074029/html/.
Homepage/Web site
Cancer-Pain.org [homepage on the Internet]. New York: Association of Cancer Online Resources,
Inc.; c2000-01 [updated 2002 May 16; cited 2002 Jul 9]. Available from: http://www.cancerpain.org/.
Part of a homepage/Web site
American Medical Association [homepage on the Internet]. Chicago: The Association; c19952002 [updated 2001 Aug 23; cited 2002 Aug 12]. AMA Office of Group Practice Liaison; [about
2 screens]. Available from:
http://www.ama-assn.org/ama/pub/category/1736.html
DATABASE ON THE INTERNET
Open database:
Who's Certified [database on the Internet]. Evanston (IL): The American Board of Medical
Specialists. c2000 - [cited 2001 Mar 8]. Available from: http://www.abms.org/newsearch.asp
Closed database:
Jablonski S. Online Multiple Congenital Anomaly/Mental Retardation (MCA/MR) Syndromes
[database on the Internet]. Bethesda (MD): National Library of Medicine (US). c1999 [updated
2001 Nov 20; cited 2002 Aug 12]. Available from:
http://www.nlm.nih.gov/mesh/jablonski/syndrome_title.html
Part of a database on the Internet
MeSH Browser [database on the Internet]. Bethesda (MD): National Library of Medicine (US);
2002 - [cited 2003 Jun 10]. Meta-analysis; unique ID: D015201; [about 3 p.]. Available
from:
http://www.nlm.nih.gov/mesh/MBrowser.html Files updated weekly. Updated June 15, 2005
• Illustrations: figures and tables must be understandable without reference to the text.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
109
- Figures presented in tiff format with a minimum of 300 dpi and photographs must be sharply
focused, well contrasted, and if mounted onto a plate, the figures should be numbered
consecutively with Arabic numbers. Magnification must be indicated by a line or bar in the figure,
and referenced, if necessary in the caption (e.g., bar = 1 mm). Plates and line figures should either
fit one column (8 cm) or the full width (16.5 cm) of the page and should be shorter than the page
length to allow inclusion of the legend. Letters and numbers on figures should be of a legible size
upon reduction or printing. A colour photograph illustrates the cover of each issue of the Journal
and authors are invited to submit illustrations with legends from their manuscript for
consideration for the cover.
- Tables should supplement, not duplicate, the text and should be numbered with Roman
numerals. A short descriptive title should appear above each table, with any explanations or
footnotes (identified with a, b, c, etc.) below.
•Short communications: should communicate rapidly single results or techniques. They should
occupy no more than three printed pages including figures and/or tables. They should not contain
excessive references. References should be cited at the end of the paper using the same format as
in full papers. A brief summary and three key words must be provided.
• Alternative format: manuscripts may be submitted following the "Uniform Requirements for
Manuscripts Submitted to Biomedical Journals" produced by the International Committee of
Medical Journal Editors also known as the Vancouver Style. In this case, authors should follow
the guidelines in the fifth edition (Annals of Internal Medicine 1997; 126: 36-47, or at the website
http://www.acponline.org/journals/resource/unifreqr/htm) and will be responsible for modifying
the manuscript where it differs from the instructions given here, if the manuscript is accepted for
publication.
Authors should also follow the Uniform Requirements for any guidelines that are omitted in these
Instructions.
Once a paper is accepted for publication, the authors must provide:
• an affidavit, provided by the Editorial Office, signed by all authors. Authors from different
countries or institutions may sign in different sheets containing the same basic statement;
• a copyright assignment form, provided by the Editorial Office, signed by the corresponding
author.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
110
•Page charges: there will be no page charges.
•Proofs: one set of page proofs will be supplied for the author to check for typesetting accuracy,
to be returned by the stipulated date. No changes to the original manuscript will be allowed at this
stage.
[Home] [About the journal] [Editorial board] [Subscription]
© 2009 Fundação Oswaldo Cruz
Av. Brasil, 4365
21040-900 Rio de Janeiro RJ Brazil
Tel.: +55 21 2598-4335
Fax: +55 21 2280-5048 / 2561-1442
[email protected]
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
111
Anexo C
Transactions of The Royal Society of Tropical Medicine and Hygiene
Guide for Authors
Online submission of manuscripts is now available here.
Guide for Authors
Manuscripts should be submitted online at:
http://www.ees.elsevier.com/trstmh/
Address for Correspondence
The Editor-in-Chief
Transactions Editorial Office
ISSN: 0035-9203
Royal Society of Tropical Medicine and Hygiene
Imprint: ELSEVIER 50 Bedford Square
London WC1B 3DP
UK
Tel: +44 (0)20 7580 2127
Fax: +44 (0)20 7436 1389
e-mail: [email protected]
Article types
The Transactions publishes:
Original Articles - 3500 words, abstract 200 words, 30 references;
Short Communications - 800 words, 1 table or figure, abstract 100 words, 5 references;
Case Reports - 800 words, 1 table or figure, abstract 100 words, 5 references;
Leading Articles - 800 words, abstract 100 words, 5 references;
Reviews - 3500 words, abstract 200 words, 30-40 references;
Mini-reviews - 800 words, abstract 100 words, 5 references;
Correspondence - 500 words, 3 references;
Images - a picture and 300 words, 3 references.
General
Authors are advised to consult the Submission checklist(below) to guide their writing and submission.
Submission of an article implies that the work described has not been published previously (except in the form of an abstract or as part of a
published lecture or academic thesis), that it is not under consideration for publication elsewhere, that its submission and potential
publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if
accepted, it will not be published elsewhere in the same form, in English or in any other language, without the written consent of the
copyright-holder.
Authors are advised to consult Appendix 1 (Special Subject Repositories) if their funding agency has a public access policy.
Authors are required to consult Appendix 2 (Proofs) to ensure that they understand their role in the processing of their manuscript after
acceptance.
The detailed requirements for Manuscripts are set out in sections 1-6 below.
Submission checklist
It is hoped that this list will be useful during the final checking of an article prior to sending it to the journal's editor for review.
Ensure that the following items are present:
• One author designated as corresponding author
• e-mail address
• Full postal address
• Telephone and fax numbers
• One or more contributors designated as guarantors of the paper
Statements on the following are included:
• Authors' contributions
• Acknowledgements
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
112
• Funding
• Conflicts of interest
• Ethical clearance
All necessary files have been uploaded in the following order: • Manuscript file (containing title page, summary, keywords, the main text of
the manuscript, references, tables and figure legends; tables can be attached as separate files if necessary)
• Figure file(s)
• Cover letter
• Authors' agreements
Article written in good English
Manuscript has been 'spellchecked'
References are in the correct format for this journal
All references mentioned in the Reference list are cited in the text, and vice versa Permission has been obtained for use of copyrighted
material from other sources (including the Web)
Colour figures are clearly marked as being intended for colour reproduction or to be reproduced in black-and-white
For further information please contact the Author Support Department at [email protected]
Editorial process
On receipt in the Editorial Office your manuscript will be subject to detailed scrutiny with respect to both format and content. The Editors
will assign the article to subject experts for peer review. The purpose of this review is to guide the editors in their decisions. If it is
considered appropriate the comments will be made available to the authors and will guide in any revision.
Should authors be requested by the Editor to revise the text, the revised version should be submitted within the proscribed period. After this
period, the article will be regarded as a new submission.
1. Article content
Original Articles and Short Communications
These provide accounts of original investigations in all aspects of tropical medicine and international health including:
• Chemotherapy and chemoprophylaxis
• Clinical tropical medicine
• Epidemiology
• Infectious diseases
• Immunology and vaccines
• Laboratory studies
• Microbiology and virology
• Noncommunicable and chronic disease
• Parasitology and entomology
• Public health and social medicine
• Qualitative and quantitative studies
Animal studies and in vitro studies will be considered only in so far as the results are directly relevant to human health.
Short Communications
These are similar to original articles but do not include sufficient new information to warrant a full-length article. The Results and Discussion
sections can be combined if appropriate.
Case Reports
These report in detail significant and rare conditions. Historically large numbers of such reports have been published but in future only those
providing valuable clinical lessons or new insights will be accepted.
Leading Articles
These set in context and illustrate the significance of articles published in the Transactions and are usually written as a result of a specific
invitation. The Editor may invite Leading Articles on other topics that highlight developments in tropical medicine and international health.
Reviews
These give an authoritative account of an aspect of tropical medicine and international health. The intention is that these reviews will provide
the readers with an insight into topics of current interest and to widen the scope of the journal to bring to the attention of readers emerging
diseases and other developing aspects of International Health. Reviews do not recapitulate material found in postgraduate textbooks.
Mini-reviews
These do not reiterate accepted ideas and information but rather challenge the reader with new thoughts that will stimulate debate; lead to the
emergence of new ideas and approaches that may change policy in International Health and Tropical Medicine The purpose of a mini-review
may be:
• To highlight and set in context a recent discovery
• To critically appraise and cast in a new light established information and ideas
• To illustrate how information and ideas established in one place or at one time can be relevant in a new context
• To suggest ways in which insights from other disciplines may be of value in the understanding of International Health and Tropical
Medicine
• To show how established policy in International Health and Tropical Medicine may have unintended consequences.
Correspondence
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
113
The Transactions accepts correspondence from readers related to published papers and from Society Fellows on other matters of current
concern. Authors will be asked to respond to comments on their papers and letters will be published together.
Images
The Transactions will publish images that illustrate all aspects of tropical medicine and international health. An author submitting an image
will provide an explanation of its significance. Copyright of the image will become the property of the Transactions and it may be used by
http://www.elsevier.com/artworkinstructions
the Society as it sees fit. A detailed guide on electronic artwork is available on the website
2. Presentation of manuscript
2.1. General
We expect documents to be prepared in Microsoft (MS) Word. Always keep a backup copy of the electronic file for reference and safety.
Save your files using the default extension of Word. Files should not be saved as 'read-only'.
Manuscripts must be written in good English and the spelling should follow that in the Oxford English Dictionaries. Italics should not be
used for expressions of Latin origin, for example, in vivo, et al., per se. A single 12-point font should be used for the whole of the
manuscript, preferably Arial. The text should be in single-column format and the pages should be numbered consecutively. Double spacing
should be used throughout including the references, tables and legends to figures. Punctuation should be consistent and only a single space
should be inserted between words and after punctuation. Each new paragraph should be clearly indicated (use two hard returns at the end of
each paragraph). The whole text, including headings and references, should be aligned left and ragged right. Formatting should be kept to an
absolute minimum as most formatting codes will be removed and replaced on processing the article, in particular, do not use the Word
options to hyphenate words. However, do use bold face, italics, subscripts, superscripts, etc. where appropriate. Do not embed 'graphically
designed'
equations
or
tables.
Authors in Japan kindly note that, upon request, Elsevier Japan will provide authors with a list of people who can check and improve the
English
of
their
paper
(before
submission).
Please
contact
our
Tokyo
office: Elsevier K.K., 4F Higashi-Azabu, 1-Chome Bldg, 1-9-15 Higashi-Azabu, Minato-ku, Tokyo 106-0044, Japan, tel.: (+81) (3) 5561
5037; fax: (+81) (3) 5561 5047, e-mail: [email protected]
2.2. Title page (should include the following in the order given)
Title. Concise and informative. Titles are often used in information-retrieval systems. Avoid abbreviations and formulae where possible.
Author names and affiliations. The forename(s) or initial(s) and surname(s) should be included for all the authors. Where the family name
may be ambiguous (e.g. a double name), please indicate this clearly. The authors' affiliation addresses (where the actual work was done)
should be listed below the names. Indicate all affiliations with a lowercase superscript letter immediately after the author's name and in front
of the appropriate address. Provide the full postal address of each affiliation, including the country name.
Corresponding author. The post-publication corresponding author should be indicated by an asterisk after the author's name and before
'Corresponding author' in the footnote. In the footnote, include the full postal address if it is different from that in the affiliation or the author
has more than affiliation, telephone and fax numbers (with country and area code) and e-mail address.
Present/permanent address. If an author has moved since the work described in the article was done, or was visiting at the time, a 'Present
address' (or 'Permanent address') may be indicated as a footnote to that author's name. The address at which the author actually did the work
must be retained as the main, affiliation address. Superscript Arabic numerals are used for such footnotes.
Running title. A short informative running title of no more than 50 characters.
2.3. Summary
A concise and factual summary is required (maximum length 200 words). Summaries for short communications, case reports, mini-reviews
and leading articles are limited to 100 words. Do not use subheadings. The summary should state briefly the purpose of the research, the
principal results and major conclusions. A summary is often presented separate from the article, so it must be able to stand alone.
No references should be included in the summary.
Non-standard or uncommon abbreviations should be avoided, but if essential they must be defined at their first mention in the summary.
Keywords
Immediately after the summary, provide six keywords, avoiding general and plural terms and multiple concepts (avoid, for example, 'and',
'of'). Be sparing with abbreviations: only abbreviations firmly established in the field may be eligible. Authors are recommended to use
keywords from the National Library of Medicine's Medical Subject List, wherever possible. The suitability of keywords can be checked on
http://www.nlm.nih.gov/mesh/2007/MBrowser.html
the NLM MeSH Browser at
Choosing keywords in this manner may help increase citation of your paper by making it more readily searchable.
2.4. Arrangement of the article
When appropriate divide your article into clearly defined sections. Mini-reviews and letters are not subdivided. Each subsection should be
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
114
given a brief heading. Each heading should appear on its own separate line in bold type. Subsections should be used as much as possible
when cross-referencing text: refer to the subsection by heading as opposed to simply 'the text'. The subdivisions set out below relate to
original articles, the subdivision of reviews is dictated by the subject matter and will be suggested by the author.
Introduction. State the objectives of the work and provide an adequate background, avoiding a detailed literature survey or a summary of the
results.
Experimental/Materials and methods. Provide sufficient detail to allow the work to be reproduced. Methods already published should be
indicated
by
a
reference:
only
relevant
modifications
should
be
described.
Theory and/or calculation. A Theory section should extend, not repeat, the background to the article already dealt with in the Introduction
and lay the foundation for further work. In contrast, a Calculation section represents a practical development from a theoretical basis.
Results. The results should be precisely presented once in the text, tables or figures without discussion of their significance. When results are
presented in tables or figures the text should comment only on the important points. Tables and figures with legends should be able to stand
alone.
Discussion. This should explore the significance of the results, not repeat them. The limitations of the study should be highlighted where
relevant.
The main conclusions of the study should be presented in a short concluding paragraph at the end of the Discussion section.
Declarations. Statements on the authors' contributions, acknowledgements, funding, conflicts of interest and ethical approval must be placed
after
the
Discussion
section
(see
paragraphs
below
for
more
detail).
If you have no declaration to make for funding, conflicts of interest and ethical approval please insert the following statements:
Funding: None.
Conflicts of interest: None declared.
Ethical approval: Not required.
Please note the statement that ethical approval is not required, should not reflect the authors' opinion but indicate that advice has been
properly
sought
and
that
the
approval
has
been
deemed
unnecessary.
2.5. References
Responsibility for the accuracy of bibliographic citations lies entirely with the authors. The style of citation and referencing was changed in
June 2008. Authors may find it helpful to refer to a copy of the Lancet to familiarize themselves with the new style. This will be similarly
helpful to those using a reference manager system.
Citations in the text. Please ensure that every reference cited in the text is also present in the reference list (and vice versa). Unpublished
results and personal communications should not be in the reference list, but may be mentioned in the text. Citation of a reference as 'in press'
implies that the item has been accepted for publication.
Text. Indicate the references by superscript numbers in the text. The actual authors can be referred to, but the reference number(s) must
always be given.
List. Number the references in the list in the order in which they appear in the text.
Examples:
Reference to a journal publication:
1.Van der Geer J, Hanraads JAJ, Lupton RA. The art of writing a scientific article. J Sci Commun 2000, 163: 51-9.
Reference to a book:
2.Strunk Jr W, White EB. The Elements of Style. 3rd ed. New York: Macmillan; 1979.
Reference to a chapter in an edited book:
3.Mettam GR, Adams LB. How to prepare an electronic version of your article. In: Jones BS, Smith RZ. Introduction to the Electronic Age.
New York: E-Publishing Inc; 1999, p 281-304.
Please note the shortened form of the last page number e.g., 51-9 and that for more than 6 authors the first 6 should be listed followed by 'et
al'. For further details you are referred to "Uniform Requirements for Manuscripts submitted to Biomedical Journals" (J Am Med Assoc 1997,
http:/www.nlm.nih.gov/tsd/serials/terms_cond.html
277:
927-34).
See
also
Online references
Such article citations should include DOI (digital object identifier). The DOI is a persistent identifier, which remains with the article even
http://www.dx.doi.org/
after
it
is
published
in
print.
See
For example: 4.Boutayeb A, Twizell EH, Achouayb K, Chetouani A. A mathematical model for the burden of diabetes and its complications.
Biomed Eng Online 2004, DOI: 10.1186/1475-925X-3-20.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
115
2.6. Tables
Number tables consecutively in accordance with their appearance in the text. Each table must have a self-explanatory title and abbreviations
that are not standard in this field must be defined. Place footnotes to tables below the table body and indicate them with lowercase
superscript letters. Avoid vertical and horizontal rules apart from the horizontal rules above and below the Table, and one below the column
headings extending over the full width of the Table. Be sparing in the use of tables and ensure that the data presented in tables do not
duplicate results described elsewhere in the article. Tables must be prepared using a spreadsheet or the Tables function of Microsoft Word,
i.e. they must be cell based [tabs and hard returns must not be used to separate columns and rows].
2.7. Figure legends
Number figures consecutively in the order in which they are referred to in the text. Subdivided figures should be marked A, B, C, etc. and
referred to in the text as 1A, 1B, 1C, etc. Each figure must have a self-explanatory legend which should comprise a brief title and description
of the figure. Keep text in the figures themselves to a minimum but explain all symbols and abbreviations used. Figure legends should be
listed
on
a
separate
page
of
the
end
of
the
manuscript
file,
not
attached
to
the
figure(s).
2.8. Figures
See detailed note below.
3. Specific journal style
Abbreviations. Define abbreviations that are not standard in this field at their first occurrence in both the summary and the main text. Ensure
consistency of abbreviations throughout the article.
Mathematical formulae. Present simple formulae in the line of normal text where possible. In principle, variables are to be presented in
italics. Use the solidus (/) instead of a horizontal line, e.g. Xp/Ym.
Powers of e are often more conveniently denoted by exp.
Number consecutively any equations that have to be displayed separate from the text (if referred to explicitly in the text).
Nomenclature and units. Follow internationally accepted rules and conventions: use the international system of units (SI). If other quantities
are mentioned, give their equivalent in SI. You are urged to consult IUB: Biochemical Nomenclature and Related Documents
http://www.chem.qmul.ac.uk/iupac/bibliog/white.html for further information.
Organisms
should
be
referred
to
by
their
scientific
names
according
to
the
Linnaean
binomial
system.
Italics must be used for generic and specific names and for genes.
Generic names should be given in full and in italics when first used and subsequently abbreviated to a single letter in italics followed by a
full stop and a space, e.g. Plasmodium vivax and P. vivax. The full generic name should always be used at the beginning of a sentence or in a
heading or subheading. Use one letter for genus abbreviation except when a two letter abbreviation is needed to avoid confusion, e.g. when
Aedes and Anopheles, are mentioned in same paper. However, when several unusual genera are being discussed with only a few references to
each spread throughout the manuscript it is better to use the whole generic name.
Numbers one to nine are spelt unless they are measurements, e.g. 5 mg. Numbers (and units if appropriate) are spelled out if they begin a
sentence, e.g. Five microlitres. Large numbers should be set without commas, i.e. 10 000 not 10,000. Decimal points must be indicated by a
full point on the line (not commas). Decimal fractions should always be preceded by a zero, e.g. 0.05.
When reporting percentages in the text both the numerator and denominator should be included. When the sample size is greater than 100
percentages should be reported to no more than one decimal place. When the sample size is 100 or less, percentages should be reported in
whole
numbers.
Statistical methods with which readers may not be familiar should be fully referenced and details of any statistical software packages used
should be given, e.g. Epi Info (CDC, Atlanta, GA, USA). Precise values of P should be given where possible, to no more than two significant
figures, but P less than 0.001 should be used instead of smaller values.
Drug names. Generic names of drugs should be used. The proprietary name may be used together with the generic name where it is first
mentioned in the text and details of the manufacturer should be given (name, city, state, country).
DNA sequences and GenBank Accession numbers. Gene accession numbers refer to genes or DNA sequences about which further
information can be found in the databases at the National Center for Biotechnical Information (NCBI) at the National Library of Medicine.
Authors wishing to enable other scientists to use the accession numbers cited in their papers via links to these sources, should type this
information in the manner set out below.
For each and every accession number cited in an article, authors should type the accession number in bold, underlined text. Letters in the
accession number should always be capitalised. (See Example below). This combination of letters and format will enable Elsevier's
typesetters to recognize the relevant texts as accession numbers and add the required link to GenBank's sequences.
Example: '(GenBank accession nos. AI631510 , AI631511 , AI632198 and BF223228 ), a B-cell tumor from a chronic lymphatic leukemia
(GenBank accession no. BE675048 ), and a T-cell lymphoma (GenBank accession no. AA361117 )'.
Authors are encouraged to check accession numbers very carefully. An error in a letter or number can result in a dead link. In the final
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
116
version of the printed article, the accession number text will not appear bold or underlined. In the final version of the electronic copy, the
accession number text will be linked to the appropriate source in the NCBI databases enabling readers to go directly to that source from the
article.
Preparation of supplementary data. We welcome submission of electronic supplementary material to support and enhance your scientific
research. Supplementary files offer the author additional possibilities to publish supporting applications, movies, animation sequences, highresolution images, background datasets, sound clips and more. Supplementary files supplied will be published online alongside the electronic
http://www.sciencedirect.com/. In order to ensure that your
version of your article in Elsevier web products, including ScienceDirect at
submitted material is directly usable, please ensure that data are provided in our recommended file formats. Authors should submit the
material in electronic format together with the article and supply a concise and descriptive caption for each file. For more detailed
http://www.elsevier.com/authors
instructions please visit
4. Preparation of electronic illustrations
Submitting your artwork in an electronic format helps us to produce your work to the best possible standards, ensuring accuracy, clarity and
a high level of detail.
General points
• Make sure you use uniform lettering, symbols and sizing in your original artwork
• Arial font should be used in illustrations if possible
• Where possible figures should be designed to fit a single column (80 mm width) with the degree of reduction to be determined by the
Publisher
• The axes of graphs should be carefully chosen so as to occupy the space available to the best advantage
• Line drawings should be as simple as possible: many computer-generated figures, e.g. three-dimensional graphs, fine lines, gradations of
stippling and unusual symbols, cannot be reproduced satisfactorily when reduced
• The lettering and symbols, as well as other details, should have proportionate dimensions, so as not to become illegible or unclear after
reduction
• Number the illustrations according to their sequence in the text
• Use a logical naming convention for your artwork files
• Provide all illustrations as separate files
• Provide legends to illustrations separately
A
detailed
guide
on
electronic
artwork
is
available
on
our
website:
http://www.elsevier.com/artworkinstructions
You are urged to visit this site; some excerpts from the detailed information are given here.
Formats
Regardless of the application used, when your electronic artwork is finalized, please 'save as' or convert the images to one of the following
formats (note the resolution requirements for line drawings, halftones, and line/halftone combinations given below):
• EPS: Vector drawings. Embed the font or save the text as 'graphics'
• TIFF: Colour or greyscale photographs (halftones): always use a minimum of 300 dpi
• TIFF: Bitmapped line drawings: use a minimum of 1000 dpi
• TIFF: Combinations bitmapped line/half-tone (colour or greyscale): a minimum of 500 dpi
• DOC, XLS or PPT: If your electronic artwork is created in any of these Microsoft Office applications please supply 'as is'
Please do not: • Supply embedded graphics in your document
• Supply files that are optimised for screen use (like
• Supply files that are too low in resolution
• Submit graphics that are disproportionately large for the content
GIF,
BMP,
PICT,
WPG);
the
resolution
is
is
required
too
low
Colour illustrations
If, together with your accepted article, you submit usable colour figures then Elsevier will ensure, at no additional charge, that these figures
will appear in colour on the web (e.g. ScienceDirect and other sites) regardless of whether or not these illustrations are reproduced in colour
in the printed version. For colour reproduction in print, you will receive information regarding the costs from Elsevier after receipt of your
accepted article.
Please note: Because of technical complications that can arise by converting colour figures to 'grey scale' (for the printed version should you
not opt for colour in print) please submit in addition usable black and white illustrations corresponding to all the colour illustrations.
5. Online submission to the journal
These instructions apply to all articles submitted to the journal. Variations applicable to some types of article are noted in the appropriate
sections.
http://ees.elsevier.com/trstmh/), where you will be guided stepwise
Authors should upload their article via the journal's homepage (
through the creation and uploading of the various files. Once the uploading is done, the system generates an electronic (PDF) version of the
article which is used for the reviewing process. Authors, Reviewers and Editors send and receive all correspondence by e-mail and no paper
correspondence is necessary.
The above represents a very brief outline of online submission. It can be advantageous to print this 'Guide for Authors' section from the site
for
reference
in
the
subsequent
stages
of
article
preparation.
Please submit, with the manuscript, the names and e-mail addresses of two potential referees. You may also mention persons who you would
prefer not to review your paper.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
117
6. Formal requirements
These matters relate to the integrity of the publication process. You need to be aware of these matters.
6.1. Authorship
‘
For articles published in this journal, a person listed as an author must have made a substantial contribution to:
• the conception and design of the study, or the analysis and interpretation of data
• drafting the article or revising it critically for intellectual content
• giving final approval of the version to be published
ALL these conditions must be met.
Acquisition of funding, collection of data, or general supervision of the research group, alone, does not justify authorship.
Designation as an author infers a responsibility for the integrity and accuracy of all the data published. One or more of the authors should be
listed as guarantors of the paper. The guarantor accepts full responsibility for the conduct of the study, had access to the data and controlled
the decision to publish. Normally the corresponding author will be a guarantor but this must be explicitly stated.
At the end of each paper the contributions of each author to the study and its publication must be listed. We encourage intending authors to
discuss this amongst themselves and agree the precise nature of each person's contribution. Authors must ensure that all authors listed meet
the above criteria for authorship and that there is no one else who fulfils the criteria but has not been included as an author.
When a large, multi-centre group has conducted the work, the group should identify the individuals who accept direct responsibility for the
manuscript. These individuals should fully meet the criteria for authorship defined above.
It is the duty of the corresponding author/guarantor to ensure that each author has signed a declaration concerning his or her individual
contribution. Any consequences that result from failure to do so will be the sole responsibility of the author/guarantor who is advised to keep
copies of these declarations on file in case of dispute. The following format is suggested "I declare that in this article entitled {title of article}
I participated in {here list contributions made to the study} and that I have seen and approved the final version. I have the following
competing interests {here list competing interests}." You will be required to send us signed copies of these statements. These signatures need
not be dated and the documents must be submitted via the online submission system.
Authors' contributions. The contributions of each author to the study and its publication must be listed (see detailed note above). We suggest
the following format (please use initials to refer to each author's contribution): BJA and CJ designed the study protocol; BJA and HGM
carried out the clinical assessment; CJ and FT carried out the immunoassays and cytokine determination, and analysis and interpretation of
these data. BJA and CJ drafted the manuscript. All authors read and approved the final manuscript. BJA and CJ are guarantors of the paper.
Acknowledgements. You should acknowledge here anyone who has contributed towards the study by providing study materials or helped in
data acquisition or analysis, or helped care for patients, but who does not meet the criteria for authorship. Persons providing purely technical
help or writing assistance should be listed in this section.
Authors
should
obtain
permission
to
acknowledge
from
all
those
named
in
the
Acknowledgements.
Alterations to authorship or acknowledged contributors. All authors must approve any change in authors and acknowledged contributors
after initial submission. This applies to additions, deletions, change in order of authors, or contributions being attributed differently. The
editor may contact any of the authors or contributors to ascertain whether they have agreed to any alteration.
6.2. Funding
Please list the source(s) of funding for the study and for each author, and for the manuscript preparation. If the funding body contributed in
any way to study design, or the collection, analysis, and interpretation of data, or the writing of the manuscript, and/or the decision to submit
the manuscript for publication, this should be explicitly stated. Full details of the funding bodies must be given, i.e. name, city, state, country
and any grant/reference numbers or other identifiers included.
6.3. Conflicts of interest
A competing interest arises when a professional judgment concerning a primary interest (such as the conduct of a trial, a patient's welfare or
the validity and interpretation of the research) tends to be unduly influenced by financial gain or other self-interested motive which may be at
odds with professional obligations. Authors should disclose at the time of submission information on financial competing interests that may
influence the manuscript and summarise these interests under the competing interests declaration in the final manuscript. Authors must
declare other interests that could influence the results of the study or the conclusions of the manuscript (e.g. employment, academic links,
family relationships, political or social interest group membership, deep personal conviction, consultancies, stock ownership, honoraria, paid
expert testimony, patent applications/registrations, and grants or other funding). For further information, see the web site of the International
http://www.icmje.org/sponsor.htm.
Committee of Medical Journal Editors at
6.4. Ethical issues
Work on human beings that is submitted to Transactions should comply with the principles laid down in the Declaration of Helsinki;
Recommendations guiding physicians in biomedical research involving human subjects. Adopted by the 18th World Medical Assembly,
Helsinki, Finland, June 1964, amended by the 29th World Medical Assembly, Tokyo, Japan, October 1975, the 35th World Medical
Assembly, Venice, Italy, October 1983, and the 41st World Medical Assembly, Hong Kong, September 1989. The manuscript should contain
a
statement
that
the
work
has
been
approved
by
the
appropriate
ethical
committees
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
118
related to the institution(s) in which it was performed and that subjects gave informed consent to the work. Studies involving experiments
with animals must state that their care was in accordance with institution guidelines.
Studies on patients or volunteers require ethics committee approval and informed consent which should be documented in your paper.
Patients have a right to privacy. Therefore identifying information, including patients? images, names, initials, or hospital numbers, should
not be included in videos, recordings, written descriptions, photographs, and pedigrees unless the information is essential for scientific
purposes and you have obtained written informed consent for publication in print and electronic form from the patient (or parent, guardian or
next of kin where applicable). If such consent is made subject to any conditions, Elsevier must be made aware of all such conditions. Written
consents must be provided to Elsevier on request. Even where consent has been given, identifying details should be omitted if they are not
essential. If identifying characteristics are altered to protect anonymity, such as in genetic pedigrees, authors should provide assurance that
alterations do not distort scientific meaning and editors should so note. If such consent has not been obtained, personal details of patients
included in any part of the paper and in any supplementary materials (including all illustrations and videos) must be removed before
submission.
6.5. Clinical trials registration
All randomised controlled trials submitted for publication in Transactions should include a completed Consolidated Standards of Reporting
http://www.consort-statement.org/ for more
Trials (CONSORT) flow chart. Please refer to the CONSORT statement website at
information. Transactions has adopted the proposal from the International Committee of Medical Journal Editors (ICMJE) which require, as
a condition of consideration for publication of clinical trials, registration in a public trials registry. Trials must register at or before the onset
of patient enrolment. The clinical trial registration number should be included at the end of the summary and in the Materials and Methods
section of the text. For this purpose, a clinical trial is defined as any research project that prospectively assigns human subjects to
intervention or comparison groups to study the cause-and-effect relationship between a medical intervention and a health outcome. Studies
designed for other purposes, such as to study pharmacokinetics or major toxicity (e.g. phase I trials) would be exempt. Further information
http://www.elsevier.com/wps/find/journaldescription.cws_home/681019/www.icmje.org.
can
be
found
at
Which trial registries are acceptable to the Transactions?
Acceptable registries must:
• be accessible to the public at no charge
• open to all prospective registrants, i.e. investigators are able to register without restriction by geographic location, academic affiliation,
patient demographics, or clinical condition
• managed by a not-for-profit organization
• have a mechanism to ensure the validity of the registration data
• be electronically searchable
• include the required data elements
The following registries have been reviewed by the International Committee of Medical Journal Editors (ICMJE) and met their criteria as of
January 2006. These are currently the registries which are acceptable to the Editor of the Transactions. This list will be updated when the
ICMJE revises its list of registries in April 2007.
http://www.actr.org.au/
1.
http://www.clinicaltrials.gov/
2.
http://www.isrctn.org/
3.
http://www.umin.ac.jp/ctr/index/htm
4.
http://www.trialregister.nl/
5.
The World Health Organization is also working towards the implementation of an international trials registration process. Its most recent
http://www.who.int/mediacentre/news/releases/2006/pr25/en/index.html
statement
(May
2006)
can
be
accessed
at
Registration of clinical trials
Publication of the results of trials beginning on or after 1 July 2005 will only be considered if registration occurred before the first patient
was enrolled.
What do we do about trials that began before 1 July 2005?
Investigators wishing to publish their work in the Transactions should register trials that began enrolling patients before 1 July 2005 as soon
as possible. We will accept retrospective registration of trials that began before 1 July 2005, i.e. registration occurred after patient enrolment
began.
A trial will be considered as ongoing if investigators were still collecting, cleaning or analysing data as of 1 July 2005. All ongoing trials
require registration before being submitted to the Transactions.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
119
6.6. Copyright
Upon acceptance of an article, authors will be asked to sign a "Journal Publishing Agreement'' (for more information on this and copyright
http://www.elsevier.com/authorsrights). Acceptance of the agreement will ensure the widest possible dissemination of information.
see
An e-mail (or letter) will be sent to the corresponding author confirming receipt of the manuscript together with a 'Journal Publishing
Agreement' form.
If excerpts from other copyrighted works are included, the author(s) must obtain written permission from the copyright owners and credit the
source(s) in the article. Elsevier has preprinted forms for use by authors in these cases : contact Elsevier's Rights Department, Philadelphia,
PA, USA: Tel. (+1) 215 238 7869; Fax (+1) 215 238 2239; e-mail [email protected]. Requests may also be completed online
http://www.elsevier.com/locate/permissions).
via the Elsevier homepage (
Appendix 1
Funding body agreements and policies
Elsevier has established agreements and developed policies to allow authors whose articles appear in journals published by Elsevier, to
comply with potential manuscript archiving requirements as specified as conditions of their grant awards. To learn more about existing
http://www.elsevier.com/fundingbodies
agreements
and
policies
please
visit
Appendix 2
Proofs
One set of page proofs in PDF format will be sent by e-mail to the corresponding author, to be checked for typesetting/editing. No changes
in, or additions to, the accepted (and subsequently edited) manuscript will be allowed at this stage. Proofreading is solely your responsibility.
A form with queries from the copyeditor may accompany your proofs. Please answer all queries and make any corrections or additions
required. Return corrections within 5 days of receipt of the proofs. Should there be no corrections, please confirm this. The Publisher
reserves the right to proceed with publication if corrections are not communicated. When the edited manuscript is received by the Publisher it
is considered to be in its final form. Proofs are not to be regarded as 'drafts'. Elsevier will do everything possible to get your article corrected
and published as quickly and accurately as possible. In order to do this we need your help. When you receive the (PDF) proof of your article
for correction, it is important to ensure that all of your corrections are returned to Elsevier in one communication. Subsequent corrections
will not be possible, so please ensure your first sending is complete. Note that this does not mean you have any less time to make your
corrections just that only one set of corrections will be accepted.
ZAIDAN, A.M. E.
Caracterização genética do vírus da hepatite B...
Anexo D
#MIOC-1302 : Hepatitis B virus genotypes circulating in Alagoas, Brazil
•
EDITING
Submission
Authors
Title
Original file
Supp. files
Submitter
Date submitted
Section
Editor
ALBA MARIA XAVIER ELOY
Hepatitis B virus genotypes circulating in Alagoas, Brazil
MIOC-1302-11468-53981-1-SM.DOC 2009-04-16
ADD A SUPPLEMENTARY FILE
None
ALBA MARIA XAVIER ELOY
April 16, 2009 - 05:34 PM
Full Paper
None assigned
Status
Status
Initiated
Last modified
Awaiting assignment
2009-04-16
2009-04-16
Av. Brasil, 4365 - Manguinhos - 21040-900 Rio de Janeiro - RJ - Brasil
Fax:+55-21-2562-1220 | Tel. +55-21-2562-1222
E-mails: [email protected]
120
ZAIDAN, A.M. E.
Anexo E
Caracterização genética do vírus da hepatite B...
121