ANTICOAGULAÇÃO NA F. ATRIAL:
QUANDO INDICAR, COMO ESCOLHER E O
QUE ORIENTAR PARA O PACIENTE ?
Dra Olga F. de Souza
Doutora em Cardiologia pela UFRJ
Coordenadora do Serviço de Arritmia, Eletrofisiologia e
Estimulação cardíaca artificial
Fibrilação Atrial: Epidemiologia
• FA é responsável por 15 milhões de AVC/ano no mundo.
• A FA é uma causa de AVC que pode ser prevenida em 15%-30%
dos casos (AVC mais graves e incapacitantes).
• O aumento da sobrevida do IAM e o envelhecimento da
população são fatores que contribuem para o aumento da
incidência de AVC relacionado à FA.
• Na prática 80% dos pacientes com FA tem indicação de
anticoagulação oral
TRATAMENTO INICIAL DA FA
ESTRATIFICAÇÃO DE RISCO DE EVENTOS
TROMBOEMBÓLICOS
FATORES DE RISCO PARA AVC
CHA2DS2-VASC
CHA2DS2-VASc criteria
Score
Congestive heart failure/
left ventricular dysfunction
1
Hypertension
1
Age 75 yrs
2
Diabetes mellitus
1
Stroke/transient ischaemic attack/TE
2
Vascular disease (prior myocardial
infarction, peripheral artery disease
or aortic plaque)
1
Age 65–74 yrs
1
Sex category (i.e. female gender)
1
Lip G et al. Chest 2010;137:263-72; Lip G et al. Stroke 2010; 41:2731–8;
Camm J et al. Eur Heart J 2010; 31: 2369–429; Hart RG et al. Ann Intern
Med 2007;146:857–67
Total
score
Patients
(n=7329)
Adjusted
stroke rate
(%/year)*
0
1
0.0
1
422
1.3
2
1230
2.2
3
1730
3.2
4
1718
4.0
5
1159
6.7
6
679
9.8
7
294
9.6
8
82
6.7
9
14
15.2
Theoretical rates without therapy; assuming that
warfarin provides a 64% reduction in stroke risk,
based on Hart RG et al. 2007.
Avaliação do risco de Sangramento Maior
HAS-BLED
Sigla
Fator de Risco
Pontuação
H
Hipertensão Arterial (PAS>160mmHg)
1
A
Disfunção renal = ClearCrea ≤ 50mL/min ou Creatinina
≥ 2,26 mg/dL ou hemodiálise ou transplante renal
1
Disfunção hepática = [Bilirrubina ≥ 2x LSN + (AST ou
ALT ou FALC ≥ 3x LSN)] ou cirrose hepática
1
S
AVC prévio
1
B
Sangramento prévio ou predisposição a sangramentos
1
L
RNI lábil ou < 60% do tempo na faixa terapêutica
1
E
Idade > 65 anos
1
D
Drogas (AINE/AINH, antiplaquetários)
1
Abuso de álcool (>20 U por semana)
1
Pisters R et al. Chest. 2010; Lip GYH et al. BMJ. 2011;
ESC Guidelines: Camm J et al. Eur Heart J 2010;31:2369–429;
EHRA/ESC Position Paper : Lip GYH et al. Europace 2011;13:723–746
HAS-BLED
Escore ≥ 3
Alto risco de
Sangramento Maior
(4,9-19,6% ao ano)
INDICAÇÃO DE ANTICOAGULAÇÃO
Estratificação de Risco - CHA2DS2-VASC
Avaliação do risco de sangramento pelo HAS-BLED
Avaliação de contra-indicações: hipersensibilidade, hepatopatias,
IR grave, gravidez, amamentação e menores de 18 anos
Classificação temporal da FA (< ou > 48 horas) para reversão na
sala de emergência ou ambulatorial
COMO ESCOLHER E O QUE ORIENTAR
PARA O PACIENTE ?
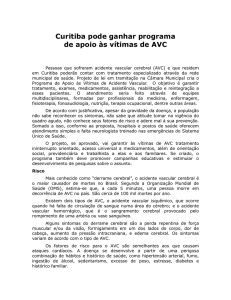
Anticoagulantes orais
Via extrínseca
Via intrínseca
XII
Xl
IX
Varfarina
TF
VII
VIIIa
X
Xa
Inibidores diretos do fator Xa
• rivaroxabana
• apixabana
IIa
Inibidor direto da trombina
• dabigatrana
Va
II
I
Coágulo
de fibrina
1. Adapted fromVerheugt FW. Nat Rev Cardiol. 2010;7(3):149-154
Antes de iniciar o tratamento
• Histórico do paciente - CHA2DS2-VASC e HAS-BLED
• Medicamentos utilizados
• AINH
• Antiagregantes plaquetários
• Função renal: calcular Clearance de Creatinina(Cockroft Gault )
• Função hepática
Expert Opin. Pharmacother G. Palareti et al. 2013.
INDICAÇÕES ESPECÍFICAS PARA OS DIFERENTES NOVOS
ANTICOAGULANTES
Características farmacocinética e farmacodinâmica dos NOACS
Metanálise dos estudos com NOACS
Indicações Específicas
Seleção dos NOACS de acordo com as indicações específicas
Estudos dos NOACs na prevenção do AVC em FA:
delineamento e parâmetros
Parâmetro
RELY
ROCKET-AF
ARISTOTLE
ENGAGE
Multicêntrico,
randomizado, PROBE
(desfechos cegados)
Multicêntirco,
randomizado, duplo-cego
Multicêntirco,
randomizado, duplocego
Multicêntirco,
randomizado, duplocego
18.113
14.264
18.201
21105
AVC ou Embolia Sistêmica
AVC ou Embolia Sistêmica
AVC ou Embolia
Sistêmica
AVC ou Embolia
Sistêmica
Sangramento maior,
incluindo fatal e que
ameaça a vida
Composição de
sangramento maior e nãomaior clin relevante
Sangramento maior
(critério do ISTH )
Sangramento maior
(critério do ISTH )
2,0
1,8
1,9
2,8
71,5 (média)
73 (mediana)
70 (mediana)
72
Clearance de Creatinina
(mediana, ml/min)
68
67
Não relatado
Não relatado
CHADS2 Score (média)
2.1(110mg) / 2.2 (150mg)
3,5
2,1
2,8
64
55
62
68
10–15% em 01 ano
16–21% em 02 anos
23,7% em aprox. 02 anos
25,4% em aprox. 1,8
anos
8.8 ao ano
Desenho
Pacientes Randomizados
Desfecho Primário Eficácia
Desfecho Primário
de Segurança
Duração de Seguimento (a)
Idade (anos)
Tempo em faixa terapêutica
TTR (média%)
Descontinuação
Análise Estatística
ITT
Per protocolo e ITT
ITT
MITT e ITT
Connolly SJ, et al. N Engl J Med 2009;361:1139–51;Connolly SJ et al. N Engl J Med 2010;363:1875–6;Patel MR, et al. N Engl J Med 2011;365:883–91;Granger C,
et al. N Eng J Med 011;365:981–92; Giugliano R et al. N Engl J Med 2013;369:2093-104
NOACs : metabolização e eliminação
Heidbuchel H. et al. Europace 2013;15:625–51
Interação medicamentosa
Para treinamento interno apenas – Confidencial Daiichi Sankyo Versão 1.0_2013-11-19
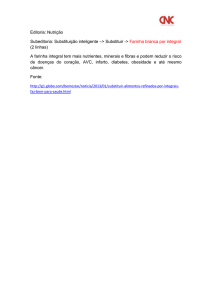
All NOACs (Meta-Analysis): Stroke or SEE
Risk Ratio (95% CI)
0.66 (0.53 - 0.82)
RE-LY
[150 mg]
ROCKET AF
0.88 (0.75 - 1.03)
ARISTOTLE
0.80 (0.67 - 0.95)
ENGAGE AF-TIMI 48
0.88 (0.75 - 1.02)
[60 mg]
Combined
0.81 (0.73 - 0.91)
[Random Effects Model]
N=58,541
0.5
Heterogeneity p=0.13
p=<0.0001
Favors NOAC
1
Favors Warfarin
2
Ruff CT, et al. Lancet 2013
All NOACs: Secondary Efficacy Outcomes
Risk Ratio (95% CI)
Ischemic Stroke
0.92 (0.83 - 1.02)
p=0.10
Hemorrhagic Stroke
0.49 (0.38 - 0.64)
p<0.0001
MI
0.97 (0.78 - 1.20)
p=0.77
All-Cause Mortality
0.90 (0.85 - 0.95)
p=0.0003
0.2
0.5
Favors NOAC
1
2
Favors Warfarin
Heterogeneity p=NS for all outcomes
Ruff CT, et al. Lancet 2014;383:955-962
All NOACs (Meta-Analysis): Major Bleeding
Risk Ratio (95% CI)
0.94 (0.82 - 1.07)
RE-LY
[150 mg]
ROCKET AF
1.03 (0.90 - 1.18)
ARISTOTLE
0.71 (0.61 - 0.81)
ENGAGE AF-TIMI 48
0.80 (0.71 - 0.90)
[60 mg]
Combined
0.86 (0.73 - 1.00)
[Random Effects Model]
N=58,498
p=0.06
0.5
Heterogeneity p=0.001
Favors NOAC
1
Favors Warfarin
2
Ruff CT, et al. Lancet 2013
All NOACs: Secondary Safety Outcomes
Risk Ratio (95% CI)
0.48 (0.39 - 0.59)
ICH
p<0.0001
1.25 (1.01 - 1.55)
GI Bleeding
p=0.043
0.2
0.5
Favors NOAC
1
2
Favors Warfarin
Heterogeneity
ICH, p=0.22
GI Bleeding, p=0.009
Ruff CT, et al. Lancet 2014;383:955-962
Conclusions from Meta-Analysis Trials
NOACs significantly reduce stroke (19%)
Primarily driven by reduction in hemorrhagic stroke (51%)
NOACs significantly reduce mortality (10%)
Trend toward less bleeding
Substantial reduction in ICH (52%)
Increased GI bleeding (25%)
The relative efficacy and safety of NOACs consistent across a wide
spectrum of AF patients -Even less bleeding when INR not as well controlled
Low dose NOAC regimens reduce mortality and have a very favorable
bleeding profile but more ischemic events
Differences in agents, patients, and trials may not be accounted for
Heterogeneity major bleeding and GI bleeding
Doses dos NOACS
RE-LY1
ROCKET-AF2
ARISTOTLE3
ENGAGE-AF4
• 150 mg ou 110
mg 2 x ao dia
• Regimes de
doses diferentes
• ≥80 anos
• Clearance de
creatinina
30–50 mL/min
• 20→15 mg 1 x ao
dia para :
– Clearance de
creatinina
<30–49 mL/min
• 5→2.5 mg 2 x ao
dia:
• Redução ≥ 2
fatores
– ≥80 anos
– ≤60 kg
– Creatinina
≥1.5 mg/dL
• 60→30 mg 1x ou
30→15 mg 1 x
para:
– Clearance de
creatinina
30–50 mL/min
– ≤60 kg
– Quinidina, ou
verapamil
# 10%
1. Connolly et al. N Engl J Med 2009;361:1139–1151
2. Patel et al. N Engl J Med 2011;365:883–891
3. Granger et al. N Engl J Med 2011;365:981–992
4. Giugliano RP et al. N Engl J Med 2013;369:2093-2104
6.4%
25%
Variáveis a serem analisadas na
escolha dos NOACS
Análise da função renal
Interações medicamentosas
Presença de dispepsia ou passado de doença gástrica
Perfil de segurança do NOACS
Presença de DAC
Resultados de eficácia e segurança em meta-análise:
NOACS comparados à varfarina em FANV
Eficácia (redução de AVC e
Embolia Sistêmica)
Segurança (Sangramento Maior)
Melhor
Dabigatrana 150 mg 2xd
RR 0.66 (95% CI, 0.53–0.82)
Edoxabana 30 mg 1xd
HR 0.47 (97.5% CI, 0.41–0.55)
Apixabana 5 mg 1xd
HR 0.79 (95% CI, 0.66–0.95)
Apixabana 5 mg 2xd
HR 0.69 (95% CI, 0.60–0.80)
Edoxabana 60 mg 1xd
HR 0.87 (97.5% CI, 0.73–1.04)
Dabigatrana 110 mg 2xd
RR 0.80 (95% CI, 0.69–0.93)
Rivaroxabana 20 mg 1xd
HR 0.88 (95% CI, 0.74–1.03)
Edoxabana 60 mg 1xd
HR 0.80 (97.5% CI, 0.71–0.91)
Dabigatrana 110 mg 2xd
RR 0.91 (95% CI, 0.74–1.11)
Dabigatrana 150 mg 2xd
RR 0.93 (95% CI, 0.81–1.07)
Edoxabana 30 mg 1xd
HR 1.13 (97.5% CI, 0.96–1.34)
Rivaroxabana 20 mg 1xd
HR 1.04 (95% CI, 0.90–1.20)
Pior*
Os resultados em negrito demonstraram uma redução na significância estatística
RR, Risco relativo; HR, hazard ratio; CI, intervalo de confiança. FANV: fibrilação atrial não valvar
*Note que a “pior” estimativa do risco ainda é não inferior à varfarina.
Schulman S. Thromb Haemost. 2014 Apr 1;111(4):575-82. doi: 10.1160/TH13-09-0803. Epub 2014 Jan 23.
O QUE AS DIRETRIZES RECOMENDAM ?
Atualização dos Guidelines
Prevenção de AVC em FA (ESC 2012)
FA valvar
FA não valvar
Yes
(doença reumática e
prótese metálica)
<65 anos & FA isolada (incluindo mulheres)
Varfarina
No
Avaliar risco (CHA2DS2-VASc score)
0
1
≥2
melhor opção
Terapia Anticoagulante
Opção
alternativa
Avaliar risco de sangramento(HAS-BLED score)
Considerar preferência do paciente
Nenhuma terapia
antitrombótica
NOAC
VKA
Adapted from Camm AJ et al. Eur Heart J. 2012;33:2719-2747
Características Clinicas
COMO ESCOLHER O ANTICOAGULANTE ORAL ?
Alto risco de sangramento, ex
HAS-BLED > 3; muito idosos
Considerar fármaco / dose com a mais
baixa incidência de angramento
Dabi 110,
Edox, Apix
Alto risco de AVC isquemico, baixo
risco de sangramento
Considerar fármaco / dose com a
melhor redução de AVC isquêmico
Dabi 150
AVC prévio
(prevenção secundária)
Considerar o fármaco de melhor
investigação,maior redução 2º AVC
Riva, Apix,
Edox
DAC, IAM prévio ou alto risco para
SCA/IAM
Considerar fármaco com efeitos
positivos na SCA
**Riva, Edox
Comprometimento da função renal
Considerar fármaco menos
dependente da função renal
Apix, Edox DR
30 Riva 15
Uso concomitante de inibidor CYP
Considerar fármaco com nenhum ou
pouco metabolismo via CYP
Dabi, Edox
Preferência do paciente
Considerar uma vez ao dia
Riva, Edox
Cardioversão Elétrica Eletiva
CARDIOVERSÃO ELÉTRICA COM WARFARINA
Complicações cerebrovasculares sintomáticas
13/ 5247 pts
0.24%
0.7%
0.5%
0.4%
0.3%
0
1841 pts
664 pts
521 pts
275 pts
1946 pts
CARDIOVERSÃO ELÉTRICA COM NOACS
Complicações cerebrovasculares sintomáticas
2
1,8
1,6
1,4
1,2
1
0,8
0,6
0,4
0,2
0
9/1708 pts
0,52%
CHADS 3.5
1.6%
CHADS 2.1-2.2
0.8%
CHADS 2.1
0.30%
0
647 pts
Dabigatran 110
672 pts
Dabigatran 150
Nagarakanti R et al Circulation 2011
265 pts
Rivaroxaban
Piccinini et al JACC 2013
265 pts
Apixaban
Flaker G. et al JACC 2014
ESC 2015
Need for cardioversion
(electrical or medical)
Patiente on NOAC for 3w
-
Patiente not anticoagulated
Inquire patient about adherence to NOAC intake
-Make note about patient answer in the chart
Deemed welladherent
Doubt about
adherence or deemed
high-risk for left atrial
thrombus:
- Perform TOE
AF > 48h
Randomized:
Cappato et al, Eur Heart J 2014 (X-VeRT)
- 463 OAC naive patients => ‘early’ arm (of whom 305
received rivaroxan)
- - 64.7% underwent TOE in ‘early arm’
- - no difference in ischemic or bleeding events
Goal - early CV
-
Start NOAC 24h before
CV
Perform TOE before
CV (until more data
from ongoing trials)
If TDE detects atrial thrombus: postpone CV after longer period of anticoagulation, with repeat TOE (No data on best strategy: converting
to (heparin + ) VKA OR continuation of NOAC (trials ongoing)
Goal – late CV
-Treat with NOAC for
23w and ensure
adherence
See ‘Patiente on
NOAC for 23w’
Cardiovert
Continue NOAC for at least 4 weeks (longer based on CHA2DS2-VASc)
Heidbuchel et al, Updated EHRA Practical Guide on NOAC in AF, EP Europace (2015)
OBRIGADA
Efective PCI with
newer generation
DES or BMS
1 year
6 months
3 months
Triple
therapy
NOAC + A +
C
1 month
Discharge
...
Double therapy
NOAC + A or C
NOAC
monothera
py
Alternative: DAPT only, if CHA, DS, VASc + 1 (men) or 2 (women) (only CAD) & elevated bleeding risk
Acute
coronary
syndrome
Triple therapy
NOAC + A + C
Double therapy
NOAC + A or C
NOAC
monothera
py
Factors to shorten combination-therapy
-
(Uncorrectable) high bleeding risk
Low artherothrombotic risk (by REACH or SYNTAX score if elective?; GRACE > 118 if ACS?)
Factors to lengthen combination therapy
Heidbuchel et al, Updated EHRA Practical Guide on NOAC in AF, EP Europace (2015)
First-generation DES
High atherothrombotic risk (scores as above; stenting of the left main, proximal left anterior
descending, proximal bifurction; recurrent Mis; etc.) and low bleeding risk