LUXAÇÃO INVETERADA DO OMBRO
ATUALIZAÇÃO / UPDATE
Luxação inveterada do ombro
Chronic unreduced shoulder dislocation
MARCO ANTONIO DE CASTRO VEADO1
RESUMO
ABSTRACT
O melhor tratamento para a luxação inveterada do
ombro é, na verdade, a prevenção. Por isso, devem ser sempre valorizados a história clínica e o exame físico. Atenção
redobrada deve ser dada aos pacientes epilépticos, alcoólatras, politraumatizados e àqueles em tratamento prolongado de “capsulite adesiva”. A incidência em axilar na
investigação radiológica é indispensável, pois ela é a chave
para o diagnóstico. Muitas vezes “o não fazer nada” constitui a melhor forma de tratamento dessa lesão. No planejamento operatório, identificar: o tamanho do defeito da
cabeça umeral, as perdas ósseas da glenóide, o estado do
manguito rotador, principalmente o do músculo subescapular, e as lesões nervosas. A tomografia computadorizada e a ressonância magnética são exames complementares de grande valia. Para o ato cirúrgico são indispensáveis:
material apropriado, auxiliares treinados e em número
suficiente. Redução aberta está bem indicada nos casos
mal definidos ou que datem mais de duas semanas do trauma. As cirurgias reconstrutoras são a indicação de eleição
nos pacientes mais jovens e com lesão da cabeça umeral
menor que 45% da superfície articular. As hemiartroplastias são a melhor escolha quando o defeito umeral está
acima desse percentual, e as artroplastias totais quando
há comprometimento da glenóide, sempre dependendo da
integridade do manguito rotador. É indicação questionável operar paciente desmotivado, pouco disposto a submeter-se ao programa de reabilitação funcional.
The best treatment for the chronic shoulder dislocation is
undeniably the prevention. Therefore, the clinical history
and physical examination must always be valued. Doubled
attention must be paid to epileptic patients, alcoholics, multiple injured patients, and those with a prolonged treatment
of “adhesive capsulitis”. The radiographic axillary view is
essential, as it is the key for the diagnosis. Many times the
“do not touch” is the best form of treatment for such injury.
During operative planning, the size of the humeral head
defect, glenoid bone losses, rotator cuff status, mainly the
subscapularis muscle, and nerve injuries must be identified.
Computerized tomography and magnetic resonance imaging are complementary tests of great value. Appropriate
material, trained and numerically sufficient surgical personnel are essential for the surgical procedure. Open reduction is well indicated for ill-defined cases or those evolving
more than two weeks from the trauma. Reconstruction procedures are indicated for younger patients, and those with a
humeral head lesion corresponding to less than 45% of the
joint surface. Hemiarthroplasties are the best choice when
the humeral defect is above that percentage, and total arthroplasties suit better glenoid compromising, ever depending on the rotator cuff integrity. It is debatable whether to
operate an unmotivated patient, who would not be ready to
be submitted to a functional rehabilitation program.
Key words – Shoulder; hemiarthroplasty; rotator cuff
Unitermos – Ombro; hemiartroplastia; manguito rotador
1. Cirurgião de Ombro do Hospital Mater Dei e Hospital da Previdência-IPSEMG de Belo Horizonte/MG; Professor da Faculdade de Ciências Médicas de
Minas Gerais-Hospital Universitário São José.
1. Shoulder Surgeon, Hospital Mater Dei and Hospital da Previdência –
IPSEMG, Belo Horizonte, Minas Gerais, Brazil; Associate Professor, Faculdade de Ciências Médicas de Minas Gerais-Hospital Universitário São José,
Belo Horizonte, Brazil.
Endereço para correspondência (Correspondence to): Av. Celso Porfírio Machado, 104 – 30320-400 – Belo Horizonte, MG. Tels.: (31) 3286-3156 (residência), 32615700 e 3261-5157 (consultório). E-mail: [email protected].
Copyright RBO2004
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
1
M.A. CASTRO VEADO
INTRODUÇÃO
INTRODUCTION
Segundo Loebenberg e Cuomo, foi White quem, pela primeira vez, em 1741, publicou comentários sobre o tratamento da luxação posterior crônica do ombro, chamando atenção
para a gravidade dessas lesões, mostrando seu resultado final
sombrio(1).
According to Loebenberg and Cuomo, White first published
in 1741 commentaries on the treatment of the chronic posterior shoulder dislocation, calling attention to the severity of
those injuries, with a reserved outcome(1).
Centuries have been through and this diagnosis is still being neglected. With the advances in the knowledge and treatment of shoulder diseases, unreduced chronic dislocation has
been sporadically found in orthopedic practice.
The diagnosis is eventually known, but the many patients –
mainly the poorest – do not have their problem solved due to
precarious conditions of our health system, the region where
they live, or the lack of somebody able to solve the problem.
Alcoholics, diabetics (seizures due to nocturnal hypoglycemia), and epileptic patients that use anticonvulsive medications erratically are often subject to have their dislocation
neglected, whereas the same happens with comatose victims
of serious accidents, with multiple injuries in the ICU, where
other higher-risk injuries demand the attention of the attending team(2,3).
Quite frequently the patient does not safely inform how long
has the shoulder been dislocated, posing a great risk, as attempts of closed reduction may fracture the humerus, already
atrophic by disuse, thus compelling the orthopedic surgeon to
carry out an eventually complex open reduction, without previous preoperative planning.
Time produces capsule, tendon and muscle scarring and
adhesions, making the reduction difficult, and eventually impossible. The humeral head cartilage softening, along with
intense soft tissue contracture and important glenoid bone
loss, are quite often times associated to fractures and nerve
injuries, predicting a poor outcome for those injuries(2).
When is a dislocation considered to be chronic?
In accordance to Schultz et al, a dislocation is considered
chronic after 24 hours of an unrecognized trauma(4). Others
consider after 45 days(5), although most – according to Rowe
and Zarins – stated a period above 21 days(6). We consider
that after the second week of trauma, we must be prepared for
an open reduction.
As to the direction of displacement, there is no agreement
either.
According to Schultz et al, and Rowe and Zarins, the posterior dislocation is more frequent than the anterior dislocation. Seizures account for 1/3 of posterior dislocations, and
half of anterior dislocations(4,6). Buhler and Gerber showed,
however, an equal frequency between both(7). Our experience
Séculos já se passaram e esse diagnóstico continua sendo
negligenciado. Com o avanço no conhecimento e no tratamento das afecções do ombro, a luxação crônica não reduzida tem sido encontrada na prática ortopédica de maneira esporádica.
Algumas vezes, o diagnóstico é conhecido, mas muitos pacientes, principalmente os mais humildes, não têm o problema resolvido devido às condições precárias do nosso sistema
de saúde, da região que habitam ou pela falta de alguém capaz de solucionar o problema.
Pacientes alcoólatras, diabéticos (convulsão por hipoglicemia noturna), epilépticos que fazem uso de medicamentos
anticonvulsivantes de maneira desordenada estão sujeitos com
freqüência a ter sua luxação negligenciada, o mesmo ocorrendo com vítimas de acidentes graves, em coma, com múltiplas lesões, internados em CTI, quando outras lesões de maior
risco e importância desviam a atenção da equipe de atendimento(2,3). Com muita freqüência, o paciente não informa com
segurança há quanto tempo o ombro está luxado, decorrendo
daí grande risco, pois as tentativas de redução incruenta podem fraturar o úmero já atrofiado por desuso, ou então obrigar o ortopedista a realizar uma redução aberta, às vezes complexa, sem prévio planejamento operatório.
O tempo faz com que as contraturas e aderências da cápsula, tendões e músculos dificultem a redução, tornando-a impossível após certo tempo. O amolecimento da cartilagem da
cabeça umeral deslocada, junto com intensa contratura de tecidos moles e perda óssea importante na glenóide, muitas vezes associada às fraturas e lesões nervosas, fazem com que
essas lesões tenham prognóstico reservado(2).
Quando uma luxação é considerada crônica?
Segundo Schultz et al, quando não são reconhecidas após
as 24 horas do trauma(4). Outros acham que seria após 45 dias(5),
embora a maioria, segundo Rowe e Zarins, estabeleça o prazo
como superior a 21 dias(6). A nossa opinião é de que após a
segunda semana do trauma já devemos estar preparados para
uma redução aberta.
Em relação à direção do deslocamento, também não existe
concordância.
2
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
LUXAÇÃO INVETERADA DO OMBRO
in 12 cases of our sampling of
Na experiência de Schultz
unreduced dislocations showet al e Rowe e Zarins, o desed the same frequency as to the
locamento posterior é mais
incidence of anterior and posfreqüente que o anterior com
terior dislocations.
as crises convulsivas resIn a research performed in
pondendo por 1/3 das luxaNew England, USA, 33% of the
ções posteriores e metade das
surgeons with one to five years’
anteriores(4,6). Buhler e Gerexperience had dealt with at
ber mostraram, entretanto,
least one case of chronic
freqüência igual entre as
shoulder dislocation, whilst
duas(7). Nossa experiência
the incidence was of 90% for
em 12 casos de luxação irrethose with more than 20 years’
dutível mostra também igual
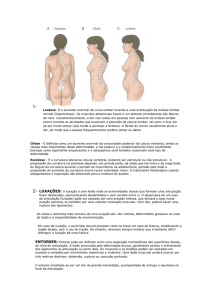
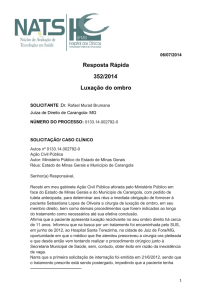
freqüência em relação à in- Fig. 1 – Radiografia do ombro em axilar mostrando uma luxação experience. Therefore, the experience with chronic glenocidência de luxação anterior posterior
Fig. 1 – Shoulder axillary view showing a posterior dislocation
humeral dislocation is directe posterior.
ly linked to the time length of
Em pesquisa realizada em
orthopedic practice(6).
New England, EUA, 33% dos
cirurgiões com um a cinco anos de experiência viram ou traIn 1855, according to Matsen and Rockwood, Malgaigne
taram pelo menos um caso de luxação crônica do ombro, enpublished on 37 cases of posterior dislocations, based solely
quanto a incidência foi de 90% naqueles com mais de 20 anos
on careful observation, about 40 years before the discovery
de experiência. Portanto, a experiência com a luxação escaof X-rays.
puloumeral crônica está diretamente relacionada com o temA careful clinical history, a thorough physical examinapo de prática do ortopedista(6).
tion, added to the essential axillary view, are the key for the
Em 1855, segundo Matsen e Rockwood, Malgaigne publicorrect identification of the injury that will take us straight to
cou 37 casos de luxação posterior, cerca de 40 anos antes da
the diagnosis(1,2,8,9) (figure 1).
descoberta do RX, unicamente baseado em sua atenta obserThere must be a high degree of suspicion about a blocked
vação(8).
dislocation, especially a posterior dislocation, whenever a
História clínica minuciosa, exame físico atento e detalhapatient presents with shoulder pain and range of motion limdo, aliados à investigação radiológica com a indispensável
itation that are resistant to treatment.
incidência em axilar, são a chave para a correta identificação
Once the diagnosis of unreduced chronic shoulder dislocada lesão e nos levarão certamente ao diagnóstico(1,2,8,9) (fig. 1).
tion is done, there are some questions to be asked. The most
Suspeitar sempre da luxação bloqueada, principalmente a
important, according to some authors, is to know if the paposterior, frente a qualquer paciente com dor e limitação de
tient is symptomatic(2,3,10).
It is not uncommon to find patients presenting old, painmovimentos do ombro resistentes ao tratamento.
free dislocations, with reasonable range of motion. ObviousUma vez diagnosticada a luxação crônica não reduzida do
ly, those patients will not be candidates for a surgical interombro, existem vários questionamentos a ser feitos. O mais
vention (figure 2).
importante, segundo alguns autores, é saber se o paciente é
Another aspect to consider is the rehabilitation. It is imsintomático(2,3,10).
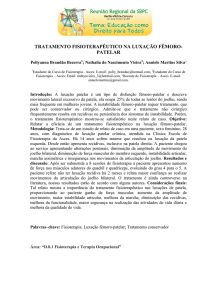
Não é incomum encontrarmos pacientes com luxações anportant to previously identify if the patient has capability, motigas sem dor e com amplitude razoável de movimentos. Obtivation, and conditions to take the long and intense program
viamente, que esses não serão candidatos a uma intervenção
of physical therapy that follows the surgery; alcoholics, epicirúrgica (fig. 2).
leptics and people at the lowest social level are not usually
Outro aspecto diz respeito à reabilitação. É importante idencooperative.
tificar previamente se o paciente tem habilidade, motivação e
The type of surgical procedure and its prognosis will dicondições de cumprir o prolongado e intenso programa de
rectly depend on the time frame that the humeral head had
fisioterapia que se segue à cirurgia: alcoólatras, epilépticos e
lost its relation with the glenoid.
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
3
M.A. CASTRO VEADO
A
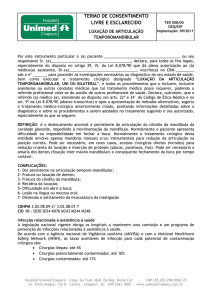
Fig. 2 – A) Paciente com uma luxação anterior crônica não reduzida
há mais de cinco
anos, assintomática; B) Aspecto
radiológico.
B
Fig. 2 – A) Asymptomatic patient
with chronic anterior dislocation
for more than five
years. B) Radiological aspect.
aqueles com baixo nível social costumam não ser cooperativos.
O tipo de cirurgia realizada e seu prognóstico vão depender diretamente do tempo que a cabeça umeral perdeu sua
relação com a glenóide.
O tamanho e a localização dos defeitos da cabeça, perdas
ósseas na glenóide e lesões do manguito rotador, principalmente a do tendão do músculo subescapular, devem ser cuidadosamente avaliados para que um adequado planejamento
operatório seja feito(1).
4
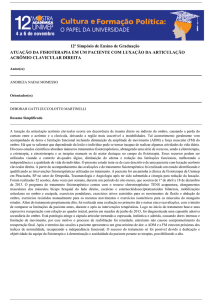
Fig. 3 – Radiografia em AP do ombro mostrando uma lesão de
Hill-Sachs
Fig. 3 – Shoulder AP X-ray showing Hill-Sachs lesion
Head bone defects size and location, glenoid bone loss and
rotator cuff injuries – mainly the subscapularis muscle – must
be carefully assessed for an adequate preoperative planning(1).
CHRONIC ANTERIOR DISLOCATION
Shoulder anterior dislocation is one of the most familiar
injuries to the orthopedic surgeon, and the diagnosis seldom
goes unnoticed if seen during the acute phase. As previously
mentioned, patients with mental state alteration or carriers
of unknown seizures may deny important information about
timing and cause of the injury.
It is not difficult to find that the humeral head is out of the
glenoid, viewed from an anteroposterior X-ray incidence. The
posterolateral humeral head defect (Hill-Sachs lesion) may
be sufficiently large in long standing cases (figure 3). As time
goes by, there is a “false” glenoid formation within the scapular anterior neck, where the dislocated humeral head is(2,3).
The axillary X-ray view seals the diagnosis of dislocation
direction(1,2,5,11) and, when associated to computerized tomography, it may show glenoid fractures and humeral head defect size(1,2,3,8).
Magnetic resonance imaging is not needed for those cases,
but it helps to check the subscapularis muscle tendon status,
as it is the main passive stabilizer on the anterior dislocation.
Sometimes after reduction of the anterior dislocation, it
recurs due to an anterior glenoid rim fracture, a situation
that may not be diagnosed, especially in the aged and osteoporotic(2,3,8) (figure 4).
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
LUXAÇÃO INVETERADA DO OMBRO
LUXAÇÃO ANTERIOR CRÔNICA
A luxação anterior do ombro é das lesões mais familiares
ao ortopedista e o diagnóstico dificilmente passa despercebido se visto na fase aguda. Como dito anteriormente, pacientes
com estado mental alterado ou portadores de crise convulsiva
não conhecida podem sonegar informações importantes em
relação ao tempo e causa da lesão.
Com uma radiografia feita em AP no plano do corpo não é
difícil perceber que a cabeça umeral encontra-se fora da glenóide. O defeito póstero-lateral na cabeça umeral (lesão de
Hill-Sachs) pode ser bastante grande em casos de longa duração (fig. 3). Com o tempo, forma-se uma “falsa” glenóide no
colo anterior da escápula, que está em contato com a cabeça
deslocada(2,3).
A radiografia axilar é definitiva para o diagnóstico da direção da luxação(1,2,5,11) quando associada à tomografia computadorizada, pode mostrar fraturas da glenóide e dimensionar
o defeito da cabeça umeral(1,2,3,8).
A ressonância magnética é dispensável nesses casos, mas
ajuda a verificar o estado do tendão do músculo subescapular,
já que ele é o principal estabilizador passivo na luxação anterior.
Algumas vezes, após a redução da luxação anterior, esta se
refaz em função da presença de fratura da borda anterior da
glenóide, situação que pode não ser diagnosticada, principalmente nos idosos osteoporóticos2,3,8 (fig. 4).
Em presença de lesão nervosa concomitante, particularmente do nervo axilar, é necessário documentá-la, se possível com
eletroneuromiografia, comunicando a complicação ao paciente
antes da realização de qualquer procedimento.
TRATAMENTO DA LUXAÇÃO
ANTERIOR CRÔNICA
O tratamento dessa condição pode variar desde uma conduta expectante, passando pela redução aberta com reconstrução articular e enxerto ósseo, chegando até mesmo à artroplastia.
Uma clara e sincera conversa com o paciente e familiares
deve acontecer a fim de mostrar-lhes a difícil situação a enfrentar.
O desafio maior é o de escolher o tipo de procedimento
mais adequado para cada paciente.
Às vezes, o melhor é não fazer nada, apesar de o deslocamento anterior crônico ser mal tolerado pelo paciente quando
comparado com o posterior. Neste, ele consegue alcançar a
face e a boca devido à contratura fixa do membro em rotação
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
A
C
B
D
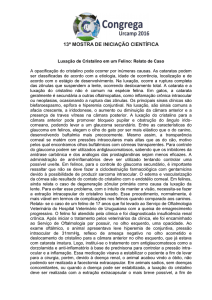
Fig. 4 – A) Radiografia em AP mostrando uma luxação anterior
associada a uma fratura da borda anterior da escápula. B) Tomografia computadorizada. Feita redução incruenta da luxação com
perda posteriormente dentro do Velpeau. C e D) Redução aberta
e preenchimento do defeito ósseo com o processo coracóide três
meses após o trauma.
Fig. 4 – A) AP X-ray showing anterior dislocation associated to
anterior scapular rim fracture. B) Computerized tomography.
Closed reduction of dislocation and further loss of reduction within
Velpeau immobilization. C and D) Open reduction and bone defect filling with coracoid process three months after the trauma.
In presence of a concurrent nerve injury, particularly the
axillary nerve, it is necessary to document the lesion with an
electromyography, telling the patient about the complication
before any procedure is performed.
TREATMENT OF CHRONIC
ANTERIOR DISLOCATION
The treatment of this condition may range from simply waiting to open reduction, and joint reconstruction to arthroplasty.
5
M.A. CASTRO VEADO
interna; na luxação anterior, o braço está fixo, afastado do
corpo e em rotação externa, situação que é mais incapacitante(6).
Redução fechada – Pode ser tentada com muita cautela
através de manipulação suave, estando o paciente com anestesia venosa e com bom relaxamento, até no máximo duas a
três semanas após a lesão. Segundo Matsen e Rockwood, se a
lesão data de uma semana ou mais, a redução fechada não
deve ser tentada porque a contratura de partes moles é tão
intensa que aumenta muito o risco de fratura no úmero(8). Nos
idosos os riscos são ainda maiores devido à menor elasticidade da parede das artérias e à osteoporose(6).
Nossa experiência é não insistir na redução de uma luxação com mais de duas semanas ou com data de ocorrência
mal definida.
Redução aberta – Deve ser realizada em luxações bloqueadas nas quais a tentativa de redução fechada não obteve
êxito. Até provavelmente seis meses considera-se a cartilagem ainda como preservada, sendo possível a reconstrução
articular. Nos casos mais graves é prudente deixar sempre um
cirurgião vascular de sobre-aviso, pois a intensa fibrose e a
anatomia alterada aumentam muito o risco de lesão dos vasos
axilares.
Preferimos o acesso deltopeitoral longo com o paciente na
posição de “cadeira de praia”. Liberação de parte da inserção
do peitoral maior, do músculo subescapular e da cápsula articular contraturada deve ser realizada, ao mesmo tempo que
ganhamos mais rotação externa, facilitando assim a capsulotomia posterior, num procedimento praticamente circunferencial. A ligadura da artéria umeral circunflexa anterior pode
ser necessária, bem como a visualização e proteção do nervo
axilar. Todo o conteúdo fibrótico da cavidade glenóide deve
ser removido para que a cabeça umeral possa ser adequadamente reduzida.
Após a redução, avaliamos a estabilidade da articulação,
isto é, a quantidade de rotação interna necessária para manter
a cabeça reduzida.
Alguns preferem a estabilização temporária com fios ou
parafusos(6,12) fixando-se a articulação glenoumeral ou o acrômio ao úmero, procedimentos criticados por Flatow et al(3).
Eles acham que, se é necessário o uso desses fios, é porque a
liberação não foi suficiente, o que facilitará a reluxação após
a retirada dos mesmos(2,3). Além do mais, os fios ou parafusos
causam dano à articulação (fig. 5).
Após a redução cirúrgica, tem sido a nossa preferência realizar a cirurgia de Bristow para evitar a luxação recidivante,
ao invés de procedermos ao reparo da lesão de Bankart. As
6
A direct and sincere talk with the patient and family must
take place to show the difficult situation they face.
A main challenge is to choose the most adequate type of
procedure for each patient.
Sometimes the best is to do nothing, despite that the chronic anterior dislocation is not as well tolerated as the posterior
dislocation by the patient. In the posterior dislocation, the
patient may reach the face and the mouth due to upper limb
fixed internal rotation, whereas in the anterior dislocation
the arm is fixed, away from the body, and in external rotation,
a more disabling situation(6).
Closed reduction – It may be carefully attempted by gentle
manipulation, having the patient under IV anesthesia and
adequate muscle relaxation, at the most within two to three
weeks after the injury. According to Matsen and Rockwood, if
the injury is older than one week or more, closed reduction
should not to be attempted, as soft tissue contracture is so
intense that it increases the risk of humeral fracture(8). In aged,
the risks are even higher due to lesser arterial wall elasticity
and osteoporosis(6).
In our experience, we do not insist on the reduction of a
dislocation with more than two weeks or an ill-defined occurrence date.
Open reduction – The attempt of closed reduction must be
performed in blocked dislocations, when a closed reduction
attempt had not succeeded. The cartilage is considered to be
preserved probably until six months, making possible the joint
reconstruction. In most serious cases, it is advisable to have a
vascular surgeon at hand, as the intense scarring and the modified anatomy largely increases the risk of axillary vessel injury.
We prefer the long deltopectoral approach, with the patient
on the beach chair position. A practically circumferential procedure is performed by the partial release of the pectoralis
major muscle, subscapularis muscle, and contracted joint
capsule insertions, at the same time that we get more external
rotation, thus facilitating a posterior capsulotomy. Anterior
humeral circumflex artery ligature may be necessary, as well
as axillary nerve viewing and protection. All glenoid cavity
fibrous content must be removed, so that the humeral head
can be adequately reduced.
After reduction, we assess joint stability, that is, the necessary amount of internal rotation to keep the head reduced.
Some favor temporary stabilization with wires or screws(6,12)
for glenohumeral joint or acromiohumeral fixation; Flattow
et al criticized both procedures(3). They found that the use of
those wires is explained due to an insufficient release, which
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
LUXAÇÃO INVETERADA DO OMBRO
A
B
Fig. 5 – A e B) Sexo masc., 43 anos, há oito meses com dor e
grande limitação de movimentos do ombro após crise de abstinência alcoólica. Pós-operatório: redução aberta instável (Bristow) e fixação com um fio de Steinmann.
Fig. 5 – A and B) Male, 43 years, with pain and great shoulder
range of motion limitation after alcohol withdrawal. Postoperative: unstable open reduction (Bristow), and Steinmann pin fixation.
grandes lesões de Hill-Sachs, maiores que 40% de defeito do
canto póstero-superior, facilitam a reluxação mesmo com pouca amplitude de rotação externa. Nesses casos, as reconstruções são necessárias.
As osteotomias rotacionais foram preconizadas pelo Grupo AO, mas somente para a instabilidade recidivante(13). Na
luxação crônica não existe nada publicado.
As ressecções da cabeça umeral não têm lugar como procedimento de primeira escolha, uma vez que as artroplastias
vieram para cobrir essa deficiência.
Naqueles com luxações mais antigas – com seis meses ou
mais – e com defeitos maiores que 40% da superfície articular, as artroplastias constituem a melhor opção, pois a cabeça
torna-se osteopênica e se achatará após a redução (cabeça tipo
bola de pingue-pongue)(1,2,3).
A maior complicação da prótese é a tendência para a luxação anterior. Nesses casos, aumento na retroversão é imprescindível(10,11).
Quando existe desgaste importante da glenóide anterior, é
necessário proceder ao abaixamento da glenóide posterior (2,3).
O osso ressecado da cabeça umeral pode também ser usado
como enxerto para aumentar a glenóide anterior. Se a cartilagem da glenóide está em boas condições, alguns associam à
hemiartroplastia, um reparo capsular semelhante ao reparo de
Bankart, para dar mais estabilidade à articulação(1).
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
will later facilitate a redislocation upon wire removal(2,3). In
addition, wires or screws damage the joint (figure 5).
After the surgical reduction, there has been our preference
to perform Bristow’s procedure to prevent the recurrent dislocation, instead of performing Bankart’s repair. Larger HillSachs injuries, consisting of more than 40% of posterosuperior corner defects, facilitate redislocation even at a little range
of external rotation. In those cases, reconstructions are necessary.
The rotational osteotomies had been advocated by AO
Group, but only for recurring instability(13). There is nothing
published for chronic dislocation.
Humeral head resections do not take place as first-line procedures, as arthroplasties had come to replace that deficiency.
Patients with older dislocations – six months or more – and
joint surface defects in excess of 40% form the best option for
arthroplasties, as the head becomes osteopenic and will flatten after reduction (ping-pong ball head)(1,2,3).
The prosthesis most important complication is the trend for
anterior dislocation. In those cases, a retroversion increase is
essential(10,11).
It is necessary to do a posterior glenoid lowering if there is
an important anterior glenoid wearing(2,3). Resected humeral
head bone can also be used as a graft to increase the anterior
glenoid. If the glenoid cartilage is in good condition, the hemiarthroplasty is associated by some experts to a capsule repair
similar to Bankart’s repair to increase joint stability(1).
Our opinion is that only a prosthetic version change along
with capsule tensioning is enough to provide adequate joint
stability.
If the subscapularis is torn, it should be mobilized and sutured. We do not have experience with calcaneal tendon grafts.
Despite complex joint reconstructions, sometimes results are
not satisfactory, and the patient may evolve with an important
loss of motion.
CHRONIC POSTERIOR DISLOCATION
McLaughlin defined that “the posterior dislocation is a trap
to the inattentive surgeon”, although its signs and symptoms
are constant and unequivocal(14).
Cooper stated that physical findings are so obvious that [it
consists of] “a lesion that shall not be confused”(8).
Neer and Hawkins reported a mean delay of one year for
the posterior dislocation diagnosis(14).
Elderly patients present more subtle symptoms, often with
diagnostic delay.
7
M.A. CASTRO VEADO
Somos da opinião de que somente uma alteração na versão
da prótese, juntamente com maior tensionamento capsular, é
suficiente para conferir boa estabilidade à articulação.
Se o subescapular está rompido, este deve ser mobilizado e
suturado. Não temos experiências com enxertos usando o tendão-de-aquiles. Apesar das complexas reconstruções articulares, os resultados nem sempre são bons, podendo o paciente
evoluir com perda importante dos movimentos.
LUXAÇÃO POSTERIOR CRÔNICA
Segundo Hawkins e Cash, McLaughlin considerava “a luxação posterior uma armadilha para o cirurgião distraído”,
embora os sinais e sintomas sejam constantes e inequívocos(14).
Segundo Matsen e Rockwood, Cooper afirmou que os achados físicos são tão óbvios, que “é uma lesão que não pode ser
confundida”(8).
Neer e Hawkins relataram atraso em média de um ano no
diagnóstico da luxação posterior (14).
Nos idosos os sintomas são mais sutis, atrasando freqüentemente o diagnóstico.
A incidência da luxação escapuloumeral posterior é estimada em 2%, mas provavelmente é muito maior, devido à
elevada ocorrência de casos não reconhecidos(8).
Rowe e Zarins, em 1982, relataram que o diagnóstico não
foi feito em 79% dos seus casos(6).
Essa lesão pode resultar de queda com a mão espalmada
com uma força aplicada sobre o ombro em flexão, adução e
rotação interna, ou após crise convulsiva, devido ao predomínio dos rotadores internos mais potentes.
Hipoglicemia noturna pode provocar convulsão sem que o
paciente perceba o que realmente aconteceu. Suspeitar sempre de luxação posterior crônica nos casos em tratamento prolongado de capsulite adesiva do ombro resistente ao tratamento
conservador (2).
Com o exame físico semiologicamente bem feito, a lesão
torna-se evidente pela perda ou ausência completa da rotação
interna (sinal importante para o diagnóstico), proeminência
do processo coracóide, enchimento posterior do ombro quando observado de cima ou de trás, mau alinhamento do braço
quando visto de lado. A elevação anterior e a rotação interna,
embora limitadas, às vezes surpreendem(14).
Rowe e Zarins descreveram um sinal físico típico: o paciente é incapaz de girar a palma da mão para cima com o
lado afetado(6) (fig. 6).
Radiografia feita somente em AP é a grande cilada, pois
freqüentemente é dada como normal, apesar de haver vários
sinais sugestivos de luxação, perda da sombra eliptiforme da
8
Fig. 6 – Sinal
de Carter Rowe:
incapacidade de
girar a palma da
mão para cima
(perda da
rotação externa).
Fig. 6 – Carter
Rowe sign:
inability to turn
the palm
towards the
ceiling (loss of
external
rotation).
The incidence of the posterior glenohumeral dislocation is
estimated around 2%, but it is probably much higher due to a
high number of unrecognized cases(8).
Rowe and Zarins in 1982 reported that the diagnosis was
not achieved in 79% of their cases(6).
This injury may result of a fall on the outstretched hand
with a force applied towards the shoulder in flexion, adduction, and internal rotation, or after seizures, due to the predominance of the more powerful internal rotators.
Nocturnal hypoglycemia may provoke seizures without the
patient’s perception of what really happened. There must always be a high suspicion degree of chronic posterior dislocation in those cases of protracted treatment of adhesive capsulitis that are resistant to conservative treatment(2).
A semiologically adequate physical examination unveils the
lesion for the evidence of complete internal rotation loss or
absence (an important diagnostic sign), coracoid process
prominence, posterior shoulder filling upon the observation
from above or from the back, and arm malalignment upon
lateral observation. Although limited, anterior elevation and
internal rotation are sometimes surprising(14).
Rowe described a typical physical sign: the patient is unable to turn his/her palm of the hand towards the ceiling with
the affected side(6) (figure 6).
Frequently considered as normal despite the presence of
several suggestive dislocation signs, such as an elliptical gleRev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
LUXAÇÃO INVETERADA DO OMBRO
Fig. 8
Tomografia
computadorizada
exibindo uma
luxação
posterior
associada à
fratura da
glenóide
Fig. 8
Computerized
tomography
showing a
posterior
dislocation
associated to
glenoid fracture
Fig. 7
Radiografia
em AP
sugerindo um
deslocamento
posterior da
cabeça umeral
Fig. 7 – AP X-ray
suggesting
a posterior
humeral head
displacement
glenóide, aumento do espaço entre a parte medial da cabeça
umeral e a borda anterior da glenóide, e o úmero em rotação
interna(14) (fig. 7).
A radiografia transaxilar é imperativa, não só para confirmar o diagnóstico, mas também para dar idéia do tamanho do
defeito ântero-medial da cabeça umeral (Hill-Sachs reverso)
e das fraturas da glenóide associadas. Na prática, é negligenciada com certa freqüência, seja por desconhecimento, incúria, ou mesmo pela dificuldade e receio que os técnicos têm
em posicionar adequadamente o braço.
A tomografia computadorizada é importante para melhor
definição do tamanho do defeito e para identificar lesões articulares associadas.
Tem sido relatado que, em torno de 50% das luxações posteriores, existe uma fratura do colo cirúrgico ou da escápula
associada(1) (fig. 8). Nas luxações anteriores esse quadro não
é tão comum. A presença dessas fraturas precisa ser conhecida antes que qualquer conduta seja tomada.
A
C
D
B
E
F
Fig. 9 – A) Em qual dos lados essa paciente foi operada? B) Radiografia em axilar do ombro esquerdo não operado (assintomático). C e D) Radiografia em AP e axilar do ombro direito com fratura-luxação posterior. E e F) Hemiartroplastia realizada dois meses
após a lesão.
TRATAMENTO
Fig. 9 – A) What side did this patient operate? B) Axillary view of
non-operated left shoulder (asymptomatic). C and D) Right shoulder AP and axillary X-rays showing posterior fracture-dislocation.
E and F) Hemiarthroplasty performed two months after the lesion.
Em muitas situações, um quadro radiológico alarmante
mostrando grande incongruência articular contrasta enormemente com o quadro clínico do paciente, que exibe amplitude
de movimentos bastante razoável e com pouca ou nenhuma
dor (fig. 9).
noid shadow, increase of space between the medial part of the
humeral head and the anterior glenoid rim, and humerus internal rotation, an isolated AP X-ray is grossly inaccurate(14)
(figure 7).
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
9
M.A. CASTRO VEADO
Em 1987, Hawkins et al publicaram sua experiência com
41 pacientes portadores de luxação posterior com seguimento de cinco anos e meio. Sete deles recusaram-se a receber
qualquer tipo de tratamento(15). Pacientes mais idosos com demanda limitada, capazes de alcançar a boca e com o ombro
contralateral funcionante, merecem ser observados. Não operamos também os com episódios de crise convulsiva não controlada ou os pouco cooperativos com o tratamento pós-operatório e de reabilitação. Reconstruções cirúrgicas devem ser
reservadas para os pacientes com bom estoque ósseo e grande
incapacidade funcional(1).
Redução fechada – Após quanto tempo da lesão estaremos autorizados a tentar a redução com segurança?
Não existe aqui também concordância entre os autores.
Segundo Matsen e Rockwood, Hawkins et al tentaram a redução em seus 12 pacientes com menos de seis semanas de
evolução e tiveram êxito em três(8). Schultz et al conseguiram a
redução em três dos 17 casos com menos de quatro semanas(4).
Acreditamos que, se a luxação tem menos que quatro semanas e defeito na cabeça umeral menor que 20%, a redução
incruenta pode ser tentada.
A tentativa de redução somente deve ser feita sob anestesia
geral, com bom relaxamento muscular, tração suave e sem
manobras tipo alavanca. Pode ser necessário relaxar o manguito posterior e a cápsula. Para isso, devemos rodar ao máximo o úmero internamente antes de tentar a redução, e associar tração lateral. Não rodar externamente antes de a redução
ser obtida, devido ao alto risco de fraturar a cabeça ou a diáfise umeral(8).
Conseguida, a redução, é necessário testar a estabilidade
da articulação, avaliando se a amplitude da rotação externa é
necessária para manter a cabeça reduzida. Em seguida, o membro superior envolvido é imobilizado em leve abdução e rotação externa de até 20° por período de seis semanas(1).
Se o tratamento incruento falhar, estará indicada a redução
aberta, após minuciosa análise do paciente no que se refere a
dor, perda de movimento, qualidade óssea e disponibilidade
para reabilitação.
Redução aberta – É executada com o paciente sob anestesia, na posição conhecida como “cadeira de praia”. Após acesso
pelo intervalo deltopeitoral, identificamos o cabo longo do
bíceps, para então localizarmos a pequena tuberosidade com
o tendão do subescapular inserido. Este pode ser liberado com
osteotomia da pequena tuberosidade ou sem ela(1,14,16).
A glenóide deve ser esvaziada do seu conteúdo fibrótico
antes da redução e inspecionada em busca de defeitos articulares.
10
The transaxillary X-ray is imperative not only to confirm
the diagnosis, but also to provide an idea about the humeral
head anteromedial defect size (reversed Hill-Sachs) and associated glenoid fractures. In practice, it is eventually neglected, either by lack of knowledge, negligence, or even due to
difficulty and fear that technicians have to adequately position the arm.
Computerized tomography is important for a better definition of defect size and to identify associated joint lesions.
It has been reported that around 50% of posterior dislocations carry an associated fracture of the surgical neck or scapula(1) (figure 8). Such picture is not so common in anterior
dislocations. The presence of those fractures must be recognized before taking any other steps.
TREATMENT
In many situations, an alarming radiological picture with
gross incongruity largely contrasts with the patient’s clinical
picture, who exhibits a quite reasonable range of motion and
little or no pain (figure 9).
In 1987, Hawkins et al published their series with 41 patients who presented a posterior dislocation, followed up for
5.5 years. Seven patients refused to receive any treatment
type(15). Older patients, with limited demands and able to reach
the mouth with the contralateral functioning shoulder, should
be observed. We do not operate patients with uncontrolled
seizures or those who may have low postoperative and rehabilitation compliance. Surgical reconstructions should be reserved for patients with adequate bone stock and severe functional impairment(1).
Closed reduction – How long after the injury are we entitled to attempt a safe reduction?
There is not an agreement among the authors. Hawkins et
al attempted a reduction for their 12 patients with less than
six weeks of evolution, and succeeded in three patients(8).
Schultz et al achieved reduction in three of 17 cases with less
than four weeks(4).
We believe that the closed reduction may be attempted if
the dislocation is less than four weeks old, with a humeral
head defect of less than 20%.
Reduction attempt must only be performed under general
anesthesia, with adequate muscle relaxation, gentle traction,
and with no lever-like maneuvers. It may be needed to relax
the posterior cuff and the capsule. For this purpose, we should
maximally internally rotate the humerus before reduction attempt, with lateral traction associated. Do not externally roRev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
LUXAÇÃO INVETERADA DO OMBRO
Fig. 10
Radiografia em
AP: cirurgia de
McLaughlin
modificada
por Neer.
Fig. 10
AP X-ray:
McLaughlin’s
procedure
modified
by Neer.
Tração é feita com a ajuda de um gancho, puxando-se a
diáfise umeral lateralmente antes de empurrar a cabeça por
meio de força aplicada de trás para diante em direção à glenóide.
Não alavancar o úmero na hora da redução, pois a cartilagem articular pode estar muito amolecida.
Em seguida, avaliamos o tamanho do defeito da cabeça
umeral. Se a articulação é instável e o defeito menor que 40%
da superfície articular, a melhor conduta é transferir o subescapular para o interior do defeito. Nos pacientes com boa qualidade óssea, optamos por osteotomizar a pequena tuberosidade e fixá-la com um ou dois parafusos maleolares associados
a uma arruela, para minimizar a possibilidade de fragmentação do osso (fig. 10). Nos mais idosos soltamos o subescapular com uma capa óssea, para apressar a consolidação e dar
mais segurança na fixação, a qual é feita com sutura não absorvível. Às vezes, utilizamos âncoras para a fixação do tendão do subescapular. Sempre cruentizamos o leito receptor
antes da fixação do tendão.
Se existir fratura associada, provavelmente a melhor opção
será a redução aberta com fixação da fratura.
A lesão da cápsula posterior ou pequenas fraturas da glenóide posterior raramente necessitam de tratamento além de
um simples desbridamento.
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
tate before reduction accomplishment due to the risk of humeral head or diaphyseal fracture(8).
The joint stability should be tested after reduction accomplished, assessing external rotation range, needed to keep the
head reduced. Then, the upper limb is immobilized in slight
abduction and external rotation of no more than 20° for a
period of six weeks(1).
If closed treatment fails, open reduction is indicated after
careful patient assessment of pain, loss of motion, bone stock,
and rehabilitation availability.
Open reduction – It is performed with the patient on a beach
chair position, under general anesthetic. After deltopectoral
approach, we identify biceps long head to locate the lesser
tubercle where the subscapularis tendon is inserted. It may be
released with or without a lesser tubercle osteotomy(1,14,16).
Glenoid scarring must be removed and inspected for joint
defects before reduction.
Traction is performed by a hook laterally pulling the humeral shaft before humeral head is pushed towards the glenoid with a back to front force.
Do not lever the humerus during reduction, as the joint
cartilage may be too soft.
The humeral head defect size is then assessed. If the joint is
unstable and the defect corresponds to less than 40% of joint
surface, the best treatment is to transfer the subscapularis
tendon to the inner part of the defect. In patients with adequate bone stock, our option is a lesser tubercle osteotomy
fixation with one or two malleolar screws with washers aiming to minimize the possibility of bone fragmentation (figure
10). In the elderly we release the subscapularis with a bone
coating to enhance healing and to provide a more secure fixation, performed with non-absorbable sutures. We sometimes
employ bone anchors for subscapularis tendon fixation, and
always leave a bleeding bone surface before tendon fixation.
If there is an associated fracture, probably the best option
is the open reduction and fracture fixation.
Posterior capsule lesions or posterior glenoid fracture seldom need other treatment then a simple debridement.
According to Loenberg and Cuomo, Keppler and Holz in
1994 advocated a humeral surgical neck rotational osteotomy and angled plate fixation only for those cases with less
than 40% of involvement of joint surface. Of ten patients, six
presented excellent and good results, two patients had reasonable results, and two patients had poor results(1). The advantage would be the absence of prolonged postoperative
immobilization, although adding a new bone aggression –
the osteotomy – which may pose an additional complication.
11
M.A. CASTRO VEADO
Segundo Loenberg e CuoA
mo, foram Keppler e Holz, em
1994, que preconizaram osteotomia rotacional no colo cirúrgico do úmero e fixação
com placa angulada, somente
nos casos com lesão menor
que 40% da superfície articular. Em 10 pacientes, seis tiveram excelentes e bons resultados, dois razoáveis e dois
pobres(1). A vantagem é a dispensa de imobilização prolongada no pós-operatório, emboB
ra acrescente nova agressão
óssea – osteotomia – que pode
ser fator adicional de complicação. Além do mais, a placa
exige maior desperiostização,
com maior risco de infecção e
retardo de consolidação ou
não consolidação.
Gerber e Lambert propõem,
nas lesões menores que 50%
e em ossos de boa qualidade,
o preenchimento da cavidade
com enxerto retirado da cabeça femoral e fixação por parafuso esponjoso(17). Seus resultados são semelhantes aos do
procedimento de McLaughlin
modificado por Neer, como relataram Gerber e Lambert(17).
Se o defeito é maior que
45% da superfície articular,
visto na radiografia transaxilar, com glenóide normal, a hemiartroplastia é a indicação de escolha da maioria dos cirurgiões(18).
Se a glenóide está comprometida, a artroplastia total é melhor opção.
O detalhe técnico fundamental é tirar a retroversão do componente umeral para diminuir a tendência da cabeça umeral
de deslocar-se posteriormente. Quanto mais tempo a cabeça
permanecer luxada posteriormente, menos retroversão deve
ser colocada(11,14,18).
Plicatura da cápsula posterior, após a osteotomia da cabeça
umeral e antes da inserção da prótese definitiva, pode ser ne12
Furthermore, the plate requires more periosteal stripping, a higher chance of infection, delayed union, and
nonunion.
Gerber and Lambert proposed cavity filling with femoral head graft and cancellous screw fixation in lesions
lesser than 50% and good
bone stock(17). Their results
are similar to McLaughlin’s
procedure modified by Neer,
Fig. 11
as reported by Gerber and
A) Tentativa
Lambert(14).
de redução
Most surgeons choose
cirúrgica de
uma luxação
hemiarthroplasty if the defect
posterior.
is in excess of 45% on the
B) Fixação
transaxillary view, with a
da grande
tuberosidade
normal glenoid. Upon glesem redução da
noid compromising, the best
luxação anterior.
option is the total arthroplasFig. 11
ty.
A) A surgical
reduction
The removal of humeral
attempt of a
component retroversion is an
posterior
essential technical detail to
dislocation.
lessen the humeral head
B) Greater
tubercle fixation
trend for posterior displacewithout anterior
ment. The longer the head
dislocation
remains posteriorly dislocatreduction.
ed, the lesser retroversion
should be placed(11,14,18).
A posterior capsule plication after humeral head osteotomy and before definite
prosthetic placement may be needed for final adjustments. It
is sometimes recommended to immobilize the upper limb in
slight abduction and external rotation to confer more stability and for plication protection(11).
Once the diagnosis is performed, the surgeon must be acquainted with the severity of the lesion, should know the surgical approach, and ought to have adequate surgical team
and material if he or she decides to operate an unreduced
dislocation. True catastrophes may arise when the surgeon is
not fully acquainted with such lesion (figure 11).
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
LUXAÇÃO INVETERADA DO OMBRO
cessária para os ajustes finais. Às vezes, é recomendado imobilizar o membro em leve abdução e rotação externa para dar
mais estabilidade e proteger a plicatura(11).
Uma vez feito o diagnóstico, o cirurgião que se propõe a
operar uma luxação inveterada deve estar ciente da gravidade
dessas lesões, conhecer a abordagem cirúrgica e ter equipe e
material cirúrgico adequados.
Verdadeiras catástrofes podem acontecer quando o cirurgião tem pouca intimidade com esse tipo de lesão (fig. 11).
REFERÊNCIAS / REFERENCES
1. Loebenberg M.I., Cuomo F.: The treatment of chronic anterior and posterior dislocations of the glenohumeral joint and associated articular surface
defects. Orthop Clin North Am 31: 23-34, 2000.
2. Deliz E.D., Flatow E.L.: “Chronic unreduced shoulder dislocations”. In:
Bigliani L.U.: Complications of shoulder surgery. Maryland, Williams and
Wilkins, p. 127-138, 1993.
3. Flatow E.L., Miller S.R., Neer C.S.: Chronic anterior dislocation of the shoulder. J Shoulder Elbow Surg 2: 2-10, 1993.
4. Schultz T., Jacobs B., Patterson R.L.: Unrecognized dislocations of the shoulder. J Trauma 9: 1009-1023, 1969.
5. Postacchini F., Facchini M.: The treatment of unreduced dislocation of the
shoulder. A review of 12 cases. J Orthop Traumatol 13: 15-26, 1987.
6. Rowe C., Zarins B.: Chronic unreduced dislocations of the shoulder. J Bone
Joint Surg [Am] 64: 494-505, 1982.
7. Buhler M., Gerber C.: Shoulder instability related to epileptic seizures. J
Shoulder Elbow Surg 11: 339-343, 2002.
8. Matsen F.A., Rockwood C.A.: “Anterior glenohumeral instability”. In:
Roockwood C.A., Matsen F.A.: The shoulder. Philadelphia, W.B. Saunders,
p. 671-672, 1990.
9. Lech O: Fundamentos em Cirurgia do Ombro. São Paulo, Harbra, 100,
1995.
Rev Bras Ortop _ Vol. 39, Nos 1/2 – Jan/Fev, 2004
10. Pritchett J.W., Clark J.M.: Prosthetic replacement for chronic unreduced
dislocations of the shoulder. Clin Orthop 216: 89-93, 1987.
11. Zuckerman J.D.: McLaughlin Procedure for Acute and Chronic Posterior
Dislocations in Master Techniques in Orthopaedics Surgery. The Shoulder.
Craig EV. New York, Raven Press, p. 165-180, 1995.
12. Neviaser J.S.: The treatment of old unreduced dislocations of the shoulder.
Surg Clin North Am 43:1671-1678, 1963.
13. Weber B.G., Simpson L.A., Hardegger F.: Rotational osteotomy for the recurrent anterior dislocation of the shoulder associated with a large Hill-Sachs lesion. J Bone Joint Surg [Am] 66: 1443-1449, 1984.
14. Hawkins R.J., Cash J.D.: “Complications of posterior instability repairs”.
In: Bigliani L.U.: Complications of shoulder surgery. Maryland, Williams
and Wilkins, p. 117-126, 1993.
15. Hawkins R.J., Neer C.S., Pianta R.M., et al: Locked posterior dislocation of
the shoulder. J Bone Joint Surg [Am] 69: 9-18, 1987.
16. Mestdagh H., Maynou C., et al: Traumatic posterior dislocation of the shoulder in adults. Ann Chir 48: 355-363, 1994.
17. Gerber C., Lambert S.M.: Allograft reconstruction of segmental defects in
humeral head for the treatment of chronic locked posterior dislocation of
the shoulder. J Bone Joint Surg [Am] 78: 376-382, 1996.
18. Walch R., Boileau P., Martin B., Dejour H.: Unreduced posterior luxations
and fractures-luxations of the shoulder. Rev Chir Orthop 76: 546-558, 1990.
13