UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE POS GRADUAÇÃO EM CIÊNCIAS DA SAÚDE
CARACTERIZAÇÃO DO PERFIL IMUNOLÓGICO EM MULHERES
PORTADORAS DO PAPILOMAVÍRUS HUMANO
Daliana Caldas Pessoa da Silva
Natal
2011 . 2
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE POS GRADUAÇÃO EM CIÊNCIAS DA SAÚDE
CARACTERIZAÇÃO DO PERFIL IMUNOLÓGICO EM MULHERES
PORTADORAS DO PAPILOMAVÍRUS HUMANO
Dissertação de mestrado
apresentada ao programa de
pós graduação em ciências
da Saúde da Universidade
Federal do Rio Grande do
Norte
Para obtenção do título de
grau mestre.
Orientador: Prof. Dr. Geraldo Barroso Cavalcanti Junior (UFRN)
Co-orientadora: Profa. Dra. Ane Katerine Gonçalves (UFRN)
Natal
2011 . 2
II
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE POS GRADUAÇÃO EM CIÊNCIAS DA SAÚDE
Coordenadora: Profa. Dra. Tércia Maria de Oliveira Maranhão
Natal
2011 . 2
III
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
PROGRAMA DE POS GRADUAÇÃO EM CIÊNCIAS DA SAÚDE
CARACTERIZAÇÃO DO PERFIL IMUNOLÓGICO EM MULHERES
PORTADORAS DO PAPILOMAVÍRUS HUMANO
Banca Examinadora:
Presidente da Banca: Geraldo Barroso Cavalcanti Junior
Membros da Banca Examinadora:
Prof. Dr. Geraldo Barroso Cavalcanti Junior – UFRN
Prof. Dr. Carlos Eduardo de Queiroz Lima – UFPE
Profa. Dra. Valéria Soraya de Farias Sales - UFRN
Natal
2011 . 2
IV
“ Se pensar é o destino o ser humano, continuar
sonhando
lógico,
é
o
implica
seu
em
grande
desafio.
trajetórias
vitórias,
com
muitas
obstáculos
pelo
caminho.
lutas,
Apesar
com
e
de
E
isto,
riscos,
não
é
em
poucos
tudo,
seja
ousado. Liberte sua criatividade. E NUNCA DESISTA
DOS SEUS SONHOS, pois eles transformarão sua vida
em uma grande aventura”
Augusto Cury
V
DEDICATÓRIA
Aos meus pais e avó, Dailor Bezerra Pessoa, Maria de Fátima Caldas
Pessoa e Izabel Fernandes Caldas, grandiosos mestres, conselheiros e
educadores, pelos fiéis exemplos de vida, amor, dedicação e perseverança.
Agradeço de coração o carinho, incentivo e apoio constantes, que nunca
mediram esforços para me fazer seguir em frente na busca de meus sonhos.
A minha filha, Isabelle Caldas Pessoa da Silva, que através de seu
amor e carinho em todas as horas, me incentivou a prosseguir.
A meu namorado, Jakson Rogério Ferreira de Lima, que através de
sua dedicação e compreensão fazem dele um verdadeiro companheiro em
todos os momentos.
VI
AGRADECIMENTO
À Deus, pelo dom da vida e por sempre me iluminar e guiar meus
caminhos.
Ao Prof. Geraldo Barroso Cavalcanti Junior, que através de sua
amizade, confiança e orientação foi fundamental tanto no meu conhecimento
científico
profissional como
pessoal.
Obrigada
eternamente,
professor
Geraldo!!!! Sempre levarei comigo seu exemplo de vida, ética, humildade e
solidariedade.
À Prof. Janaina Crispim Freitas, pela amizade, atenção e assessoria
científica constante. A sua presença foi extremamente importante ao meu
amadurecimento científico. Gratidão eterna, querida professora, ao seu
incentivo e apoio que nunca me faltaram desde o início do nosso encontro.
À Prof. Ana Katherine da Silveira Gonçalves, pela atenção,
colaboração e auxílio científico.
Àos amigos Rosana Lucena de Sá Leitão, Roberto Chaves de
Vasconcelos pela atenção e colaboração. Ainda por disponibilizar o laboratório
de citometria de fluxo do Hemonort, para realização da imunofenotipagem das
pacientes.
Ao colega José Queiroz Filho, não apenas pela colaboração científica,
mas principalmente pelo valor da eterna amizade, companheirismo e apoio nas
dificuldades e alegrias.
A amigo graduando Diego, pela amizade e excelente auxilio técnico.
As funcionárias do laboratório Potengi, pela amizade, colaboração e
extrema atenção em todos os momentos.
VII
LISTA DE ABREVIATURAS
APCs:
Células Apresentadoras de Antígenos
DCs:
Células Dendríticas
HMC:
Complexo de Histocompatibilidade
HPV:
Papiloma vírus Humano
ISTs:
Infecção Sexualmente Transmissíveis
LGG:
Linfócitos Grandes Granulados
LIE:
Linfócitos intra epiteliais
LSIL:
Lesão Intraepitelial Cervical de Baixo Grau
NK:
Natural Killer
NKT:
RPM:
Rotação Por Minuto
TH:
T. Helper
ZN:
Zona de Transformação
VIII
LISTA DE FIGURAS
Representação esquemática do genoma do HPV: E
FIGURA 01
(Early do inglês) são genes precoces, L (Late do inglês)
são genes tardios e URR (upstream Region Regulation)
03
é a região reguladora da replicação viral.
Replicação do HPV relacionada à diferenciação das
FIGURA 02
células do epitélio escamoso estratificado da cérvice
uterina mostrando um epitélio cervical normal e um
08
infectado pelo vírus HPV
FIGURA 03
FIGURA 04
FIGURA 05
FIGURA 06
FIGURA 07
FIGURA 08
FIGURA 09
FIGURA 10
FIGURA 11
FIGURA 12
FIGURA 13
Células escamosas com características coilocíticas
Representação esquemática do perfil imunológico por
cintometria de fluxo de uma paciente com lesão
induzida por HPV.
Representação esquemática do perfil imunológico por
cintometria de fluxo de uma paciente do grupo controle.
Distribuição da leucometria em mulheres HPV+ e HPV-.
Distribuição da contagem de linfócitos em mulheres
HPV+ e HPV-.
Distribuição da contagem de monócitos em mulheres
HPV+ e HPVDistribuição da contagem de granulócitos em mulheres
HPV+ e HPV-.
Distribuição dos valores de linfócitos TCD3+ em
mulheres HPV+ e HPV-.
Distribuição dos valores de linfócitos BCD19+ em
mulheres HPV+ e HPV-.
Distribuição dos valores de linfócitos TCD4+ em
mulheres HPV+ e HPV-.
Distribuição dos valores de linfócitos TCD8+ em
mulheres HPV+ e HPV-.
13
17
18
31
32
33
34
35
36
37
38
IX
FIGURA 14
FIGURA 15
FIGURA 16
Distribuição da relação CD4/CD8 em mulheres HPV+ e
HPV-.
Distribuição dos valores de células NK (CD16-56+) em
mulheres HPV+ e HPV-.
Distribuição dos valores de células NKT (CD3+/CD1656+) em mulheres HPV+ e HPV.
39
40
41
X
LISTA DE TABELAS
TABELA 01
Valores de referência da sub-população linfocitária.
16
TABELA 02
Características gerais e parâmetros hematológicos
das mulheres pertencentes ao grupo controle.
23
TABELA 03
Características gerais e parâmetros hematológicos
das mulheres infectadas pelo HPV
24
TABELA 04
Porcentagem de pacientes portadoras de HPV de
alto risco e de baixo risco oncongênico.
25
TABELA 05
Parâmetros clínicos e epidemiológicos de 30
pacientes com LSIL estratificada por idade, tipo de
lesão, presença oncogênico de baixo grau
(destaque em verde) e alto risco (destaque em
vermelho) do HPV e perfil imunológico.
26
TABELA 06
Perfil imunológico das mulheres pertencentes ao
grupo controle
29
TABELA 07
Perfil imunológico das mulheres infectadas pelo HPV
30
XI
LISTA DE ANEXOS
Anexo 01
...................................................................................
55
XII
SUMÁRIO
1
LISTA DE ABREVIATURAS
VIII
LISTA DE FIGURAS
IX
LISTA DE TABELAS
XI
LISTA DE ANEXOS
XII
SUMÁRIO
XIII
RESUMO
XV
INTRODUÇÃO
1.1
2
4
CÂNCER DE COLO UTERINO
1
REVISÃO DA LITERATURA
3
2.1
BIOLOGIA E CARACTERIZAÇÃO DO HPV
3
2.2
TÉCNICAS DE DETECÇÃO DO HPV
4
2.3
3
1
O HPV E A INTERFERÊNCIA NO SISTEMA IMUNOLÓGICO DO
HOSPEDEIRO
5
9
OBJETIVOS
3.1
OBJETIVO GERAL
9
3.2
OBJETIVO ESPECÍFICO
9
10
CASUÍSTICA E METODOLOGIA
4.1
CARACTERIZAÇÃO DA PESQUISA
10
4.2
PARTICIPANTES
10
4.3
CRITÉRIO DE EXCLUSÃO
10
4.4
MATERIAL
11
XIII
4.4.1
4.5
AMOSTRAS BIOLÓGICAS
PROCEDIMENTOS
4.5.1
4.5.2
5
12
UTILIZANDO A COLORAÇÃO DE PAPANICOLAOU
METODOLOGIA DA CITOMETRIA DE FLUXO NO
14
ESTUDO DO PERFIL IMUNOLÓGICO
4.5.2.2
4.5.3
11
METODOLOGIA DA CITOLOGIA ONCÓTICA
4.5.2.1
4.6
11
ANÁLISE HEMATOLÓGICA DE PACIENTES E
GRUPO CONTROLE
ANÁLISE DE CITOMETRIA DE FLUXO DE
14
PERFIL IMUNOLÓGICO
METODOLOGIA DA CAPTURA HÍBRIDA
19
ANÁLISE ESTATÍSTICA
19
21
RESULTADOS
5.1
5.2
5.3
14
CARACTERÍSTICAS GERAIS E PARÂMETROS
21
HEMATOLÓGICOS DA POPULAÇÃO INVESTIGADA.
DETECÇÃO DO PAPILOMAVÍRUS HUMANO EM AMOSTRAS DE
CITOLOGIA CERVICAL
INVESTIGAÇÃO DOS PARÂMETROS IMUNOLÓGICOS DA
25
27
POPULAÇÃO ANALISADA
6
DISCUSSÃO
42
7
CONCLUSÃO
46
8
REFERÊNCIAS BIBLIOGRÁFICAS
47
9
ABSTRACT
54
10
ANEXO
55
XIV
Resumo
O câncer de colo uterino consiste em um problema de grande relevância
social, visto que se trata da segunda malignidade ginecológica mais freqüente
no mundo. O principal precursor do câncer da cérvice uterina consiste na
infecção pelo Papiloma vírus humano (HPV). O HPV tem despertado grande
interesse na comunidade científica, devido à relação estabelecida entre a sua
epidemiologia e o câncer de cérvice uterina. Apesar do grande avanço na
biologia do HPV, pouco se sabe acerca da resposta imunológica a este vírus. O
Papilomavírus humano (HPV) é um DNA vírus epiteliotrófico, que está
vinculado à carcinogênese do colo uterino por meio de evidências
epidemiológicas e laboratoriais. As infecções pelo HPV ocorrem em mulheres
em todo o mundo. Existe consenso na literatura quanto à associação do DNA –
HPV com as neoplasias intra – epiteliais cervicais e o câncer cervical. Por este
motivo é de grande importância a detecção precoce deste tipo de infecção para
que seja efetuado um tratamento específico. Esse trabalho está caracterizando
o perfil imunológico de pacientes portadoras de HPV através da quantificação
linfocitária (TCD4, TCD8, células NKT e células NK), e correlacionou esse
material à técnica de captura híbrida, para poder comprovar a infecção pelo
HPV, esperando assim contribuir precocemente para o diagnóstico do câncer
de colo uterino.
Descritores: Papilomavírus humano, Perfil imunológico captura hibida
XV
1.INTRODUÇÃO
1.1– CÂNCER DE COLO UTERINO
O câncer cervical é a segunda neoplasia mais prevalente entre mulheres
no Brasil e no mundo(KODON K., 2009). Dados estimam que 231.000 mortes
anualmente desta doença e cerca de 80% delas são oriundas dos países em
desenvolvimento (BOSCH, FXAN, et al., 2008;BRASIL mds, 2008).
A infecção persistente pelo Papiloma vírus Humano (HPV), do tipo
oncogênico desempenha papel preponderante no desenvolvimento do câncer
do colo uterino, sendo esse vírus detectado em quase todas as lesões pré –
malignas e neoplásicas cervicais. (REIMERS et al., 2009; WOLSCHICK et al,
2011).
Além da infecção pelo HPV, existem também outros fatores de risco
envolvidos na carcinogênese cervical tais como: baixo nível sócio-econômico,
início precoce da atividade sexual, multiplicidade de parceiros sexuais,
tabagismo, higiene íntima inadequada, uso prolongado de contraceptivos orais,
doenças sexualmente transmissíveis (DST) e imunossupressão (AU, 2004;
BOARDMAN, COOPER et al., 2004; FRANCESCHI, 2005; TRIMBLE,
GENKINGER et al, 2005; WANG et al.,2009).
A carcinogênese cervical é um processo que se desenvolve em múltiplas
etapas (MUNOZ et al, 2003; MOSCICKI et al, 2006). A infecção persistente por
um ou mais tipos de Papillomavírus humano (HPV) oncogênico e a
transformação do epitélio infectado em neoplásico constituem em uma das
etapas mais importantes desse processo (MOSCICKI et al, 2006).
Embora estas etapas já estejam bem estabelecidas, diversos estudos
relacionam os fatores imunológicos como determinantes destas transições
(MUNOZ et al, 2003; AGUILAR et al, 2006; CASTLE et al, 2006).
XVI
A capacidade do indivíduo de eliminar a infecção pelo HPV seria
determinada por fatores genéticos, possivelmente, atuando através de
mecanismos imunológicos (GHADERI et al., 2002).
A resposta imune do hospedeiro é considerada hoje um fator
determinante da carcinogênese cervical, portanto a elucidação do perfil
imunológico desencadeada no organismo pelo HPV e relacionada ao tipo de
resposta imune provocada pela células T e sub-populações T helper (CD3+⁄
CD4+), supressor citotóxico (CD3+⁄ CD8+) e células natural Killer (NK), pode
contribuir para o monitoramento das pacientes com lesão intra epitelial cervical
O surgimento de novos parâmetros de avaliação para infecção por HPV
é de grande relevância científica, visto a grande incidência deste vírus e a
morbidade ocasionada por este em mulheres no mundo inteiro. Dada à
importância deste estudo, podemos ressaltar que a sua aplicabilidade irá
culminar com um novo consenso para o diagnóstico das lesões intra-epiteliais
cervicais na profilaxia do câncer de colo uterino.
XVII
1.1.1.1.1.1 2. REVISÃO DA LITERATURA
2.1 – BIOLOGIA E CARACTERIZAÇÃO DO HPV
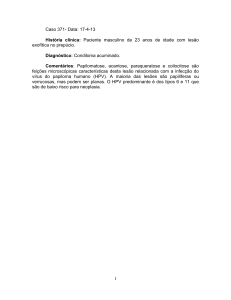
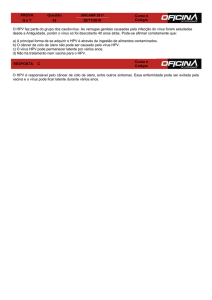
O Papilomavírus Humano (HPV) é um vírus de dupla fita circular de DNA
(figura 01) com comprimento de 7900 Kilobases de forma icosaédrica, não
envelopado, com 72 caspsômeros e pertence à família Papillomaviridae. O
HPV é classificado conforme a espécie de hospedeiro natural e subclassificado
em tipos de acordo com as seqüências de nucleotídeos de DNA (ICTV, 2003;
BURT, 2003).
Após a integração dos HPVs de alto risco no genoma celular, esses
passam a codificar as oncoproteínas E6 e E7 que promovem o processo
maligno. A célula hospedeira possui genes supressores de tumores pRb e p53.
O gene Rb é o principal regulador do ciclo celular e o gene (p53) é chamado
de “guardião do genoma”, pois tem finalidade de supervisionar se todos os
genes estão íntegros.
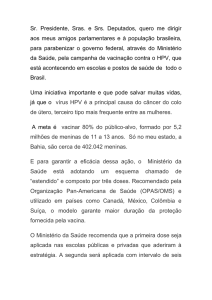
Figura 1 - Representação esquemática do genoma do HPV: E (Early do inglês) são genes
precoces, L (Late do inglês) são genes tardios e URR (upstream Region Regulation) é a região
reguladora da replicação viral (adaptado de Munoz et al.,2006)
XVIII
Os HPVs dos tipos 6 e 11 induzem a condilomas que afetam a pele
anogenital e parte inferior da vagina, sendo detectado nas lesões intraepiteliais
escamosa de baixo grau (LSIL) e são considerados de baixo risco porque estão
envolvidas em lesões benignas. Os HPVs dos tipos 16, 18, 30, 31, 33, 34, 35,
45, 51, 52, 56, 58, 59, 66, 68 e 70 são fortemente associados com câncer intra
– epitelial cervical, sendo considerados de alto risco e prevalecem em cânceres
anogenitais (GOMPEL, 1997; PINHO et al.,2003; VARGAS et al.,2004).
2.2 – TÉCNICAS DE IDENTIFICAÇÃO DO HPV
Para determinação do câncer de colo de útero, o uso das técnicas
atuais, como teste citopalógico, apesar de serem confiáveis, apresentam
baixos índices de reprodutibilidade. Os testes moleculares, quando apresentam
resultados positivos para tipos virais altamente oncogênicos, não determinam
necessariamente o desenvolvimento de uma displasia, sendo necessários
vários outros fatores concomitantes. Portanto, novas técnicas citológicas de
análises prediletivas, confiáveis e reprodutíveis devem ser admitidas(MADKAN
et al., 2007).
A utilização da técnica de captura híbrida como metodologia no
diagnóstico molecular do Papilomavírus Humano (HPV) tem se mostrado como
uma das mais sensíveis na identificação do DNA viral existente nos mais
diversos materiais clínicos (MANOS et al.,1989; BAUER et al.,1991; ADAMS et
al., 1996, IWASAWA et al.,1997; GRAVITT et al.,1998; CHOW et al., 2000;
NELSON et al., 2000; RÒLON et al., 2000), bem como na resolução de dúvidas
originadas durante o diagnóstico citopalógico, não apenas nas infecções pré
maligna , mas também nas infecções latentes ou subclínicas associadas a esse
agente viral (MANOS et al.,1989; ADAMS et al.,1996; HIETANEN et al.,1997;
COX, 1999; TENTI et al.,1999; CUZICK, 2000; VILLA, 2000; WRIGHT et al.,
2000).
XIX
A Detecção do DNA do HPV pela técnica de captura hibrida é
importante, mas se torna imperativo discriminar o tipo de HPV presente em
materiais clínicos provenientes das mucosas genitais, a fim de verificar se os
tipos presentes são de alto ou baixo potencial para desenvolvimento de
neoplasias cervicais (BERNARD et al., 1994; VILLA, 2000).
A determinação do tipo de HPV pode auxiliar também na condução de
um tratamento mais apropriado para pacientes acometidas por essa infecção
viral.
2.3 – O HPV E A INTERFERÊNCIA NO SISTEMA IMUNOLÓGICO DO
HOSPEDEIRO
O sistema imunológico da mucosa vaginal é formado pelos tecidos
linfóides que estão associados à superfícies da mucosa vaginal. Agregados de
tecidos linfóides não encapsulados são encontrados particularmente na lâmina
própria tecidual, e na lâmina submersa do trato geniturinário (ROITT, 2003).
A
mucosa
geniturinária
contém
células
dendríticas
para
a
internalização, processamento e transporte de antígenos para os linfonodos
drenantes (ROITT, 2003).
A resposta imune da vagina, tanto celular quanto humoral, parece
depender da ação hormonal. Como o epitélio endometrial, a vagina também se
modifica nas diferentes fases do ciclo menstrual, no entanto, mais
acentuadamente à ação de estrógenos e progesterona. Os hormônios parecem
que atuam de forma contrária aos mecanismos de defesa local. Estudos
demonstram claramente que tanto o estrógeno e a progesterona influenciam na
resposta imune inata e adaptativa. Evidências destes efeitos são encontradas
em estudos experimental realizados entre fêmeas e machos (FIDLER, 2003;
BETTINI et al., 2003).
XX
Existem vários tipos de linfócitos, porém não se consegue fazer
diferenciação entre eles pela microscopia óptica convencional. Sendo somente
a sua diferenciação por métodos imunológicos tais como: imunohistoquímica e⁄
ou imunofluorescência, detectado por meio de anticorpos monoclonais os
antígenos são capazes de caracterizar estas células
A maioria dos linfócitos circulantes são do tipo T, e uma menor
quantidade do tipo B e “Natural Killer (NK)”. Os linfócitos T possuem receptores
especializados em reconhecer antígenos ligados a MHC na superfície de
outras células, que pode ser do tipo alfa/beta (TCR α ⁄ β) ou gama/delta (TCR γ
⁄ ∆). Na circulação sangüínea, ocorre o predomínio de células T com TCR α ⁄ β
e na mucosa vaginal com TCR γ ⁄ ∆. Existe a hipótese de que os linfócitos T
TCR γ ⁄ ∆ desempenhem função primordial na proteção das superfícies das
mucosas (FIDLER, 2003; ROITT, 2003).
Funcionalmente os linfócitos T são classificados em: linfócitos T
auxiliares, T supressores citotóxicos. Os linfócitos T auxiliares também
chamados T helper (Th), possuem receptor CD4 que reconhece a molécula do
complexo principal de histocompatibilidade classe II, atuam no reconhecimento
de macrófagos ativados e são importantes “sinalizadores” através da produção
de interleucinas, que interagem com outros tipos celulares. De acordo com as
citocinas produzidas desenvolve-se uma resposta predominantemente celular
(tipo Th1). Com o direcionamento de mais células da resposta imune inata e
linfócitos T para o local da infecção, ou uma resposta predominantemente
humoral (tipo Th2), induzindo o recrutamento de linfócitos B e produção de
imunoglobulinas (ROITT, 2003; ABBAS 2008).
Os linfócitos T citotóxicos possuem receptores CD8 e são capazes de
reconhecer e tolerar as moléculas de MHC de classe I autologa presente na
superfície de outras células nucleadas e conseqüentemente exercer a ação de
citotoxidade contra moléculas quando associadas a partículas virais ou se as
mesmas forem geneticamente de outra origem (ABBAS, 2008).
Outra população de linfócitos são os linfócitos denominados de
linfócitos grandes granulares ou LGL, do termo em inglês “Large Grand
XXI
Lymphocyte”. Estes linfócitos se caracterizam por apresentarem em seu
citoplasma um abundante conteúdo de grandes grânulos de tonalidade violeta
(grânulos azurófilos), quando corados por corantes hematológicos ( ABBAS
2008). Esses linfócitos são classicamente denominados de “células assassinas
naturais” ou Natural Killer (NK) sendo do ponto de vista imunofenotípico
idenficados por técnicas de imunofenotipagem pela expressão do antígeno CD
56, expressando também altos níveis de controle (FC) receptor para fração das
imunoglobulinas (CD 16) ou ainda as enzimas granzimas e perfurinas que
estão presentes nos grânulos acima citados (ROITT, 2003).
Cerca de 60 a 65% dos linfócitos circulantes nos adultos sadios
correspondem a linfócitos T total. Destes, cerca de 35 a 50% correspondem as
células TCD4+ e 25 a 30% as células TCD8+. As células NK correspondem a
uma contagem em torno de 10 a 15% e os linfócitos B em torno de 10 a 20%.
(LANIER, 1997).
As células NK usualmente lisam células alvo que não expressam
moléculas MHC de classe I, tais como, células tumorais ou aquelas infectadas
por vírus. Dessa forma, moléculas MHC clássicas de classe I, quando
expressas na superfície das células nucleadas podem exercer um mecanismo
protetor da lise mediada por células NK nas células saudáveis (BONTROP,
2000).
A região MHC de classe II possui genes que codificam as moléculas
clássicas de histocompatibilidade de classe II, expressas normalmente nas
células apresentadoras de antígenos (APCs), ou seja, nos monócitos,
macrófagos, células dendríticas, células de Langerhans e linfócitos B
(SULLIVAN et al., 2006). Do ponto de vista funcional, essas moléculas estão
envolvidas na apresentação de peptídeos de origem extracelular, tais como
bactérias, para células TCD4+ (TABAYOYONG et al., 2007). A ativação dessas
células libera citocinas que atuam em diversas reações imunes (KELLY et al.,
1991; SLOAN CAMERON et al., 1995).
Uma vez que a infecção pelo HPV apresenta natureza não-lítica, limita
a produção de antígenos virais que são processados e apresentados ao
sistema imune adaptativo. As proteínas codificadas pelo vírus, em sua maioria,
não são secretadas através das células infectadas. Portanto, as proteínas E
XXII
(precoces) são expressas em níveis baixos e, sobretudo, no núcleo celular e a
produção de proteínas do capsídeo viral, altamente imunogênicas, é limitada a
camada mais diferenciada e liberada ao epitélio, onde os sinais próinflamatórios são diminuídos. O HPV apresenta um perfil insuficiente para
ativar a resposta imune do hospedeiro, uma vez que não há fase do ciclo de
vida do HPV na corrente sanguínea, e apenas quantidades mínimas de
replicação do vírus são expostas ao sistema imune, o vírus se torna
praticamente imperceptível para o sistema imune do hospedeiro (KANODIA et
al., 2007; STANLEY, 2008). Embora a resposta imune a infecção ao HPV seja
pouco entendida, postula-se que a resposta imune celular (Th1) é prioritária em
relação à resposta imune humoral (Th2). Ainda, a resposta imune do tipo Th1
pode gerar resposta específica dos linfócitos T citotóxicos, contribuindo para
eliminação da infecção e regressão das lesões infectadas pelos tipos de HPV
de baixo risco (GONÇALVES, 2004).
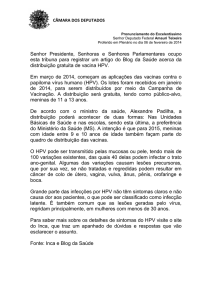
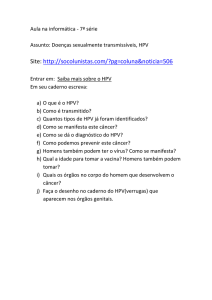
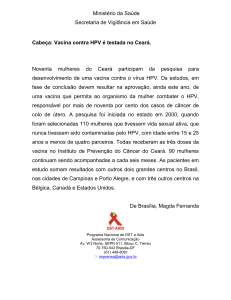
Figura 2 - Replicação do HPV relacionada à diferenciação das células do epitélio escamoso
estratificado da cérvice uterina mostrando um epitélio cervical normal e um infectado pelo vírus
HPV (Adaptado de MUÑOZ et al., 2006).
XXIII
3.0 – OBJETIVOS
3.1 - Geral:
Avaliar o perfil imunológico de mulheres portadoras do Papiloma Vírus
Humano (HPV) por meio do perfil leucocitário, contagem de monócitos,
granulócitos além de linfócitos total e subpopulações: i) Linfócitos B (LB), ii)
Linfócitos T (LT) e subpopulações LT Helper e LT Supressor Citotóxico e, iv)
células natural killer (NK).
3.2 - Específicos:
•
Avaliar o efeito citopatologico compatível com HPV nas mulheres em
estudo através da citologia oncótica.
•
Tipificar os HPVs (em alto ou baixo grau) pela técnica de captura
híbrida em mulheres cuja citologia cervico-vaginal apresentaram alterações
citopatológicas compatíveis com HPV.
•
Comparar o perfil leucocitário e imunológico das mulheres com lesão
cervical Intraepitelial cervical de baixo risco e com HPV de alto risco oncológico
e com mulheres com HPV de baixo risco oncológico, associando também
pacientes não portadoras de HPV.
XXIV
4 – DELINEAMENTO DO ESTUDO
4.1 – Caracterização da pesquisa:
O presente estudo foi conduzido mediante a aprovação do comitê de
ética da Universidade Federal do Rio Grande do Norte. Este trabalho foi
realizado por um estudo prospectivo, realizando inicialmente teste de captura
híbrida nas mulheres com histórico de lesão cérvico-vaginal recorrente e
estudo de perfil imunológico neste grupo de pacientes e em mulheres sadias
que serviram como grupo controle.
4.2 – Participantes:
Esse estudo foi realizado com um grupo de 30 pacientes na faixa etária
dos 18 aos 59 anos, cuja citologia oncótica cérvico vaginal apresentou efeito
citopático para HPV e foram não reagentes para o teste de HIV, HVC e HbsAg,
provenientes do serviço de citologia do laboratório Potengi.
O grupo controle foi composto de 30 pacientes saudáveis não
portadoras de lesão cervico vaginal e sem HPV.
4.3 – Critérios de exclusão:
- Tabagistas
- Pacientes fora do grupo etário escolhido;
- Pacientes gestantes;
- Pacientes submetidos a qualquer tipo de tratamento ginecológico;
XXV
- pacientes com qualquer tipo de doenças do sistema imunológico:
imunodeficiências, doenças inflamatórias e auto-imunes.
4.4 – Material:
4.4.1- Amostras biológicas
a- Sangue periférico:
Amostras de sangue periférico (10 mL) foram obtidas através de
punção de venosa, foram, coletadas por sistema a vácuo vacutainer (BECTON
– DICKINSON – VACUTAINER SST BD). Tubos contendo anticoagulante, para
a realização dos seguintes exames; hemograma e quantificação da subpopulação linfocitária por citometria de fluxo.
Paralelamente a esses exames, todas as pacientes foram submetidas
à testes sorológicos para Fator Reumatóide, HIV, HTLV, HVC e HbsAg, sendo
todas soronegativas.
b- Raspado cérvico-vaginal:
Raspado das paredes vaginais, ecto e endocervice foram colocados
em lâminas de vidro previamente identificadas, fixadas em álcool 96% para
posterior coloração e leitura, com a finalidade de identificar a presença de
coilócitos e discariose que são efeitos citopático para o vírus HPV. Parte das
células escamosas foram acondicionadas em frasco contendo 1,5 mL de
solução tampão t.E (Tris-HCL 10 mM pH 8,0; EDTA 1 mM) e estocadas a – 20º
para ser utilizada a técnica de captura híbrida, onde foi identificado se o HPV
era de alto ou de baixo risco oncogênico. Realizado no laboratório Alvaro.
4.5 – Procedimentos:
XXVI
4.5.1 – Metodologia da citologia oncótica utilizando a coloração de
Papanicolaou:
As Pacientes foram encaminhadas para o setor de anamnese, onde foi
preenchida sua ficha, em seguida foi coletado material cervico vaginal das
mesmas utilizando espátulas de Ayre e escova vaginal e confeccionado os
esfregaços em duas lâminas sendo estas fixadas em álcool absoluto e em
seguida foram coradas pela técnica de Papanicolaou, onde se analisou estas
lâminas e observou a presença de coilócitos ou não, que caracteriza o efeito
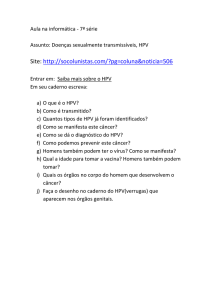
citopático compatível com HPV. Fig. 03.
XXVII
A
B
C
D
E
F
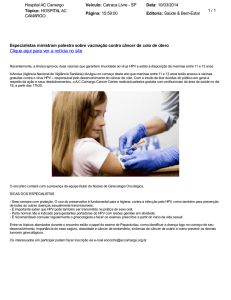
Figura 03 - Células escamosas com características coilocíticas. (Fonte: Própria)
A- Grupamentos de células escamosas maturas tipo superficiais e intermediárias apresentando
binucleação, hipertrofia e hipercromasia nuclear com halos perinucleares que caracteriza a coilocitose.
B- Células metaplásicas maturas com núcleos periféricos e espessa periferia citoplasmática, acentuado
infiltrado leucocitário.
C- Células metaplásicas maturas com núcleo central pouco dilatado caracterizando um coilócito
típico, infiltração leucocitária e hemácias.
D- Células intermediarias e metaplásicas com núcleos pouco volumosos e espessa periferia
citoplasmática, infiltrado leucocitário.
E- Célula metaplásica com periferia citoplasmática espessa com núcleo excêntrico, leucócitos
XXVIII
F- Células maturas típicas e células apresentando coilócito típico com núcleos picnóticos,
binucleados
e periféricos.
4.5.2 – Metodologia da citometria de fluxo no estudo do perfil
imunológico:
4.5.2.1
-
Análise
hematológica
de
pacientes
e
grupo
controle
Dez mililitros (10 mL) de sangue venoso periférico foi coletado em tubos
vacutainer contendo EDTA e foram homogeneizados imediatamente. A
contagem de glóbulos brancos (WBC), dosagem de hemoglobina, e contagem
de plaquetas foram realizadas no analisador hematológico (Cell Dyn-3.000). A
análise citomorfológica foi realizado em esfregaços de sangue corados pelo
Leishmann. Um total de 100 leucócitos foram contados e o resultado marcado
em porcentagem. Para conversão em valores absolutos, os valores percentuais
foram multiplicados pela contagem de leucócitos absolutos e divididos por 100.
4.5.2.2 - Análise de citometria de fluxo de perfil imunológico:
A imunofenotipagem foi realizado em amostras de sangue periférico por
citometria de fluxo. Marcadores de superfície celular foram identificados usando
anticorpos monoclonais (MoAb) específico para: i) Linfócitos B e T
(CD3FITC/CD19PE/CD45PerCP), ii) T helper e supressor de linfócitos
citotóxicos
(CD4FITC/CD8PE/CD3PerCP),
iii)
NK
e
células
NKT
(CD3FITC/CD16-56PE/CD45PerCP). Todos os AcMo foram adquiridos sistema
Imunocitoquímica Becton-Dickinson,San Jose, CA.
Cem
microlitros
(100
µL)
de
sangue
periférico
previamente
homogeneizado foram incubadas com 20 µL (vinte microlitros) de AcMo por 30
minutos a temperatura ambiente ao abrigo da luz. Após este período, a
suspensão foi homogeneizada acrescentando a mesma um mililitro (1mL) de
uma solução de lise de eritrocitos previamente diluída a 10% (FACs-lyse
XXIX
Solution / Becton Dickinson). Em seguida, suspensão celular foi submetida a
uma nova incubação por mais 10 minutos em temperatura ambiente ao abrigo
da luz. Ao fim deste tempo, a suspensão celular foi centrifugada por 5 minutos
a 1.500 RPM, o sobrenadante foi descartado e o sedimento celular
ressuspendido em solução salina tamponada de fosfato (PBS, pH 7,2) e
centrifugado novamente a 1.500 RPM; sendo esta última etapa foi repetida
mais uma vez. Finalmente, o pellet celular foi ressuspenso em 1 mL solução de
formol a 1% em PBS .
A leitura (aquisição das amostras) foi realizada em um total de 20 mil
eventos (células) por tubo em um analisador de fluorescência celular ativado
(FACScan, San Jose, CA, EUA), com software Cell Quest (Software Cell
Quest-TM, Becton Dickinson Immunocytometry Systems, San Jose, CA, EUA)
.
Após a aquisição, as células foram analisadas pelos parâmentros
determinado pelo espalhamento luminoso do laser sobre as células
sanguíneas: Forward Scatter (FSC) em escala linear que avalia o tamanho
celular e Side Scatter (SSC), também em escala linear, determinante da
complexidade celular. Por meio destes parâmetros foi feito o procedimento de
isolamento da população linfocitária (gate) e procedida a análise das
fluorescências relativas FL1, FL2 e FL3 em escala logaritimica que detecta
verde, laranja, vermelho e fluorescência, respectivamente, representativo da
reação antígeno-anticorpo conjugado ao Isohtiocyanate fluorescein (FICT ),
Phicoeritrin (PE), e Peridin Protein clorophyl (PerCP), respectivamente.
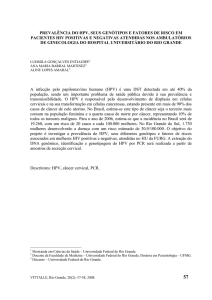
Os resultados foram expressos em porcentagem de células em
marcadores dupla tais como: linfócitos Pan T (CD3+/CD19-), células B (CD3/CD19+), linfócitos T helper (CD3+/CD4+), T supressor de linfócitos citotóxicos
(CD3+/CD8+), as células NK (CD3-/CD16-56+), e as células NKT (CD3+/CD1656+). Para conversão em valores absolutos, os valores percentuais foram
multiplicados pela contagem absoluta de linfócitos e dividido por 100 (Figuras 4
e 5). Os valores de referências para adultos sadios empregados nesse estudo
encontra-se resumido na Tabela 1.
XXX
Tabela 01 – Valores de referência da sub-população linfocitária.
Subpopulação Linfocitária
Valores de Referência
(%) / µL
Linfócitos T ou CD3
(60 – 87) / 605 - 2.460
Linfócito T Helper ou CD3+/CD4+
(32 - 61) / 600 - 1.666
Linfócito T Supressor Citotóxico ou CD3+/CD8+
(14 - 43) / 224 - 1.112
Células Natural killer ou CD16-56+
(04 - 28) / 73 - 654
Linfócitos B ou CD19
(05 - 20) / 72 - 520
Relação CD4/CD8
(1,5) / 1 - 2,5
Referência: Adaptado de SANTAGOSTINO et al, 1999.
XXXI
A
C
E
B
D
F
Figura 4 – Representação esquemática do perfil imunológico por cintometria de fluxo de uma
paciente com lesão induzida por HPV.
XXXII
A
B
C
D
E
F
Figura 5 – Representação esquemática do perfil imunológico por cintometria de fluxo
de uma paciente do grupo controle..
XXXIII
4.5.3 – Metodologia da Captura Híbrida:
A detecção do DNA- HPV foi obtida através do exame de captura hibrida
(Digene Diagnostic Inc®). O material para análise consistia de rapado
endocervical, coletado com escova fornecida pelo laboratório. Após a coleta, a
escova contendo o material biológico era condicionada em tubo com meio
liquido especialmente desenvolvido para conservação das células com seu
respectivo DNA. O processamento desse material biológico foi realizado no
laboratório Álvaro, conforme protocolos técnicos do fabricante. A carga viral
mensurada em URL/CP, por quimioluminômetro, com intensidade de luz
proporcional a carga de DNA-HPV. Com o propósito de classificar os exames
em positivos ou negativos, estabelecia-se, a cada processamento, um valor de
corte para a intensidade de luz. Quando esta intensidade superava o valor de
corte, considerava-se o exame como positivo; do contrário, era classificado
como negativo. A proporção de URL/CP para considerar o exame como
positivo era de 1, que corresponde a 1 pg/ml de DNA-HPV, ou 0,1 cópia e
vírus/ célula.
Nas mulheres com exame positivo, dada a concentração de valores de
carga viral desviada para a direita, optou-se por usar uma escala logarítmica de
distribuição e agrupá-las graficamente em 1 a < 10, 10 a < 100, 100 a <1000 e
> 1000 URL/CP. As sondas incluídas neste estudo eram dirigidas apenas aos
tipos 16,18,31.33, 35, 39, 45, 51,52, 56, 58, 59 e 60, considerados de alto risco
oncogênicos.
4.6 - Análise Estatística
Os dados obtidos nos ensaios foram analisados por diferentes
XXXIV
testes
estatísticos
e
gráficos
e
considerados
estatisticamente
significativos quando p < 0,05.
Para
melhor
compreensão
da
correlação
entre
mulheres
infectadas ou não pelo HPV e parâmetros hematológicos e imunológicos,
foram confeccionados gráficos e calculadas médias, medianas, desvios,
empregando o software Microsoft ® Excel 2000 versão 9.0.
A comparação da contagem da subpopulação linfocitária entre os
grupos foram realizadas utilizando o teste de Mann-Whitney. Os
parâmetros clínicos foram avaliados por média do teste exato de Fischer
por tabela de contingências 2x2 com ajuda do software estatístico
Statistic Pack for Social Sciences (SPSS for Windows versão 9.0;
Copyright ® SPSS, INC).
XXXV
5. RESULTADOS
5.1. Características gerais e parâmetros hematológicos da população
investigada.
Nas 30 mulheres pertencentes ao grupo controle, 14 eram de cor
branca, quatro pretas e 12 mulatas. Com relação à faixa etária, observou-se
variação de 21 a 49 anos com media de 30 anos (Tabela 2).
Ainda neste grupo, a leucometria variou de 4.000 a 11.900/mm3 com
media de 5.900/mm3. A contagem de linfócitos variou de 1.200/mm3 a
2.600/mm3, com mediana de 1.760/mm3. Com relação à contagem de
monócitos observaram-se os seguintes resultados: i) mínimo de 140/mm3, ii)
máximo de 476/mm3, iii) mediana de 252/mm3. A contagem mínima de
granulócitos foi de 2.183/mm3, máxima de 9.282/mm3 e mediana de 3.789/mm3
(Tabela 2).
No grupo pertencente a mulheres infectadas pelo HPV, 20 eram de cor
branca, uma preta e nove mulatas. Com relação à faixa etária, observou-se
variação de 18 a 49 anos com media de 30 anos (Tabela 3).
Neste, grupo, a leucometria variou de 4.100 a 13.000/mm3 com média
de 2.490/mm3. A contagem de linfócitos variou de 1.000/mm3 a 5.000/mm3,
com mediana de 2.493/mm3. Com relação à contagem de monócitos,
observaram-se os seguintes resultados: i) mínimo de 164/mm3, ii) máximo de
1.300/mm3, iii) mediana de 580/mm3. A contagem de granulócitos mínima foi de
2.625/mm3, máxima de 8.300/mm3 e mediana de 4.960/mm3 (Tabela 3).
A correlação estatística entre os dois grupos de mulheres e parâmetros
hematológicos determinados pela leucometria total, contagem absoluta de
linfócitos, monócitos e granulócitos estão relacionados nas figuras 6 a 9
respectivamente.
XXXVI
Observou-se correlação estatisticamente significativa entre os dois
grupos para os seguintes parâmetros: leucometria com p< 0,0002 (Figura 6),
contagem com de linfócitos com p< 0,0003 (Figura 7) e contagem de
monócitos, com p< 0,0001 (Figura 8), porém não na contagem de granulócitos
p= 0,01 (Figura 9).
XXXVII
Tabela 2. Características gerais e parâmetros hematológicos das mulheres pertencentes ao grupo
controle.
N°
IDADE
COR
LEUC (mm3)
LINF (mm3)
MON (mm3)
GRAN (mm3)
1
31
B
6.200
2.000
248
3.906
2
32
B
5.100
1.500
204
3.366
3
27
B
5.200
1.500
208
3.432
4
26
M
5.500
2.000
220
3.245
5
42
B
5.400
1.500
162
3.672
6
49
M
7.100
2.300
284
4.544
7
35
B
5.200
1.700
156
3.672
8
25
M
4.900
2.100
245
2.499
9
44
P
4.700
1.300
141
3.196
10
31
M
6.600
1.600
264
4.686
11
20
B
8.100
1.800
567
5.670
12
55
M
4.800
1.300
288
3.168
13
32
M
5.400
1.400
324
3.672
14
40
M
7.200
2.100
288
4.752
15
38
M
5.000
1.500
150
3.350
16
48
M
7.100
2.600
284
2.183
17
38
B
4.200
1.200
168
2.814
18
41
P
5.100
1.600
204
3.213
19
21
B
6.900
1.300
207
5.313
20
41
B
5.900
2.200
354
3.304
21
28
M
7.500
2.500
300
4.650
22
31
B
4.600
1.600
230
2.668
23
31
P
6.000
2.300
180
3.480
24
22
M
11.900
2.100
476
9.282
25
24
M
5.400
1.600
162
3.564
26
35
B
6.500
1.500
390
4.550
27
31
B
4.600
1.600
230
2.668
28
31
P
6.000
2.300
180
3.480
29
32
B
4.000
1.500
160
2.560
30
21
B
4.800
1.500
288
3.120
Min
21
xxx
4.000
1.200
141
2.183
Max
49
xxx
11.900
2.600
567
9.282
MD
33,4
xxx
5.400
1.900
230
3.480
M
30
xxxx
6.021
1774
255
3.907
OBS: B (cor branca), M (mulata); P (preto ou negro); Leuc. (Leucometria); Linf. (Linfócitos); Mon.
(Monócitos); Gran. (Granulócitos); Min. (mínimo); Máx. (Máximo); MD. (Mediana); M (Media).
XXXVIII
Tabela 3. Características gerais e parâmetros hematológicos das mulheres infectadas pelo HPV
N°
IDADE
COR
LEUC (mm3)
LINF (mm3)
MON (mm3)
GRAN (mm3)
01
39
B
7.100
1.400
710
5.396
02
42
B
5.700
1.800
570
3.306
03
24
B
8.600
3.000
774
4.730
04
30
B
8.400
1.700
840
5.796
05
34
B
5.000
1.000
700
3.300
06
29
M
9.500
2.600
1.235
5.605
07
31
B
5.000
1.700
400
2.900
08
44
M
5.000
1.900
450
2.650
09
38
B
6.500
2.400
650
3.380
10
38
B
8.000
1.600
560
4.560
11
29
B
7.000
2.100
270
4.340
12
48
M
7.500
3.300
247
2.625
13
35
M
9.000
3.500
540
4.950
14
35
M
11.000
4.100
660
6.160
15
32
B
8.700
3.000
435
5.220
16
34
B
5.000
1.200
250
3.500
17
30
B
9.000
2.700
540
5.760
18
34
M
10.000
3.000
500
6.500
19
18
M
10.000
3.900
500
5.600
20
39
B
6.000
2.300
300
3.300
21
35
B
13.000
3.300
1.300
8.300
22
27
M
11.300
3.300
452
7.400
23
34
M
4.100
1.200
164
2.700
24
36
B
7.000
2.500
280
4.200
25
43
P
9.800
3.100
784
5.800
26
40
B
12.000
3.000
840
7.400
27
35
B
11.800
5.000
826
8.300
28
35
B
7.000
2.200
490
4.270
29
42
B
8.500
1.700
765
6.035
30
35
B
6.500
1.300
390
4.810
Min
18
xxx
4.100
1.000
164
2.625
Max
49
xxx
13.000
5.000
1.300
8.300
Med
34,8
xxx
8.200
2.450
540
4.880
M
30
xxx
8.129
2.525
590
4.991
OBS: B (cor branca), M (mulata); P (preto ou negro); Leuc. (Leucometria); Linf. (Linfócitos); Mon.
(Monócitos); Gran. (Granulócitos); Min. (mínimo); Máx. (Máximo); MD. (Mediana); M (Media).
XXXIX
5.2. Detecção do papilomavírus humano em amostras de citologia cervical
De acordo com análises citológicas, 30 (50%) pacientes apresentaram lesão
intraepitelial cervical de baixo grau ou LSIL do termo em inglês low grade
squamous intraepithelial lesion, associadas ao HPV, diagnosticada pela citologia
cervical e 30 (50%) não apresentaram alterações associadas ao HPV (mulheres
saudáveis). Para a confirmação da etiopatogenia das lesões e tipificação do HPV
foi utilizada a técnica de captura híbrida nas pacientes com o vírus HPV e LSIL,
apresentado o seguinte resultado: oito 08 (27%) apresentaram HPV de alto
risco, 16 (53%) e 6 das 30 (20%) estavam infectadas com os dois tipos de HPV
(Tabela 4 e 5).
Tabela 4. Porcentagem de pacientes portadoras de HPV de alto risco e de
baixo risco oncongênico.
Tipo de HPV
Número de pacientes
(%)
HPV – A
08
27,0%
HPV – B
16
53,0%
HPV AB
06
20%
OBS: HPV-A (HPV de baixo risco); HPV-B (HPV de alto risco).
XL
Tabela 5. Parâmetros clínicos e epidemiológicos de 30 pacientes com LSIL estratificada por idade, tipo de lesão,
presença oncogênico de baixo grau ( destaque em verde) e alto risco (destaque em vermelho) do HPV e perfil
imunológico.
Tipo de
HPV
HPV
lesão
AR
BR
39
LSIL
NEG
02
42
LSIL
03
24
04
Nº
ID
CD3/mm³
CD4/mm³
CD8/mm³
CD19/mm³
NK/mm³
NKT/mm³
CD4/CD8
01
POS
1079
742
280
266
42
0
2,65
NEG
POS
1386
900
594
180
54
0
1,51
LSIL
POS
NEG
2260
1200
1170
300
60
5,4
1,02
30
LSIL
NEG
POS
1234
748
340
170
51
3,0
2,2
05
34
LSIL
POS
POS
700
430
250
100
20
9
1,72
06
29
LSIL
NEG
POS
1835
1248
832
494
130
1,9
1,52
07
31
LSIL
NEG
POS
1122
697
425
153
187
5,1
1,64
08
44
LSIL
POS
POS
1292
798
494
152
152
3,8
1,61
09
38
LSIL
POS
NEG
1630
672
912
271
72
1,2
0,73
10
38
LSIL
NEG
POS
1216
738
432
160
48
3,2
1,7
11
29
LSIL
POS
NEG
1302
630
651
84
84
0,2
0,96
12
48
LSIL
POS
NEG
2730
1287
924
330
462
9,9
1,39
13
35
LSIL
NEG
POS
1106
1439
805
429
105
3,7
1,78
14
35
LSIL
POS
POS
2549
1517
1185
574
164
0
1,27
15
32
LSIL
NEG
POS
1857
1350
750
270
30
0
1,8
16
34
LSIL
NEG
POS
875
600
348
120
12
0
2,5
17
30
LSIL
NEG
POS
2160
1242
702
405
81
2,1
1,76
18
34
LSIL
NEG
POS
1770
750
870
600
90
1,5
0,86
19
18
LSIL
POS
NEG
2613
874
1053
663
174
1,2
1,4
20
39
LSIL
NEG
POS
1544
1058
782
230
69
2
1,35
21
35
LSIL
NEG
POS
2264
1320
990
231
99
1
1,33
22
27
LSIL
POS
NEG
2678
1419
1056
396
165
3
1,34
23
34
LSIL
NEG
POS
898
552
240
144
60
6
2,3
24
36
LSIL
POS
NEG
2016
1275
650
250
50
1
1,96
25
43
LSIL
POS
POS
2289
1023
1147
310
93
6,2
0,89
26
40
LSIL
POS
NEG
2040
1290
750
120
510
9
1,72
27
35
LSIL
NEG
POS
4100
2100
1700
650
100
5
1,25
28
35
LSIL
POS
POS
1518
902
616
220
374
6,6
1,46
29
42
LSIL
NEG
POS
1241
782
510
102
85
3,4
1,5
30
35
LSIL
POS
POS
923
650
429
91
52
9,1
1,51
OBS: HPV-AR (HPV de alto risco em destaque vermelho), HPV-BR (HPV de baixo risco em destaque verde).
XLI
5.3. Investigação dos parâmetros imunológicos da população analisada
Com base na resposta imune ao HPV, investigamos possíveis associações entre
HPV e avaliação quantitativa da subpopulação linfocitária determinada pela
citometria de fluxo (Tabelas 5 a 7 e Figuras 10 a 16).
Na avaliação quantitativa do perfil imunológico determinado pela contagem ds
linfócitos
T
(CD3+)
e
subpopulações:
T
helper
(CD3+/CD4+)
e
T
supressor/citotóxico (CD3+/CD8+), linfócitos B (CD19+), células NK (CD1656+/CD45+) e células NKT (CD3+/CD16-56+), constatou-se elevada contagem de
linfócitos TCD8+ predominantemente nas pacientes infectadas por HPV de alto risco
quando comparados com mulheres de baixo risco (Tabela 5).
Na mulheres com DNA do HPV de alto risco, 5 das 8 pacientes (62,5%)
tiveram aumento da expressão de linfócitos TCD8+. Inversamente, considerando
apenas os pacientes com DNA de HPV de baixo risco, apenas 2 das 16 (12,5%)
pacientes apresentaram um aumento de linfócitos CD8 positivos T quando comparado
com pacientes que exibem alto risco DNA HPV. Além disso, a avaliação quantitativa
de CD19 foi normal em pacientes que exibem LSIL e HPV, quando comparado com
o grupo controle composto por mulheres saudáveis (Tabela 5).
Nas 30 mulheres pertencentes ao grupo controle, a contagem de
linfócitos T variou de 949 a 2.080/mm3 com mediana de 1.303/mm3. A
contagem de linfócitos T helper variou de 574/mm3 a 1.216/mm3 com mediana
de 777/mm3. Para os linfócitos T supressor citotóxico constataram-se os
seguintes níveis: nível mínino 264/mm3, máximo 805/mm3 e mediana de
420/mm3. Com relação às contagens de linfócitos B, observaram-se os
seguintes resultados: contagem mínima de 96/mm3, máxima de 400/mm3 e
mediana de 198/mm3. A contagem mínima de células NK foi de 130/mm3,
máxima de 399/mm3 e mediana de 232/mm3. A contagem de células NKT foi de
mínimo de 13/mm3; máximo de 184/mm3 e mediana de 70/mm3. Neste grupo
de mulheres, todos os parâmetros acima citados bem como a relação
XLII
CD4/CD8 mostraram-se dentro dos limites de normalidade conforme
demonstrado anteriormente na tabela 2 (Tabela 6).
No grupo de mulheres infectadas pelo HPV, a contagem de linfócitos T
variou de 700 a 4.100/mm3 com média de 1.700/mm3. A contagem de linfócitos
T helper variou de 430/mm3 a 2.150/mm3 com mediana de 910/mm3. Para os
linfócitos T supressor citotóxico constataram-se os seguintes níveis: contagem
mínima de 280/mm3, máximo 1.700/mm3 e mediana de 728/mm3. Com relação
às contagens de linfócitos B, observaram-se os seguintes resultados: mínimo
de 84/mm3, máximo de 663/mm3 e mediana de 240mm3. A contagem mínima
de células NK foi de 12/mm3, máxima de 510/mm3 e mediana de 84,5/mm3. As
células NKT por sua vez observou-se ausência dessas células em 5 casos;
contagem máxima de 30/mm3 e mediana de 3,3/mm3. Neste grupo, de
mulheres, o cálculo da relação CD4/CD8 mostrou variação de 0,73 a 2,65 com
mediana de 1,5 (Tabela 7).
A análise estatística dos parâmetros imunológicos dos dois grupos
demonstrou diferenças entre si para: contagem de células TCD8 com p= 0,002
(Figura 12), relação CD4/CD8 com p< 0,003 (Figura 13), contagem de células
NK com p< 0,0002 (Figura 15) e células NKT com p<0,00001 (Figura 16). Com
relação aos parâmetros: linfócitos T total (Figura 10), Linfócitos B total (Figura
14) e linfócitos T helper (Figura 11), não se constataram diferença
estatisticamente significativa entre a contagem destas células e os grupos
HPV+ e HPV-, sugerindo a pouca influência da fisiopatologia do HPV nestas
células do sistema imune a nível sistêmico, ao contrário do observado com as
células TCD8+, células NK e NKT.
XLIII
Tabela 6. Perfil imunológico das mulheres pertencentes ao grupo controle
Caso
n
Linf. T
CD3/m
3
m
Linf. Th
LTSC
3
Rel.
3
Linf. B
Cel. NK
3
Cel. NKT
3
3
CD4 /mm
CD8 /mm
CD4/CD8
CD19 /mm
CD16-56 /mm
CD16-56/CD3/mm
01
1.480
920
600
1,37
260
280
20
02
1.110
660
390
1,69
120
240
60
03
1.000
780
285
1,69
150
315
45
04
1.440
960
580
2,73
160
340
100
05
1.065
690
300
1,65
165
180
75
06
1.794
1038
690
2,3
253
322
23
07
1.479
918
405
1,5
170
255
17
08
1.323
924
462
2
357
231
42
09
1.040
799
630
2
143
156
13
10
1.184
774
268
1,6
128
176
32
11
1.260
738
504
1,95
342
252
108
12
949
624
264
1,5
130
234
78
13
1.050
574
405
2,2
182
182
28
14
1.491
1.092
441
1,4
294
168
105
15
1.110
630
420
2,7
210
210
90
16
2.080
750
650
1,5
286
260
104
17
1.125
660
288
2,0
156
180
78
18
1.072
640
400
2,3
160
240
80
19
988
715
403
1,6
130
130
84
20
1.738
1.144
572
1,8
264
143
132
21
1.800
1.250
475
2,0
400
325
75
22
1.248
800
320
2,0
160
224
32
23
1.541
1.035
667
2,6
230
276
184
24
1.575
840
805
2,5
336
399
84
25
1.088
800
336
1,6
256
208
64
26
1.095
720
495
1,45
165
195
30
27
1.248
720
320
2,25
96
226
64
28
1.541
1.150
667
1,72
230
276
161
29
1.140
750
300
2,5
195
285
45
30
1.050
750
420
1,79
225
165
60
Min.
949
574
264
1,15
65
130
13
Max
2.080
1.250
805
2,75
400
399
184
Med
1.216
777
420
1,87
188
232
69
M
1.316
833
463
1,92
213
237
72
OBS: Linf B. (Linfócitos B), Linf T (Linfócitos T); Linf Th (Linfócitos T helper); Linf TSc
(Linfócitos T supressor citotóxico); Cel. NK (Células Natural Killer); Cel. NKT (Células
XLIVNKT);
(mínimo); Máx. (Máximo); Med. (Mediana), M (Média).
Tabela 7. Perfil imunológico das mulheres infectadas pelo HPV
Caso
Linf. T
Linf. Th
3
LTSC
3
Rel.
3
Linf. B
Cel. NK
3
Cel. NKT
3
3
n
CD3/mm
CD4 /mm
CD8 /mm
CD4/CD8
CD19 /mm
CD16-56 /mm
CD1656/CD3/mm
01
1.079
742
280
2,65
266
42
0
02
1.386
900
594
1,51
180
54
0
03
2.260
1.200
1.170
1,02
300
60
5,4
04
1.234
748
340
2,2
170
51
30
05
700
430
250
1,72
100
20
9
06
1.835
1.248
832
1,52
494
130
1,9
07
1.122
697
425
1,64
153
187
5,1
08
1.292
798
494
1,61
152
152
3,8
09
1.630
672
912
0,73
271
72
12
10
1.216
738
432
1,7
160
48
3,2
11
1.302
630
651
0,96
84
84
0,2
12
2.730
1.287
924
1,39
330
462
9,9
13
2.106
1.439
805
1,78
429
105
3,7
14
2.549
1.517
1.185
1,27
574
164
0
15
1.857
1.350
750
1,8
270
30
0
16
875
600
348
2,5
120
12
0
17
2.160
1.242
702
1,76
405
81
2,1
18
1.770
750
870
0,86
600
90
1,5
19
2.613
874
1.053
1,4
663
174
1,2
20
1.544
1.058
782
1,35
230
69
2
21
2.264
1.320
990
1,33
231
99
1
22
2.678
1.419
1.056
1,34
396
165
3
23
898
552
240
2,3
144
60
6
24
2.016
1.275
650
1,96
250
50
1
25
2.289
1.023
1.147
0,89
310
93
6,2
26
2.040
1.290
750
1,72
120
510
9
27
4.100
2.100
1.700
1,25
650
100
5
28
1.518
902
616
1,46
220
374
6,6
29
1.241
782
510
1,5
102
85
3,4
30
923
650
429
1,51
91
52
9,1
Min.
700
430
280
0,73
84
12
0
Max.
4.100
2.100
1.700
2,65
663
510
30
Med.
1.700
901
726
1,54
240
84,5
3,3
M
1.813
1.006,9
742
1,56
289
131
4,73
OBS: Linf B. (Linfócitos B), Linf T (Linfócitos T); Linf Th (Linfócitos T helper); Linf TSc (Linfócitos T
supressor citotóxico); Cel. NK (Células Natural Killer); Cel. NKT (Células NKT); Min. (mínimo); Máx
(Máximo); Med. (Mediana); M (Media).
XLV
HPV+
HPV-
p=0.0002
Figura 6. Distribuição da leucometria em mulheres HPV+ e HPV-.
.
XLVI
HPV
+
HPV
-
p=0.0003
Figura
7.
Distribuição
da
contagem
de
linfócitos
em
mulheres
HPV+
e
HPV-.
XLVII
HPV+
p<0.0001
HPV-
Figura 8. Distribuição da contagem de monócitos em mulheres HPV+ e HPV-.
XLVIII
HPV+
p=0.01
HPV-
Figura 9. Distribuição da contagem de granulócitos em mulheres HPV+ e HPV-.
XLIX
HPV+
p=0.018
HPV-
Figura 10. Distribuição dos valores de linfócitos TCD3+ em mulheres HPV+ e HPV-.
L
HPV+
p=0.03
HPV-
Figura 11. Distribuição dos valores de linfócitos BCD19+ em mulheres HPV+ e HPV-.
LI
HPV+
p=0.022
HPV
-
Figura 12. Distribuição dos valores de linfócitos TCD4+ em mulheres HPV+ e HPV-.
LII
HPV+
p=0.0002
HPV-
Figura 13. Distribuição dos valores de linfócitos TCD8+ em mulheres HPV+ e HPV-.
LIII
HPV+
p=0.003
HPV-
Figura 14. Distribuição da relação CD4/CD8 em mulheres HPV+ e HPV-.
LIV
HPV
+
p=0.0002
HPV-
Figura 15. Distribuição dos valores de células NK (CD16-56+) em mulheres HPV+ e HPV-.
LV
HPV+
HPV-
p<0.00001
Figura 16. Distribuição dos valores de células NKT (CD3+/CD16-56+) em mulheres HPV+ e
HPV
LVI
6 - DISCUSSÃO
A comunidade médica mundial está empenhada na elaboração de programas de
vacinação contra o HPV. Antes que estes sejam implementados é importante
reconhecer, que talvez este esforço isolado não seja suficiente, uma vez que a
erradicação da infecção pelo HPV é também dependente da resposta imune celular.
Estudos têm demonstrado níveis significativamente mais baixos de células de defesa
tipo TH1 (células de Langerhans) no epitélio cervical de pacientes portadoras de lesões
intraepiteliais de alto grau (LIEAG) quando comparadas aquelas encontradas no epitélio
cervical de pacientes saudáveis (EVANS et al, 1997; BONTKES et al 2000; ).
Sabe-se ainda que os linfócitos T citotóxicos (LTC) desempenham um papel
importante na imunidade local, impedindo a progressão da doença.
Existe na literatura fortes evidências de que os LTC específicos para o
HPV de alto poder oncogênico parecem ter um papel central na inibição da
carcinogênese cervical (BOR-CHING SHEU, et al.,2007). As referidas células
desempenham uma função importante no reconhecimento e defesa contra
antígenos específicos do HPV e agindo dessa
forma como sentilenas no
combate de células infectadas. Trabalhos têm demonstrado que dependendo
do tipo de resposta Th específica para o vírus HPV-16 produtor da
oncoproteína E7 pode resultar no clearance ou na persistência do vírus em
pacientes com neoplasia cervical (DE GRUIJL TD, et al., 1998).
Em estudo prévio, KADISH (2002) avaliou in vitro a resposta imune celular
linfoproliferativa aos peptídios E6 e E7 do HPV 16 em 136 mulheres portadoras de NIC
(neoplasia intraepitelial cervical) I e II seguidas durante um ano, Neste estudo observouse que a resposta imune celular ao peptídio E7 esteve relacionada a clarificação da
infecção e a regressão da doença neste período de tempo.
O presente estudo teve a finalidade de avaliar o perfil imunológico e a resposta
imune sistemica ao HPV, mediante a caracterização quantitativa da subpopulação
LVII
linfocitária do sangue periférico por citometria de fluxo em mulheres infectadas com o
HPV de baixo ou alto risco oncogênico e portadoras de LSIL. Estudando também
paralelamente mulheres com as mesmas características sem doença, as quais
constituiram o grupo contole
Identificamos uma diminuição na contagem de linfócitos TCD4+, com relativo
aumento no número de células TCD8+ entre as pacientes acometidos com HPV de alto
risco quando comparados com aquelas infectadas com HPV de baixo risco e
principalmente com as mulheres pertencentes ao grupo controle (Tabelas 5 a 7 e Figuras
10, 12, 13 e 14). Tal fato sugere que possivelmente, o HPV, especialmente o de alto
risco poderia estar induzindo um efeito citopático nos linfócitos TCD4+ como uma
estratégia de subverter a resposta imunitária destas pacientes frente à infecção.
Estudos anteriores demonstram que pacientes com câncer cervical foi observado
uma perda completa ou uma diminuição da expressão das moléculas de classe I em
células tumorais. Este mecanismo poderia representar uma estratégia do vírus para
escapar
da vigilância imunológica e, consequentemente, não ser reconhecido em
virtude da ausência
da diminuição da expressão dos antígenos por parte destas
moléculas apresentadoras. Consequentemente, as pacientes apresentariam uma redução
do número de linfócitos T específicos necessárias para erradicar o vírus. (MONNIERBENOIT S, et al., 2006; DE BOER MA, et al., 2007). Em contrapartida,
KANODIA (2007) observou que a expressão de moléculas imunossupressoras no
microambiente cervical favoreceu ao escape viral.
O que nos faz pensar inicialmente que ocorreria uma maior expressão de
moléculas imunossupressoras a nível local, que posteriormente seriam inibidas a nível
sistêmico. O que justifica nossos achados.
Neste estudo, observamos ainda um decréscimo na quantidade de linfócitos
TCD4+ e um acréscimo de TCD8+ nas pacientes infectadas com HPV de alto risco
oncogênico, similarmente ao que acontece em pacientes infectados pelo vírus da
imunodeficiência humana (HIV). Neste caso específico, o mecanismo de apoptose induz
a um esgotamento fisiológico dos linfócitos T no curso da infecção viral diminuíndo a
LVIII
resposta imune e contribuindo desta forma para o quadro de imunodeficiência
(WATTRE P, et al., 1996).
Todavia, quando analisamos a população de células NK e NKT, independente do
poder oncogênico do HPV, observou-se uma diminuição acentuada nas duas subpopulações avaliadas (Tabelas 5 a 7 e Figuras 15 e 16). O decréscimo observado nestas
sub-populações pode estar relacionado com a expressão aumentada de proteínas proapoptóticas, que poderia ser decorrente da ativação de mecanismos indutores de
apoptose.
Entretanto, não observamamos
diferenças significativa na contagem de
linfócitos B no sangue periférico nos dois grupos de mulheres estudados (com e sem
HPV), o que talvez não ocorresse se tivesse sido avaliado material cérvico vaginal, uma
vez que a mucosa genital normal é infiltrada por linfócitos TCD4+, TCD8 + , células
plasmáticas , células dendríticas (DCs) e macrófagos (GARCIA-CHACON R, et al.
2009; INSINGA R.P, et al., 2009). Nossos resultados poderiam traduzir ainda uma
participação limitada da resposta imune humoral , quando a infecção já está instalada.
Constatamos também uma contagem mais elevada de linfócitos nas pacientes
portadoras de HPV. Em adição, outro estudo examinou a expressão aumentada de
linfócitos T CD3
entre as pacientes com NIC
III (MALUF PJ, et al., 2008).
Resultados semelhantes foram observados em uma análise por imunohistoquímica da
expressão de células TCD4+ e TCD8+ na presença do HPV de alto risco oncogênico
em lesões pré malignas e malignas do colo uterino (MONNIER-BENOIT et al, 2006).
Concluindo, podemos dizer que as respostas imune celular e humoral são
essenciais no processo de progressão ou regressão da infecção e⁄ ou lesão induzida pelo
HPV. Associada a isso, diferentes linhas de pensamento evidenciam principalmente o
papel da resposta imune celular neste processo. ( KARIM 2011).
Por outro lado, existe ainda a necessidade de estudos adicionais, como finalidade
de entendimento da interação entre o HPV e o hospedeiro, como também da resposta
deste hospedeiro ao vírus.
LIX
7. CONCLUSÕES
Baseados nos objetivos propostos, concluímos que:
•
Observou-se a uma modulação do sistema imune adaptativo a nível
sistêmico durante a infecção pelo HPV, independente do grau de
oncogenicidade do vírus, sendo pronunciadamente mais evidente na
diminuição do número de células NK e NKT e aumento das células TCD8+.
•
Durante a infecção pelo HPV as mulheres acometidas com o vírus de alto
poder oncogênico apresentam uma modulação da resposta imune adquirida
mais acentuada quando comparada com as mulheres infectadas pelo HPV de
baixo grau, caracterizada pela diminuição acentuada na contagem de
linfócitos TCD4+ com relativo aumento dos linfócitos TCD8+.
•
Não foi observada correlação estatisticamente significativa na contagem
de células B (CD19+), levando a crer na pouca participaçào desses linfócitos
imunidade humoral na resposta imune a nível sistêmico da infecção pelo
HPV.
•
O aprofundamento nos estudos envolvendo uma maior caracterização
imunofenotípica destas células do sistema
imune e também a nível local
associada a imunobiologia do vírus pode contrubuir de forma significativa aos
conhecimentos atuais acerca de prováveis mecanismos entre virus e sistema
imune do hospedeiro.
•
Esses estudos constitui de uma
investgação preliminar para o
entendimento da fenotipagem da infecção pelo HPV em mulheres com LSIL.
LX
8 – REFERÊNCIAS BIBLIOGRÁFICAS
1.
ABBAS AK, et al. (2008). “Celular and molecular Immunology”, 6.ed
USA: Wb Saunders.
2.
ADAMS, V. et al. (1996). "Detection and typing of human papillomavirus
in biopsy and cytological specimens by polymerase chain reaction and
restriction enzyme analysis: A method suitable for semiautomation". J. Med.
Virol. 48:161-170.
3.
ALBRING L, et al. (2006). “O cancer do colo do útero, o Papilomavírus
Humano (HPV) e seus fatores de risco e as mulheres indígenas Guarani:
Estudo de revisão”. RDAC, 38(2): 87-90.
4.
ALMADORI G, et al. (2005). “Molecular markers in laryngeal squamous
cell carcinoma: towards integrated clinicobiological approach”. Eur J câncer;
41(5): 638-93.
5.
ALVES DB, et al. (2010). “CD4 and CD8 T lymphocytes and NK cells in
the stroma of the uterine cervix of women infected with human papillomavirus”.
Rev Soc Bras Med Trop, 4: 425-9.
6.
AU, WW. (2004) “Life style, envirinomental and genetic susceptibility to
cervical cancer”. Toxicology, 198(1-3), p.117-20.
7.
BAUER, H.M.; MANOS, M.M. (1993). "PCR Detection of Genital Human
Papillomavirus". In: PERSING, D.H.
et al. (Ed.).
"Diagnostic molecular
microbiology principles and applications". Rochester: Mayo Foundation. cap.
2.16, p.407-413.
8.
BERNARD, H.U. et al. (1994). "Identification and assessment of known
and novel human papillomaviruses by polymerase chain reaction amplification,
restriction
fragment
length
polymorphisms,
nucleotide
sequence,
and
phylogenetic algorithms". J. Infect. Dis. 170:1077-1085.
9.
BONTKES HJ, et al. (2000). “Human papillomavirus type 16, E6/E7-
specific cytotoxic T lymphocytes in women with cervical neoplasia”. Int J
Cancer. 88: 92–98.
10.
BONTROP
RE,
et
al.
(2000)
“The
evolution
of
the
major
histocompatibility complex: Insights from phylogeny. In: R.L.A.A. Warrens
(Ed.). HLA in health and disease. London: Academic Press”. The evolution of
the major histocompatibility complex: insigthts from phylogeny, p.163-169.
LXI
11.
BOR-CHING SHEU, et al. (2007). “Immune concept of human
papillomaviruses and related antigens in local cancer milieu of human cervical
neoplasia”. Journal compilation Japan Society of Obstetrics and Gynecology;
3: 103-13.
12.
BOSCH, FXAN, et al. (2008) “Epidemiology and natural history of human
papilomavirus infections and type-specific implications in cervical neoplasia.
Vaccine”, 26(10), p, k 1-16.
13.
BRASIL mds. (2008). Instituto Nacional de Câncer do Ministério da
Saúde (INCA).
14.
CAMPOS et al. (2005) “Prevalência do Papilomavírus humano e seus
genótipos em mulheres portadoras e não portadoras do vírus da
imunodeficiência humana”. Revista Brasileira de Ginecologia e obstetrícia,
27(5): 248-56.
15.
CHOW, V.T.K. et al. (2000). "Identification of multiple genital HPV types
and sequence variants by consensus and nested type-specific PCR coupled
with cycle sequencing". Pathology. 32:204-208.
16.
COX, J.T. (1999). "Evaluating the role of HPV testing for women with
equivocal Papanicolaou test findings". JAMA. 281:1645-1647.
17.
CUZICK, J. (2000). "Human Papillomavirus testing for primary cervical
cancer screening". JAMA. 283:108-109.
18.
DE BOER MA, et al. (2007). “Circulating human papillomavirus type 16
specific T-cells are associated with HLA Class I expression on tumor cells, but
not related to the amount of viral oncogene transcripts”. Int J Cancer;
121:2711–2715.
19.
DE GRUIJL TD, et al. (1998). “Differential T helper cell responses to
human papillomavirus type 16, E7 related to viral clearance or persistence in
patients with cervical neoplasia: a longitudinal study”. Cancer Res; 58:1700–
1706.
20.
EDDIE et al. (1999). “Freqüência da infecção pelo Papilomavírus
Humano em Mulheres com ectopia Cervical. Revista Brasileira de Ginecologia
Obstetrícia”. 21(8).
21.
EINSTEIN MH, et al. (2009) “Clinician's guide to human papillomavirus
immunology: knowns and unknowns”. Lancet Infect Dis. 9:347-56.
LXII
22.
ETTINI, JS, et al. (2003). “PCR diagnosis of HPV in cervical biopsies of
CIN and invasive neoplasia formerly diagnosed a HPV negative”. Acta Cytol.
47(4): 545-9.
23.
EVANS EML, et al. (1997). “Infiltration of cervical cancer tissue with
human papillomavirus-specific cytotoxic T-lymphocytes”. Cancer Res. 57:
2943–2950
24.
FARAH, S.B. (2008). “DNA Segredos e mistérios”, 2.ed São Paulo:
Sarvier.
25.
FEBS J., (2010) Aug 28: doi: 10.1111/j.1742-4658.2010.07833.x
26.
FIDLER, IJ. (2003). “The pathogenesis of cancer metastasis: the seed
and soil hypothesis revisited”. Nat Rev cancer, 3(6):453-8.
27.
FILIPPIN
et
al.
(2006)
“Determinação
do
número
de
regiões
organizadoras de nucléolo (agnor) em lesões do epitelio cervical uterino”.
RDAC, 38(3):133-139.
28.
FRANCESCHI, S. (2005). “The IARC commitment to câncer prevention:
The example of papillomavirus and cervical câncer”. Recent Results Cancer
Res,V. 166, p. 277-97.
29.
GARCIA-CHACON R, et al. (2009). “Immunobiology of HPV Infection”.
Arch Med Res. 40:443-8.
30.
GOMPLES C, et al. (1997). "Citologia ginecológica e suas bases
anatomoclinicas”. São Paulo:Manole.
31.
GONÇALVES, M.A. e E.A. DONADI. (2004). “Immune cellular response
to HPV: current concepts”. Braz J Infect Dis. 8(1): 1-9.2204.
32.
GRAVITT, P.E. et al. (1998). "Genotyping of 27 human papillomavirus
types by using L1 consensus PCR products by a single hybridization, reverse
line blot detection method". J. Clin. Microbiol. 36:3020-3027.
33.
GUERRA, MR, et al. (2005). “Risco de câncer no Brasil: tendência e
estudos epidemiológicos mais recentes”. Revista Brasileira da Cancerologia,
51(3): 227-234.
34.
HIETANEN, S. et al. (1997). "Type I diabetic pregnancy and subclinical
human papillomavirus infection". Clin. Infect. Dis. 24:153-156.
35.
INSINGA RP, et al. (2009). “Epidemiologic natural history and clinical
management of Human Papillomavirus (HPV) Disease: a critical and
LXIII
systematic review of the literature in the development of an HPV dynamic
transmission model”. BMC Infect Dis. 29:119.
36.
IWASAWA, A. et al. (1997). "J. Human papillomavirus in squamous cell
carcinoma of the vulva by polymerase chain reaction". Obstetr. Gynecol. 89:8184.
37.
KANESHIMA et al., (2001). “Avaliação do método PCR- RFLP para
tipagem de HPV em infecções cervicais de pacientes atendidas do Lepac,
Universidade Estadual de Maringá. Acta Scientiarum”. 23(3): 731-737.
38.
KANODIA S, et al. (2007). Mechanisms used by human papillomaviruses
to escape the host immune response. Curr Cancer Drug Targets. 7, p.79-89.
39.
KARIM R, et al. (2011). “Human papillomavirus deregulates the response
of a cellular network comprising of chemotactic and proinflammatory genes”.
PLoS One. 14;6(3):e17848.
40.
KELLY, A.,P.,J.J. MONACO, et al. (1991). “A new human HLA class II –
related locus”, DM. Nature, 353(6344): 571-3.
41.
KODON K. (2009). “Development of na HPV vaccine – remainig issues
and perspective”. Nippon rinsho; 67(1): 62-8.
42.
LANIER, L.L. (1997). “Natural Killer cells: from no receptors to too many”.
Immunity, 6(4):371-8.
43.
LEPIQUE AP, et al. (2009). “HPV vaccionation: the beginning of the end
of cervical cancer? – A review”. Memoriais do Instituto Oswaldo Cruz; 104 (1):
1-10.
44.
LINDSEY et al. “Vírus do Papiloma: Vias de transmição, Risco
oncogênico e co-fatores”. Laes e Haes. 25/146.
45.
MADKAN VD, et al. (2007). "The oncogenic potential of human
papillomaviruses: a rewiew onthe role of rost genetics and environmetal cofactors".
British Journal of dermatology. 157(2):2208-241.
46.
MALUF PJ, et al. (2008). “EFT lymphocytes (CD3) may participate in the
recurrence of cervical intraepithelial neoplasia grade III”. Arch Gynecol Obstet.
278(6):525-30.
47.
MANOS, M.M.
et al. (1989). "Use of polymerase chain reaction
amplification for the detection of genital human papillomaviruses". Cancer Cells.
7:209-214.
LXIV
48.
MONNIER-BENOIT S, et al. (2006). “Immunohistochemical analysis of
CD4+ and CD8+ T-cell subsets in high risk human papillomavirus–associated
pre-malignant and malignant lesions of uterine cervix”. Gynecol Oncol, 102:2231.
49.
MOSCICKI AB, et al. (2006). “Updating the natural history of HPV and
anogenital cancer”. Vaccine. 24: 42–51.
50.
MUNOZ N,
et al. (2003). “Epidemiologic classification of human
papillomavirus types associated with cervical cancer. N Engl J Med. 348: 518–
527.
51.
NAKAGAWA et al. (1999). “CD4 positive and CD8 positive cytotoxic T
Lynphocytes contribute Human Papillomavirus Type 16 E6 and E7
responses”. Clinical and dianostic laboratory immunology. 6(4): 494 – 498.
52.
NELSON, J.H. et al. (2000). "A novel and rapid PCR-based method for
genotyping human papillomaviruses in clinical samples".
J. Clin. Microbiol.
38:688-695.
53.
PINHO AA, et al. (2003). "Prevenção do câncer do útero: um modelo
teórico para analisar o acesso e a utilização do teste de Papanicolaou". Rev
Bras Mater Infant. 3:95-112.
54.
ROITT, IVAN, et al. (2003). “Imunologia”. 6. ed. Barueri: Manole. 481 p.
Titulo original: “Immunology”. ISBN: 85-204-1439-7.
55.
RÓLON, P.A. et al. (2000). "Human papillomavirus infection and invasive
cervical cancer in Paraguay". Int. J. Cancer. 85:486-491.
56.
SANTAGOSTINO A, et al. (1999). “An Italian national multicenter study
for the definition of a reference ranges for normal values of peripheral blood
lymphocyte subsets in healthy adults”. Haematologica, 84:499-504.
57.
SANTIN et al. “Induction of Human Papilomavirus-Specific CD4+ and
CD8+ Lynph by E7 – pulsed autologous Dendritic Cells in Patientes whit
Human Papilomavirus Type 16 and 18 positive Cervical Cancer”.
58.
SATHISH N, et al. (2004). “HPV DNA in plasma of patients with cervical
carcinoma”. J Clin Virol; 31 (3): 204-9.
59.
SATO A, et al. (2010). “Association of RNase L with a Ras GTPase-
activating-like protein IQGAP1 in mediating the apoptosis of a human cancer
cell-line”. FEBS J. 28.
LXV
60.
SATO, S, et al. (2004). “Seeing strangers or announcing danger: galectin
– 3 in two models of innate immunity”. Glycoconj J, 19(7-9): 583-91.
61.
SLOAN, VS, et al. (1995). “Mediation by HLA-DM of dissociation of
peptides from HLA – DR”. Nature, 375(6534): 802-6.
62.
STANLEY MA. (2003). “Genital human papillomavirus infection-current
and prospective therapies”. J Natl Cancer Inst Monogr.31: 117-24.
63.
STANLEY MA. (2009). “Immune responses to human papilloma viruses”.
Indian J Med Res, 130(3):266-76.
64.
STANLEY, M. (2008). “Immunobiology of HPV vaccines”. Gynecol.Oncol.
109, S15-S21.
65.
SULLIVAN, LC, et al. (2006). “A structural perspective on MHC class Ib
molecules in adaptive immunity”. Trends Immunol, 27(9): 413-20.
66.
SWATI PATEL and SHUBHADA CHIPLUNKAR (2009). “Host immune
responses to cervical cancer”. Current Opinion in Obstetrics and Gynecology;
21:54–59.
67.
TABAYOYONG, WB, et al. (2007). “Soluble HLA revisited”. Leuk. Res.,
31(2): 121-125.
68.
TENTI, P. et al. (1999). "Perinatal transmission of human papillomavirus
from gravidas with latent infections". Obstetr. Gynecol. 93:475-479.
69.
TRIMBLE, C.L., et al. (2005). “Active and passive cigarette smoking and
the risk of cervical neoplasia”. Obstet Gynecol, 148(1): 174-81.
70.
VARGAS VRA, et al. (2004). "Prevalência das lesões intra-epiteliais
escamosas em exame citológico numa determinada população de Santo
Ângelo, RS".RBAC. 36:7-11.
71.
VILLA, L.L. (2000). "Biologia Molecular: Conceitos e Princípios Básicos".
In: MARTINS, N.V.; PEREYRA, E.A.G. (Ed.). "Conhecendo o HPV Patologia do
trato-genital inferior Colposcopia e CAF". São Paulo: Frôntis Editorial. cap. 20,
p.137-143.
72.
WANG SS, et al. (2009). “Human papillomavirus cofactors by disease
progression and human papillomavirus types in the study to understand
cervical cancer early endpoints and determinants”. Cancer Epidemiol
Biomarks Prev. 18(1): 113-20.
73.
WATTRE P, et al. (1996). “Apoptosis and human viral”. Ann Biol Clin
(Paris). 54(5):189-97. Review.
LXVI
74.
WOLSCHICK, et al. (2011). “Câncer do colo do útero: tecnologias
emergentes no diagnostico, tratamento e prevenção da doença”. RBAC,
48(2): 123-129.
75.
WRIGHT, T.C. et al. (2000). "HPV DNA testing of self-collected vaginal
samples compared with cytologic screening to detect cervical cancer". JAMA.
76.
NGUYEN HH, et al. (2005). “Immune responses to human papillomavirus
in genital tract of women with cervical cancer”. Gynecol Oncol. 96: 452–461.
77.
Matsumoto K, et al. (2006). “IgG antibodies to HPV16, 52, 58 and 6 L1-
capsids and spontaneous regression of cervical intraepithelial neoplasia”.
Cancer Lett. 231: 309-313.
78.
KONYA
J,
et
al.
(2001).
“Immunity
to
oncogenic
human
papillomaviruses”. Adv Cancer Res. 82: 205–238.
79.
Al-Saleh W, et al. (1998). “Correlation of T-helper secretory differentiation
and types of antigenpresenting cells in squamous intraepithelial lesions of the
uterine cervix”. J Pathol. 184: 283–290.
LXVII
ABSTRACT
Cervical cancer is a problem of great social relevance, since it is the second
most common gynecologic malignancy in the world. The main precursor of
uterine cervix cancer is the infection with human papillomavirus (HPV). HPV
has been given much interest by scientific community because of the
relationship established between its epidemiology and cervical cancer. Despite
the great advances in the biology of HPV, little is known about the immune
response to this virus. The human papillomavirus (HPV) is an epitheliotrophic
DNA
virus,
which
is
associated
to
cervical
carcinogenesis
through
epidemiological and laboratory evidences. HPV infections occur in women all
over the world. There is consensus in the literature about the association of
DNA-HPV with cervical intraepithelial neoplasy and cervical cancer. For this
reason it is of great importance the early detection of this type of infection, so
specific treatment can be performed, allowing healing and preventing the
spread of HPV viral particles. This work is characterizing the immunological
profile of patients with HPV by quantifying lymphocyte (CD4, CD8, NK cells and
NKT cells), and correlating this material to the hybrid capture technique in order
to confirm the HPV infection, hoping to contribute for the early diagnosis of
cervical cancer
Keywords: human papillomavirus, immune profile, hybrid capture
LXVIII
ANEXO
Elsevier Editorial System(tm) for European Journal of Obstetrics & Gynecology and
Reproductive Biology
Manuscript Draft
Manuscript Number:
2
Title: UP-REGULATION OF CD8 (+) CELLS IS ASSOCIATED WITH ONCOGENIC HIGHRISK HPV IN WOMEN WITH LSIL.
Article Type: Research Article
Section/Category: Gynecology and Immunology.
Keywords: Human papillomavirus, LSIL, CD4, CD8, NK.
Corresponding Author: Dr GERALDO BARROSO CAVALCANTI JUNIOR, PhD.
Corresponding Author's Institution: UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
First Author: Daliana Caldas Pessoa da Silva
Order of Authors: Daliana Caldas Pessoa da Silva, Geraldo Barroso Cavalcanti Junior, PhD.
Abstract: Human papillomavirus (HPV) infection is frequent in young women and persistent
infection may lead to cervical cancer. Immune response might be a key element regarding the
progression or regression of human papillomavirus (HPV) infection. Individuals with a
suboptimal immune response may be at increased risk of persistent HPV infection leading to
sequelae of various grades of dysplasias and / or associated malignancy. On the other hand,
different lines of evidence indicate that regression of HPV-induced lesions is the consequence
of the cell-mediated immune response. Object: In this study we performed a cross-sectional
study, in patients with a cytologic diagnosis of low-grade squamous intraepithelial lesion (LSIL),
systematically comparing the quantitative expression of CD4 T and CD8 lymphocytes, CD19,
NK, and NKT cells in patients infected by HPV, stratifying patients according to the presence of
oncogenic low- and high-risk HPV DNA. Study Design: We analyzed 30 patients with LSIL who
underwent HPV genotype detection using hybrid capture. Using flow cytometry, the presence of
T lymphocytes (CD4 and CD8), CD19, NK, and NKT cells were investigated. Results: We found
a strong increase of CD8-positive T lymphocytes among patients with oncogenic high-risk HPV
DNA and a statistically significant decrease in the expression of NK and NKT cells in all groups
of patients analyzed when compared with healthy controls. Furthermore, the quantitative
evaluation of the CD19 was normal in patients exhibiting LSIL and HPV when compared among
the healthy control group. Conclusions: These preliminary data suggest that the strong increase
in CD8 T lymphocytes was related to oncogenic high-risk HPV DNA.
LXIX
Suggested Reviewers:
Steven Witkin PhD
Cornell University
[email protected]
Edmund Baracat PhD
Universidade de São Paulo - USP
[email protected]
Iara Linhares
Universidade de São Paulo - USP
[email protected]
Christiane Piena Soares
Universidade Estadual de São Paulo – UNESP
[email protected]
Carlos Roberto Alves
Fundação Oswaldo Cruz – FIOCRUZ / RJ
LXX
June 07, 2011
Dear Editor,
We would like to submit the original research report UP-REGULATION OF CD8
(+) CELLS IS ASSOCIATED WITH ONCOGENIC HIGH-RISK HPV IN
WOMEN WITH LSIL for your evaluation for publication in EUROPEAN
JOURNAL
OBSTETRICS
AND
GYNECOLOGY
BIOLOGY. The purpose of this research was
AND
REPRODUCTIVE
to perform a cross-sectional
study, in patients with a cytologic diagnosis of low-grade squamous
intraepithelial
lesion
(LSIL),
systematically
comparing
the
quantitative
expression of CD4 T and CD8 lymphocytes, NK cells, and NKT cells in patients
infected by HPV, stratifying patients according to the presence of oncogenic
low- and high-risk HPV DNA.
Thank you for your time,
Correspondence:
Prof. Geraldo Barroso Cavalcanti Júnior, MSc, PhD
Laboratory of Clinical Immunology
Department of Clinical and Toxicological Analysis
Faculty of Pharmacy, 1th floor, Health Sciences Center, Federal University of Rio
Grande do Norte.
Avenue Gustavo Cordeiro de Farias S/N, CEP: 59010-180
Natal-RN, Brazil / FAX: + 55 (84) 3215-4226
E-mail: [email protected]
ABSTRACT
Human papillomavirus (HPV) infection is frequent in young women while
persistent infection may lead to cervical cancer. Immune response might be a
key element regarding the progression or regression of human papillomavirus
(HPV) infection. Individuals with a suboptimal immune response may be at
LXXI
increased risk of persistent HPV infection leading to sequelae of various grades
of dysplasias and / or associated malignancy. On the other hand, different lines
of evidence indicate that regression of HPV-induced lesions is the consequence
of the cell-mediated immune response. Objective: To compare the quantitative
expression of CD4 T and CD8 lymphocytes, CD19 as well as NK cells and NKT
cells in HPV-infected patients, correlated with the presence of low-risk and
oncogenic HPV DNA.
Study Design: We analyzed 30 healthy women and 30 patients with Low
Squamous Intraepithelial Lesions undergoing HPV genotype detection by hybrid
capture. Using flow cytometry, the presence of T lymphocytes (CD4 and CD8),
CD19, NK, and NKT cells were investigated. The average number of cells in
each group was verified using the Student t-test. A significance level of 5% was
adopted in all the tests carried out. The Graph Pad statistical program was used
to calculate the values.
Results: We found a sharp increase in CD8-positive T lymphocytes among
patients with oncogenic HPV DNA and a statistically significant reduction in the
expression of NK and NKT cells in all groups of patients analyzed when
compared with the healthy control group. Furthermore, the quantitative
evaluation of the CD19 was normal in patients exhibiting LSIL and HPV when
compared with the healthy control group.
Conclusions: These preliminary data suggest a correlation between the
increased number of CD8 T lymphocytes and oncogenic HPV DNA.
Key words: Human papillomavirus, immunology, CD4, CD8, CD19, NK, NKT.
LXXII
3
UP-REGULATION OF CD8 (+) CELLS ASSOCIATED
WITH ONCOGENIC HIGH-RISK HPV IN WOMEN WITH
LOW SQUAMOUS INTRAEPITHELIAL LESIONS
DALIANA CALDAS PESSOA DA SILVA, ANA KATHERINE DA SILVEIRA
GONÇALVES, MSc, PhD., GERALDO BARROSO CAVALCANTI JUNIOR,
MSc, PhD.
UFRN – Universidade Federal do Rio Grande do Norte, Toxicology and Clinical
Analysis and Obstetrics and Gynecology Department, Natal – RN, Brazil.
Correspondence for:
Prof. Dr. Geraldo Barroso Cavalcante Junior
R. Gal. Gustavo Cordeiro de Farias, s/n
Petropolis – ZIP Code:
Natal/RN – Brazil.
Email: [email protected]
TEL: +55(84) 3342- 9797
LXXIII
CONDENSATION
INCREASED CD8 LYMPHOCYTES AND DECREASED NK CELLS AND NKT
CELLS IN PATIENTS WITH CYTOLOGIC DIAGNOSIS OF LOW-GRADE
SQUAMOUS INTRAEPITHELIAL LESION AND HIGH-RISK HPV DNA.
LXXIV
INTRODUCTION
Cervical cancer is the second most common cancer among women,
responsible for 400,000 deaths worldwide (1-3). Human papillomavirus (HPV) is
a common sexually transmitted infection and thus considered to be the most
important etiological factor of nearly all cervical, anogenital, and oral cancers (45).
HPV-induced cervical carcinogenesis is understood as a multistep
process (6–8). The major steps in cervical carcinogenesis include persistent
infection of the metaplastic cervical epithelium with oncogenic HPV infection
followed by clonal progression of the infected epithelium to cervical pre-cancer
or further invasion (6). Although these fundamental steps are well established,
several immunological studies have shed light on the factors that influence each
of these transitions (9-11). As a result, several predisposing factors have been
implicated in enhancing persistence and/or progression (9-11).
The importance of host immune response in the clearance of HPV
infections is established (6–13). Data from the literature demonstrate that the
local and systemic immune responses seem to play an important role in the
progression of cervical intraepithelial neoplasia (CIN) (14). Host defense is a
partnership between innate immunity and adaptive immunity (15, 16). In simple
terms, the innate immune system detects the pathogen, acting as the first line of
defense and activating the appropriate adaptive immune response (17).
Immune response could possibly be a key element regarding the
progression or regression of HPV infection. Individuals with a suboptimal
immune response may be at increased risk of persistent HPV infection leading
to sequelae of various grades of dysplasia and / or associated malignancy (14,
18, 19). Persistent infection with oncogenic HPV is the main cause of cervical
cancer. Polymerase chain reaction (PCR)-based assays show that HPV DNA
exists in approximately 90.7–96.6% patients with cervical cancer and in 13.4–
15.6% of the control women (7).
Studies have demonstrated the importance of HPV persistence with
abnormal cervical cytology and the subsequent occurrence of cervical intraepithelial neoplasia (CIN) (9-11).
LXXV
Most
HPV-associated
CIN
lesions
in
normal
women
regress
spontaneously, but a small number persist and may progress to invasive
cancer. The risk of high-grade CIN was greatest in women who tested positive
for oncogenic HPV, and the cumulative risks increase with high-viral-loads (11).
The genomic instability of HPV-infected epithelial cells distinguishes the
process of cell transformation from a productive viral infection and enhances the
subsequent key steps toward malignancy. In most individuals, HPV-specific
immune response eventually leads to clearance of the virus. Cervical cancers
usually arise in individuals who retain HPV oncogenic expression for years or
decades without effective immune response to resolve their infection (13–21).
Both cellular and humoral immune responses are essential for the
clearance of HPV-associated cervical lesions. On the other hand, different lines
of evidence indicate that regression of HPV-induced lesions is the consequence
of the cell-mediated immune response. HPV oncogenes that are expressed in
these cells are involved in their transformation and immortalization, and are
required for the progression (22).
Although the role of the humoral and cellular immunity in clearing and
controlling the virus remains undisputed, the characteristics of an effective cellmediated immune response are poorly defined. In this study we performed the
cross-sectional study in patients with a cytological diagnosis of low-grade
squamous intraepithelial lesion (LSIL)
by systematically comparing the
immunologic profile of peripheral blood cells by flow cytometry (FC) in both
groups—HPV- and non-HPV-infected women—through the investigation of Tlymphocyte count (CD3 +), B (CD19 +) natural killer cells or NK cells (CD3/CD16-56 +), NKT cells (CD3 + / CD16-56 +) T cell subsets and also the T
helper (CD3 + / CD4 +) and T suppressor cytotoxic cells (CD3 + / CD8 +), and
then the ratio of TCD4/TCD8 cells. HPV-infected patients were stratified
according to the presence of low- and high-risk HPV DNA.
PATIENTS AND METHODS
Patients
The samples from 60 women seen in an outpatient clinic for genital
infections were collected. Of the total samples, 30 were diagnosed as LSIL
LXXVI
cervical cytology specimens and the remaining 30 were defined as healthy
controls without HPV infection. In addition, both groups were submitted to
Hybrid Capture exam to detect or exclude the presence of low- and high-risk
HPV DNA. All women underwent a blood count study and study of immune
profile for FC.
Women with a degenerative chronic illness, smokers, users of any type
of medication, hormonal contraceptives, and immunosuppressive drugs were
excluded. Also those who were suspect of or had a confirmed pregnancy or
sexuality transmitted disease, including Hepatitis B or HIV infection at the
moment of the gynecological examination, as well as those who made use of
spermicides and antibiotics in less than 30 days prior to testing, did not
participate in the research. Women who had sexual relations, those who had
used vaginal douches in the past 24 hours, or were menstruating,were also
excluded. This prospective study was approved by the Institutional Ethics
Committee for Human Research of the Hospital Universitário Onofre Lopes
from Universidade Federal do Rio Grande do Norte (CEP-HUOL/UFRN).
Sample
Thirty patients underwent a pelvic examination and cervical cytology
using the Papanicolaou method. Swab samples were collected for analysis of
HPV DNA by Hybrid Capture methodology and analysis cytomorphology.
Papanicolaou exams from cervical cytomorfological analysis
We evaluated 30 patients who had clinical features of HPV, such as
condyloma acuminata, and confirmed in the analysis the presence of
cytomorphologic criteria characteristic of the virus, koilocytes, binucleation, a
kind of membrane, among other features.
Hybrid Capture
Using HPV detection we assessed Hybrid Capture in patients with a
cytologic diagnosis of low-grade squamous intraepithelial lesion (LSIL).
Residual samples from 30 LSIL-diagnosed cervical cytology specimens were
evaluated by high-low risk human papillomavirus.
LXXVII
3.1.1.1.1.1.1.1.1
Hematological analysis from patients and control
group
Ten milliliters (mL) of peripheral venous blood was collected in vacutainer
tubes containing EDTA and were mixed immediately. The white blood cell count
(WBC), hemoglobin dosage, and platelet count were accomplished in the
hematological analyzer (Cell-Dyn 3.000). The cytomorphologic analysis was
accomplished in blood films stained by Leishmann. A total of 100 leukocytes
were counted and the result scored in percentage. For conversion to absolute
values, the percentage values were multiplied by the absolute leucocyte count
and divided by 100.
Flow cytometry analysis of immunological profile:
The Immunophenotyping was performed by three-color flow-cytometry
analysis of peripheral blood samples. Surface cell markers were identified by
using
monoclonal
antibodies
(MoAb)
against:
B
and
T
lymphocytes
(CD3FITC/CD19PE/CD45PerCP), T helper and suppressor cytotoxic lymphocytes
(CD4FITC/CD8PE/CD3PerCP),
and
NK
and
NKT
cells
(CD3FITC/CD16-
56PE/CD45PerCP) (41, 42). All MoAb were purchased from Becton-Dickinson
Immunocytochemistry System (San Jose, CA).
One hundred microliliters (100 µL) of total blood cells previously
homogenized were incubated with the 20 µL of MoAb for 30 minutes at room
temperature and in darkness. Then, the suspension was homogenized and
increased to the same 1mL of a 1 in 10 dilution of Becton Dickinson’s FACS
lysing solution in distilled water, having new incubation for more 10 minutes at
room temperature. After this period, the cellular suspension was centrifuged for
5 minutes at 1.500 RPM, the supernatant fluid was discarded, and the cell
pellet was resuspended in cold phosphate buffered saline (PBS, pH 7.2) and
centrifuged again at 1.500 RPM; this last stage was repeated twice. At last, the
cell pellet was resuspended in 1 mL of cold 1% paraformaldehyde in PBS and
the cell suspensions were kept cold in the dark until FC analysis.
A total of 20,000 events per sample were acquired with Fluorescence
Activated Cell Analyzer (FACScan, San Jose, CA, USA) with Cell Quest
software (Cell QuestTM Software, Becton Dickinson Immunocytometry Systems,
LXXVIII
San Jose, CA, USA). Stained samples were analyzed through the forward
scatter (FSC) and side scatter (SSC) gated set around the lymphocyte cell
population, taking into account the parameters Forward Scatter (FSC) in lineal
scale that evaluates the cellular size, Side Scatter (SSC) also in lineal scale,
which evaluates the cellular complexity and cell marker expression in
fluorescence analysis by FL1, FL2, and FL3 in logarithmical scale that detects
green, orange, and red fluorescence, respectively, which represents the
reaction antigen-antibody conjugated Fluorescein Isohtiocyanate (FICT),
Phycoerythrin (PE), and Peridin Chlorophyll Protein (PerCP), respectively.
The results were expressed as percentage of cells in dual markers such
as: Pan T lymphocytes (CD3+/CD19-), B cells (CD3-/CD19+), T helper
lymphocytes (CD3+/CD4+), T suppressor cytotoxic lymphocytes (CD3+/CD8+),
NK cells (CD3-/CD16-56+), and NKT cells (CD3+/CD16-56+). For conversion to
absolute values, the percentage values were multiplied by the absolute
lymphocyte count and divided by 100 (Figures 1 and 2).
Statistical Analyses
Quantitative comparisons of CD4 T cells, CD8 T cells, NK cells, NKT
cells, and B cells between groups were performed using the Mann-Whitney test.
Clinical parameters were evaluated by means of the two-sided Fisher exact test
for 2×2 contingency tables, with the aid of the GraphPad InStat software (San
Diego, CA, USA). Age, reported as arithmetic mean and standard deviation,
was also compared between groups by means of the two-sided Student
unpaired t-test. Correlations were calculated using the Spearman test.
Statistical analyses were performed using the GraphPad Instat 3.05 software,
with p values < 0.05 considered to be significant.
LXXIX
RESULTS
Detection of human papillomavirus in cervical cytology specimens
According to histopathological analyses, 30 (45.4%) patients exhibited LSILdiagnosed cervical cytology specimens and 30 (54.6%) were normal cervical
histology (healthy women group). Using HPV detection we assessed Hybrid
Capture in patients with a cytologic diagnosis of low-grade squamous
intraepithelial lesion (LSIL). Among the cytology specimens that presented
HPV, 08 out of 30 (27%) exhibited high-risk HPV DNA, 16 out of 30 (53%)
exhibited low-risk HPV DNA, and 6 out of 30 (20%) both (Table 1).
Flow cytometry on blood peripheral sample
Based on the immune response to HPV, we investigated possible
associations between HPV and quantitative evaluation of the CD4, CD8, CD19,
CD3, NK, and NKT cell data. Using flow cytometry, in the quantitative
evaluation of the CD4, CD8, CD19, CD3, NK, and NKT cells, we found strong
positive expression of CD8 positive T lymphocytes among the high-risk HPV
DNA patients when compared with patients with low-risk HPV DNA and the
healthy control group (Table 2, Figure 1).
Among the high-risk HPV DNA group, 5 out 8 (62,5%) had increased
expression of CD8-positive T lymphocytes. Inversely, considering only the
patients with low-risk HPV DNA, only 2 out of 16 (12,5%) patients showed an
increase in CD8-positive T lymphocytes when compared with patients exhibiting
high-risk HPV DNA. Furthermore, the quantitative evaluation of CD19 was
normal in patients exhibiting LSIL and HPV when compared with the healthy
control group (Figure 2B).
LXXX
On the other hand, when NK and NKT cells were analyzed in the group
as a whole, there was a decrease in 26 out of 30 patients (86.6%) when
compared with the healthy control group (Figure 3C and Figure 2D).
In relation to the CD8-positive T lymphocytes, the quantitative evaluation
of CD8 had an increased expression in patients exhibiting LSIL and HPV when
compared with the healthy control group (Figure 3F).
LXXXI
DISCUSSION
There is increasing evidence that the immune system plays a decisive
role in determining the outcome of HPV infection. Both cellular and humoral
immune responses are essential for the clearance of HPV-associated cervical
lesions. (23).
The cell-mediated immune responses by HPV-specific cytotoxic T
lymphocytes (CTL) against oncogenic HPV are believed to play a central role in
cervical carcinogenesis. The above-mentioned cells play a valuable function in
the recognition and defense against HPV-specific antigens and malignant cells.
Differential Th cell responses to HPV-16 E7 have been proposed to correlate
with viral clearance or persistence in patients with cervical neoplasia (24). HPV16 E7-specific Th cell responses may develop as a consequence of increased
antigen availability resulting from clearance and/or progression of cervical
lesions (24,25).
In patients with cervical cancer, a complete loss or down regulation of
HLA Class I on tumor cells was observed. These patients presented reduced
E6 and E7 HPV-specific T cell responses. The absence of T cell response can
be attributed to the lack of a sufficient amount of antigen to activate the immune
response or local immune escape strategy adopted by the virus (26, 27).
Certain human viruses are able to develop suitable strategies that can
induce the generation and accumulation of immunosuppressive molecules
contributing to viral escape from immunological response (28).
In HIV-infected patients, CD4+ T-cell apoptosis is mediated by the
cytopathic effect of the virus and the cell surface expression of gp 120-env
protein.
In
addition,
apoptosis-mediated
physiological
depletion
of
T
lymphocytes in the course of viral infection can silence the immune response
and can induce immunodeficiency (29).
This study systematically evaluated the components quantitatively
expressed in T lymphocytes and their subtypes, T helper cells, cytotoxic T
cells, NK cells, and NKT cells, and also evaluated the B lymphocytes of
patients infected and not infected with the HPV virus. We reported a strong
increase in CD8-positive T lymphocytes among patients with oncogenic highrisk HPV DNA in contrast with those with low-risk HPV-DNA. Possibly, the HPV
LXXXII
may overcome immune surveillance, either by downregulating the proliferation
of HPV-specific CTL or by altering the effector compositions of immune cells
against HPV infection.
Similar results were observed in a previous report. Previous studies
have shown that the presence of proapoptotic proteins in virus-infected cells
and in virus-primed T cells shows greater sensitivity for activated lymphocytes
responding to viral infections expressing high levels of Fas ( CD 95) and that
they are susceptible to apoptosis(29.30). Whether or not HPV is implicated in
the magnitude of the proapoptotic protein expression remains to be elucidated;
however, it is possible that HPV may be involved in the modulation of apoptosis,
since it has been reported that certain viruses are able to develop suitable
strategies for modifying apoptosis.
The genital mucosa also has both inductor and effector arms of an
immune response and HPV infection can interfere with the local immune
vigilance mechanisms in both arms (16). The normal uterine cervix is infiltrated
by lymphocytes (CD4+, CD8+, plasma cells), dendritic cells (DCs) and
macrophages (31, 32). There are also intraepithelial lymphocytes (IELs) in the
ectocervix and the transformation zone (TZ), which are mostly CD8+ and less
frequently CD4+ (31, 32). The stroma, on the other hand, comprises
submucosal lymphocytes predominantly of the CD4+ type found just below the
basement membrane (33) or more abundantly inside the TZ. NK cells are
normally not found, but are present in infections.
The lymphocytic infiltrate is composed predominantly of CD4+ T cells in
the cervical stroma below the area of dysplasia and of CD8+ T cells within the
dysplastic epithelium (34). In this study, we reported strong positive expression
of CD8-positive T lymphocytes among patients with oncogenic high-risk HPV
DNA. Systemic immune vigilance determines latency in HPV infections and
their evolution into high-grade lesions (16); cell-mediated immune responses
measured in the periphery are thought to be largely epiphenomenal.
A recent study realized by Alves et al. (2010) showed higher quantities of
CD4 T and CD8 T lymphocytes observed in CIN II/III and carcinoma (35). Also,
another study examined the strong positive expression of CD3-positive T
lymphocytes among CIN III patients (36). Similar results were observed in a
previous report of an immunohistochemical analysis of CD4+ and CD8+ T-cell
LXXXIII
subsets in high-risk human papillomavirus-associated pre-malignant and
malignant lesions of the uterine cervix (26). Immune response might be a key
element regarding the progression or regression of human papillomavirus
(HPV) infection (37). Different lines of evidence indicate that regression of HPVinduced lesions is the consequence of the cell-mediated immune response.
Overall, it remains to be understood why some LSIL patients express CD8 cellmediated immune response, whereas others do not. These findings are
important; however, additional studies are necessary to identify the influence of
HPV infections and their relation to evolution-grade lesions and cell-mediated
immune response.
Our study demonstrates that there is an association between the
absolute counts of NK and NKT cells with the presence of HPV. However, NK
cells are not a homogeneous cell population and several subtypes exist in both
humans and mice (38); further functional cytotoxicity studies would be needed
to evaluate cytotoxicity of NK cells. NKT cells have a constitutively activated
phenotype and are capable of rapidly secreting large amounts of cytokines
(IFN-g, IL-4, IL-17, IL-5, and IL-13) upon activation, which can modulate many
immunological
processes,
including
tumor
immunity,
maintenance
of
immunologic self-tolerance, prevention of autoimmune disorders, and protection
from a variety of pathogens during experimental infections. NKT cells produce
IFNg and IL-2, which activate NK cells and dendritic cells, enhancing antigen
presentation (39,40). Innate immunity is crucial to the anti-microbial host
defense as it helps control infectious agents until a more potent microbespecific, adaptive immune response can be generated. With this finding, we
speculated that decreased peripheral activated NK and NKT cells may play a
detrimental role in regression of human papillomavirus (HPV) infection (39).
In conclusion, further studies are needed to clarify the molecular aspects
of the relationship between immune response and HPV infection, with potential
applications for cervical cancer prediction.
LXXXIV
ACKNOWLEDGEMENTS:
This study was supported by grants from the Coordination of
Improvement of Higher Education Personnel (CAPES) and Foundation for the
Support of Teaching, Research and Support of Rio Grande do Norte
(FAPERN); Hemocentro Dalton Cunha Barbosa (Hemonorte).
LXXXV
REFERENCES
1.
Zur Hausen H. Papillomaviruses in human cancers. Proc Assoc Am
Physicians 1999; 111: 581-7.
2. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ: Cancer
Statistics. CA Cancer J Clin 2008; 58:71-96.
3. Alvarez-Salas LM, Di Paolo JA: Molecular approaches to cervical cancer
therapy. Curr Drug Discov Technol 2007; 4:208-219.
4. Doorbar J. The papillomavirus life cycle. J Clin Virol 2005; 32:7-15.
5. Kondo K. Development of an HPV vaccine--remaining issues and
perspective. Nippon Rinsho 2009; 67:62-68
6. Moscicki AB, Schiffman M, Kjaer S, Villa LL. Updating the natural history of
HPV and anogenital cancer. Vaccine 2006; 24: 42–51.
7. Munoz N, Bosch FX, de Sanjose S et al. Epidemiologic classification of
human papillomavirus types associated with cervical cancer. N Engl J Med
2003; 348: 518–527.
8. Aguilar LV, Lazcano-Ponce E, Vaccarella S et al. Human papillomavirus in
men: comparison of different genital sites. Sex Transm Infect 2006; 82: 31–33.
9. Castle PE, Solomon D, Schiffman M, Wheeler CM for the ALTS Group.
Human papillomavirus type 16 infections and 2-year absolute risk of cervical
precancer in women with equivocal or mild cytologic abnormalities. J Natl
Cancer Inst 2005; 97: 1066–1071.
10. Ho Gyf, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of
cervicovaginal papillomavirus infection in young women. N Engl J Med 1998;
338: 423–428.
11. Woodman CBJ, Collins S, Winter H et al. Natural history of cervical human
papillomavirus infection in young women: a longitudinal cohort study. Lancet
2001; 357: 1831–1836.
12. Walboomers JMM, Jacobs MV, Manos MM et al. Human papillomavirus is a
necessary cause of invasive cervical cancer worldwide. J Pathol 1999; 189: 1213. Doorbar J. Molecular biology of human papillomavirus infection and cervical
cancer. Clin Sci 2006; 110: 525–541.
14. Voss JS, Kipp BR, Campion MB, Sokolova IA, Henry MR, Halling KC,
Clayton AC. -. Assessment of fluorescence in situ hybridization and hybrid
LXXXVI
capture 2 analyses of cervical cytology specimens diagnosed as low grade
squamous intraepithelial lesion for the detection of high grade cervical
intraepithelial neoplasia. Anal Quant Cytol Histol. 2010; 32:121-30.
15. Coleman N, Birley HD, Renton AM, Hanna NF, Ryait BK, Byrne M, et al.
Immunological events in regressing genital warts. Am J Clin Pathol. 1994; 102:
768-74.
16. Stanley MA, Scarpini C, Coleman N. Cell mediated immunity and lower
genital tract neoplasia. RCOG.monograph; 2003.12:266.
17. Garland SM, Smith JS. Human papillomavirus vaccines: current status and
future prospects. Drugs. 2010;18;70:1079-98.
18. Lee BN, Follen M, Rodriquez G et al. Deficiencies in myeloid antigen
presenting cells in women with cervical squamous intraepithelial lesions.
Cancer 2006; 107: 999–1007.
19. Zhou F, Leggatt GR, Frazer IH. Human papillomavirus 16 E7 protein inhibits
interferon-γ-mediated enhancement of keratinocyte antigen processing and Tcell lysis. FEBS J.278(6):955-63, 2011.
20. Snijders PJF, Steenbergen RDM, Heideman DAM, Meijer CJLM. HPV
mediated cervical carcinogenesis: concepts and clinical implications. J Pathol
2006; 208: 152–164.
21. Wallin KL, Wiklund F, Angstrom T et al. Type-specific persistence of human
papillomavirus DNA before the development of invasive cervical cancer. N Engl
JMed 1999; 341: 1633–1638.
22. Zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical
application. Nat Rev Cancer 2002; 2: 342–350.
23. Bor-Ching Sheu, Wen-Chun Chang, Ho-Hsiung Lin, Song-Nan Chow, SuCheng Huang. Immune concept of human papillomaviruses and related
antigens in local cancer milieu of human cervical neoplasia. Journal compilation
Japan Society of Obstetrics and Gynecology 2007; 3: 103-13.
24. De Gruijl TD, Bontkes HJ,Walboomers JMM et al. Differential T helper cell
responses to human papillomavirus type 16, E7 related to viral clearance or
persistence in patients with cervical neoplasia: a longitudinal study. Cancer Res
1998; 58:1700–1706.
LXXXVII
25. Swati Patel and Shubhada Chiplunkar. Host immune responses to cervical
câncer. Current Opinion in Obstetrics and Gynecology 2009; 21:54–59
26. Monnier-Benoit S, Mauny F, Riethmuller D, Guerrini J, Capilina M, Félix S,
et al. Immunohistochemical analysis of CD4+ and CD8+ T-cell subsets in high
risk human papillomavirus–associated pre-malignant and malignant lesions of
uterine cervix. Gynecol Oncol, 2006; 102:22-31.
27. de Boer MA, Jordanova ES, van Poelgeest MI, et al. Circulating human
papillomavirus type 16 specific T-cells are associated with HLA Class I
expression on tumor cells, but not related to the amount of viral oncogene
transcripts. Int J Cancer 2007; 121:2711–2715.
28.
Kanodia S, Fahey LM, Kast WM. Mechanisms used by human
papillomaviruses to escape the host immune response. Curr Cancer Drug
Targets. 2007;7:79-89.
29. Wattre P, Bert V, Hober D. Apoptosis and human viral. Ann Biol Clin (Paris).
1996; 54(5):189-97.
30. Sato A, Naito T, Hiramoto A, Goda K, Omi T, Kitade Y, Sasaki T, Matsuda
A, Fukushima M, Wataya Y, Kim HS. Association of RNase L with a Ras
GTPase-activating-like protein IQGAP1 in mediating the apoptosis of a human
cancer cell-line. FEBS J. 2010; 28.
31. Garcia-Chacon R, Velasco-Ramirez SF, Flores-Romo L, Daneri-Navarro A.
Immunobiology of HPV Infection. Arch Med Res. 2009;40:443-8.
32. Insinga RP, Dasbach EJ, Elbasha EH. Epidemiologic natural history and
clinical management of Human Papillomavirus (HPV) Disease: a critical and
systematic review of the literature in the development of an HPV dynamic
transmission model. BMC Infect Dis. 2009; 29:119.
33. Einstein MH, Schiller JT, Viscidi RP, Strickler HD, Coursaget P, Tan T,
Halsey N, Jenkins D. Clinician's guide to human papillomavirus immunology:
knowns and unknowns. Lancet Infect Dis. 2009;9:347-56
34. Stanley MA. Immune responses to human papilloma viruses. Indian J Med
Res, 2009; 130:266-76.
LXXXVIII
35. Alves DB, Tozetti IA, Gatto FA, Cassandri F, Ferreira AM, Carlos Eurico
Dos Santos F, Falcão GR, Scapulatempo ID, Padovani CT, Abdo MA. CD4 and
CD8 T lymphocytes and NK cells in the stroma of the uterine cervix of women
infected with human papillomavirus. Rev Soc Bras Med Trop 2010;4: 425-9
36. Maluf PJ, Michelin MA, Etchebehere RM, Adad SJ, Murta. EFT lymphocytes
(CD3) may participate in the recurrence of cervical intraepithelial neoplasia
grade III. Arch Gynecol Obstet. 2008; 278:525-30.
37. Karim R, Meyers C, Backendorf C, Ludigs K, Offringa R, van Ommen GJ,
Melief CJ, van der Burg SH, Boer JM. Human papillomavirus deregulates the
response of a cellular network comprising of chemotactic and proinflammatory
genes. PLoS One. 14;6(3):e17848, 2011.
38. Poli A, Michel T, Thérésine M, Andrès E, Hentges F, Zimmer .CD56bright
natural killer (NK) cells: an important NK cell subset. J.Immunology, 126(4):45865, 2009 Review.
39. Carnaud C, Lee D, Donnars O, Park SH, Beavis A, Koezuka Y, Bendelac A:
Cutting edge: Cross-talk between cells of the innate immune system: NKT cells
rapidly activate NK cells. J Immunol 1999, 163:4647-4650.
40. Gigli G, Caielli S, Cutuli D, Falcone M: Innate immunity modulates
autoimmunity: type 1 interferon-beta treatment in multiple sclerosis promotes
growth and function of regulatory invariant natural killer T cells through dendritic
cell maturation. Immunology 2007, 122:309-417.
41. Cavalcanti Júnior, G.B.; Sales, V.F.S. ; CAVALCANTI SILVA, D.G.K et al.
Detection of CD5 in B-cell chronic lymphoproliferative diseases by flow
cytometry: a strong expression in B-cell chronic lymphocytic leukemia. Acta
Cirur Bras,. 20 (S1): 101-107, 2005.
42. Santo Rodrigues, C.A.; Queiroz, M.G.L; SALES, V.F.S. et al. Estudo
comparativo entre técnicas de contagem de subpopulação de células T em
LXXXIX
indivíduos infectados e não infectados com o vírus da imunodeficiência
humana. Rev Bras Anál Clín. 34 (2): 95-101, 2002.
43. Santagostino A., Garbaccio G., Pistorio A. et al. An Italian national
multicenter study for the definition of reference ranges for normal values of
peripheral blood lymphocyte subsets in healthy. Haematologica :499-504, 1999.
XC
Table 01 - Percentage of patients with high-risk HPV and low-risk HPV
Legend: H-HIGH; L-LOW
5
4
HPV Type
7
HPV – H
Patient
6
Number
8
8
10
HPV – L
11
16
13
HPV -HL
14
6
9
%
27.0%
12
15
53.0%
20%
XCI
Table 02 - Clinical and epidemiological parameters of the 30 patients with L SIL stratified
according to age, lesion type, presence of oncogenic low- and high-risk HPV DNA and levels of
CD4 + , CD8+, CD19+, NK and NKT cells in the peripheral blood
Nº
Age
Lesion
Type
HR
HPV
LR
HPV
CD3/
mm³
CD4/
mm³
CD8/
mm³
CD19/
mm³
NK/
mm³
NKT/
mm³
CD4/CD8
01
39
LSIL
NEG
POS
1079
742
280
266
42
0
2,65
02
42
LSIL
NEG
POS
1386
900
594
180
54
0
1,51
03
24
LSIL
POS
NEG
2260
1200
1170
300
60
5,4
1,02
04
30
LSIL
NEG
POS
1234
748
340
170
51
3,0
2,2
05
34
LSIL
POS
POS
700
430
250
100
20
9
1,72
06
29
LSIL
NEG
POS
1835
1248
832
494
130
1,9
1,52
07
31
LSIL
NEG
POS
1122
697
425
153
187
5,1
1,64
08
44
LSIL
POS
POS
1292
798
494
152
152
3,8
1,61
09
38
LSIL
POS
NEG
1630
672
912
271
72
1,2
0,73
10
38
LSIL
NEG
POS
1216
738
432
160
48
3,2
1,7
11
29
LSIL
POS
NEG
1302
630
651
84
84
0,2
0,96
12
48
LSIL
POS
POS
2730
1287
924
330
462
9,9
1,39
13
35
LSIL
NEG
POS
1106
1439
805
429
105
3,7
1,78
14
35
LSIL
POS
POS
2549
1517
1185
574
164
0
1,27
15
32
LSIL
NEG
POS
1857
1350
750
270
30
0
1,8
16
34
LSIL
NEG
POS
875
600
348
120
12
0
2,5
17
30
LSIL
NEG
POS
2160
1242
702
405
81
2,1
1,76
18
34
LSIL
NEG
POS
1770
750
870
600
90
1,5
0,86
19
18
LSIL
POS
NEG
2613
874
1053
663
174
1,2
1,4
20
39
LSIL
NEG
POS
1544
1058
782
230
69
2
1,35
21
35
LSIL
NEG
POS
2264
1320
990
231
99
1
1,33
22
27
LSIL
POS
NEG
2678
1419
1056
396
165
3
1,34
23
34
LSIL
NEG
POS
898
552
240
144
60
6
2,3
24
36
LSIL
POS
NEG
2016
1275
650
250
50
1
1,96
25
43
LSIL
POS
POS
2289
1023
1147
310
93
6,2
0,89
26
40
LSIL
POS
NEG
2040
1290
750
120
510
9
1,72
27
35
LSIL
NEG
POS
4100
2100
1700
650
100
5
1,25
28
35
LSIL
POS
POS
1518
902
616
220
374
6,6
1,46
29
42
LSIL
NEG
POS
1241
782
510
102
85
3,4
1,5
30
35
LSIL
POS
POS
923
650
429
91
52
9,1
1,51
CD3/
mm³
700
CD4/
mm³
430
CD8/
mm³
221
CD19/
mm³
126
NK/
mm³
12
NKT/
mm³
CD4/CD8
0
0,73
.
Age
Lesion
Type
HR
HPV
LR
HPV
MIN
18
MAX
49
4100
1559
1641
663
510
9,9
2,65
MED
34,83
1774
1007
729
282
122
4,7
1,55
XCII
Figure 1 - CD4+, CD8+ and NK cell levels in the peripheral blood. CD4+, CD8+, and NK cell levels of
peripheral blood from the patients and healthy controls were determined separately by either surface
staining or intracellular staining of the cells using specific antibodies followed by FACS analysis. Scatter
A and histograms: A representative sample
B from patients with high-risk HPV in a, b, c, d, e, and f:
dot plots
Expressed as median fluorescence intensities (MFI) for different categories of patients
C
D
Figure 2
A - Comparison of the dispersion of CD3+ cells from patients and control CD3+ cells of patients
with HPV
B - Comparison of the dispersion of CD19+ cells from patients and control CD19+ cells of
patients with HPV
C - Comparison of the dispersion of NK cells from patients and control NK cells of patients with
HPV
D - Comparison of the dispersion of NKT cells from patients and control NKT cells of patients
with HPV
XCIII
E
F
G
Figure 3
E - Comparison of the dispersion of CD4+ cells from patients and control CD4+ cells of patients
with HPV
F - Comparison of the dispersion of CD8+ cells from patients and control CD8+ cells of patients
with HPV
G - Comparison of the dispersion of CD4+/CD8+ cells from patients and control CD4+/CD8+
cells of patients with HPV
XCIV