LUXAÇÃO AGUDA DA PATELA
ATUALIZAÇÃO / UPDATE
Luxação aguda da patela
Acute patellar dislocation
ARNALDO JOSÉ HERNANDEZ1, EDIMAR FAVARO2, MARCOS HENRIQUE FERREIRA LARAYA3
RESUMO
ABSTRACT
A luxação aguda da patela é uma experiência dolorosa
que ocorre subitamente, como primeiro episódio, afetando principalmente pacientes jovens. O sucesso do tratamento está diretamente relacionado com o conhecimento
da anatomia e da biomecânica. O objetivo da presente atualização é realizar revisão da literatura atual sobre o assunto,
discutindo as tendências mais modernas no tratamento da
luxação aguda da patela. O ligamento femoropatelar medial é o principal estabilizador estático na prevenção do
deslocamento lateral da patela e a primeira estrutura lesada na sua luxação aguda. Além desse ligamento destaca-se a importância do músculo vasto medial oblíquo na
estabilidade patelar. A junção do ligamento femoropatelar medial com a fáscia profunda do músculo vasto medial oblíquo sugere que a estrutura passiva ligamentar e a
dinâmica muscular possuem ação conjunta. Fatores anatômicos e a presença de fraturas osteocondrais predispõem
a recidivas da luxação. A luxação aguda da patela é considerada como sendo pouco freqüente ou subdiagnosticada.
Mais recentemente, a ressonância magnética veio complementar o estudo radiográfico convencional, auxiliando na
opção terapêutica. Atualmente, o tratamento cirúrgico na
Acute patellar dislocation is a painful experience occurring suddenly as the first episode, affecting mainly young
patients. Treatment success is directly related to the knowledge of anatomy and biomechanics. The aim of this present
update is to review the current literature on the subject, discussing the most up-to-date trends in the treatment of acute
patellar dislocation. The medial patellofemoral ligament is
the main static stabilizer for the prevention of lateral patellar displacement, and it is the first injured structure during
acute dislocation. Along with this ligament, the vastus medialis obliquus muscle is important for patellar stability. The
blending of medial patellofemoral ligament with the deep
fascia of the vastus medialis obliquus muscle suggests a conjoint action through ligament passive structure and muscle
dynamics. Anatomical factors and the presence of osteochondral fractures predispose to dislocation recurrence. Acute
patellar dislocation is considered of low frequency or underdiagnosed. More recently, magnetic resonance imaging
has complemented the conventional radiographic study, assisting in the therapeutic decision. Currently, surgical treatment during acute phase, with repair of injured structures,
started to be considered by many as the best therapeutic op-
1. Chefe do Grupo de Cirurgia do Joelho do Instituto de Ortopedia e Traumatologia do Hospital das Clínicas da Faculdade de Medicina da Universidade de
São Paulo; Doutor pela Faculdade de Medicina da Universidade de São Paulo.
2. Ex-Estagiário do Grupo de Cirurgia do Joelho do Instituto de Ortopedia e
Traumatologia do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo.
3. Ex-Estagiário do Grupo de Cirurgia do Joelho do Instituto de Ortopedia e
Traumatologia do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo; Mestre pela Universidade Federal de São Paulo.
1. Head, Knee Surgery Group, Institute of Orthopedics and Traumatology, Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo,
Brazil.
2. Fellow, Knee Surgery Group, Institute of Orthopedics and Traumatology,
Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo, Brazil.
3. MSc, Fellow, Knee Surgery Group, Institute of Orthopedics and Traumatology, Hospital das Clínicas, Faculdade de Medicina da Universidade de São
Paulo, Brazil.
Endereço para correspondência (Correspondence to): Arnaldo José Hernandez, MD, Rua Barata Ribeiro, 414, cj. 53 – 01308-000 – São Paulo, SP, Brasil. Tel./fax:
(11) 3214-4422; e-mail: [email protected]
Copyright RBO2004
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004
65
A.J. HERNANDEZ, E. FAVARO & M.H.F. LARAYA
fase aguda, com a reparação das estruturas lesadas, passou a ser considerado por muitos como a melhor opção
terapêutica, embora a conduta conservadora clássica ainda tenha respaldo e seus defensores na revisão realizada.
Unitermos – Joelho; patela; luxação
INTRODUÇÃO
As afecções da articulação da patela com o fêmur são, certamente, das que mais trazem frustrações ao ortopedista, tanto pela sua alta prevalência como pelo grande número de casos
insolúveis, principalmente em adolescentes jovens(1). Considerando que nas disfunções femoropatelares se englobam
várias manifestações clínicas, a classificação citada por Gouveia Sobrinho, em 1992, é abrangente e as separa em síndromes dolorosas (hiperpressão) e instabilidades rotulianas, que
são agrupadas em: extensão, flexão e potenciais(2). As instabilidades em flexão, por sua vez, subdividem-se em luxações
recidivantes, habituais e permanentes. Além dessas entidades,
a literatura também relata a luxação aguda da patela, que apresenta fisiopatologia pouco compreendida e tratamento controverso(3).
A luxação aguda da patela é experiência dolorosa que ocorre
subitamente, como primeiro episódio, afetando principalmente
pacientes jovens, sendo a meta do tratamento restaurar a função normal do joelho. O sucesso terapêutico está diretamente
relacionado com o conhecimento da anatomia, da biomecânica, do mecanismo do trauma, da fisiopatologia da lesão, do
exame físico detalhado e total familiaridade com as técnicas
de tratamento conservador e cirúrgico, assim como com os
procedimentos que possam ser usados para restaurar a função
da articulação femoropatelar(4).
O objetivo da presente atualização é realizar revisão da literatura atual sobre o assunto, discutindo as tendências mais
modernas no tratamento da luxação aguda da patela.
ANATOMIA E BIOMECÂNICA
Kaplan, em 1957, foi quem primeiro descreveu o ligamento femoropatelar medial, embora não o tenha denominado
assim(5). A partir do estudo pioneiro de Warren e Marshall, em
1979, que descreveram a anatomia capsuloligamentar medial
do joelho, dividindo-a em três camadas, maior ênfase tem sido
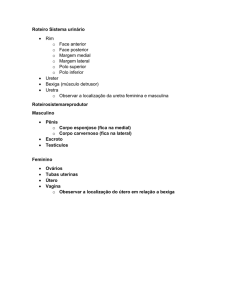
atribuída ao ligamento femoropatelar medial (figura 1)(6,7).
Feller et al, em 1993, confirmaram que o ligamento femoropatelar medial é estrutura distinta da segunda camada medial do joelho, não havendo variações de um lado para o outro
66
tion, although the classic conservative treatment still has
support and its defenders in the accomplished revision.
Key words – Knee; patella; dislocation
INTRODUCTION
Patellofemoral diseases are certainly the most frustrating
to the orthopedic surgeon, due to their high prevalence and
large number of insoluble cases, mainly in young adolescents(1). Considering that patellofemoral diseases include several clinical manifestations, the comprehensive classification
cited by Gouveia Sobrinho in 1992 is based upon subsets in
painful syndromes (hyperpressure) grouped as in extension,
flexion and at risk(21). The patellar flexion instabilities are further subdivided into recurring, usual, and permanent dislocations. Besides those aforementioned entities, the literature
also reports acute patellar dislocation with ill-understood
pathophysiology and controversial treatment(3).
Acute patellar dislocation is a painful experience that occurs suddenly as a first episode, affecting mainly young patients, and the aim of the treatment is to restore normal function of the knee. The success of the treatment is directly related
to the knowledge of anatomy, biomechanics, mechanism of
trauma, pathophysiology of the injury, detailed physical examination, and total familiarity with the surgical and conservative treatment techniques, as well as to the procedures that
can be used to restore patellofemoral joint function(4).
The aim of this present update is to review the current literature on the subject, discussing the most up-to-date trends on
the treatment of acute patellar dislocation.
ANATOMY AND BIOMECHANICS
Kaplan first described in 1957 the medial patellofemoral
ligament, albeit with a different name(5). The medial patellofemoral ligament has gained more importance from Warren
and Marshall’s pioneer study in 1979, which described and
divided the knee medial capsule and ligament anatomy into
three layers (figure 1)(6,7).
Feller et al in 1993 confirmed that the medial patellofemoral ligament is a distinct structure from the second medial
layer of the knee, with no variations from one side to the other
in the same subject(8). From an anatomical study, Tuxoe et al
observed in 2002 that the medial patellofemoral ligament has
a mean width of 1.9 cm and a mean length of 5.3 cm(9). Other
authors reported that the medial patellofemoral ligament is
the main static stabilizer for the prevention of patellar lateral
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004
LUXAÇÃO AGUDA DA PATELA
em um mesmo indivíduo(8). Tuxoe et al, em 2002, por meio
de estudo anatômico, observaram que o ligamento femoropatelar medial tem em média 1,9cm de largura e 5,3cm de comprimento(9). Outros autores relataram que o ligamento femoropatelar medial é o principal estabilizador estático para a
prevenção do deslocamento lateral da patela, contribuindo isoladamente com cerca de 60% da força de restrição deste deslocamento, sendo a primeira estrutura lesada na luxação aguda da patela(10,11).
Além do ligamento femoropatelar medial, a literatura também destaca a importância do músculo vasto medial oblíquo
na estabilidade patelar. Esse músculo foi, inicialmente, descrito de forma distinta por Lieb e Perry em 1968(12) e, posteriormente, confirmado pelo estudo de Reider et al, em 1981,
que observaram que esse músculo apresenta função de estabilização dinâmica na face medial da patela, inserindo-se nessa
em um ângulo entre 55º e 70º em relação à linha média(13).
Mais recentemente, a literatura valorizou a junção do ligamento femoropatelar medial com a fáscia profunda do músculo vasto medial oblíquo, sugerindo que a estrutura passiva
ligamentar e a dinâmica muscular possuem ação conjunta(8).
Em ensaio laboratorial biomecânico a reconstrução do ligamento femoropatelar medial com o tendão do músculo grácil
determina o restabelecimento do alinhamento patelar após o
desvio determinado por sua lesão(14). Em recente revisão sobre o ligamento patelofemoral medial, Amis et al relataram
que suas fibras fundem-se às fibras do vasto medial oblíquo,
formando um complexo que se origina no epicôndilo medial
do fêmur e no tubérculo do adutor. Apesar de delgado, esse
ligamento apresenta resistência à tração de 208N e é o estabilizador medial primário da patela. Sua ação é mais importante
em extensão, quando se encontra sob tensão, o que não se
observa em flexão(15).
Estudando 25 espécimes anatômicos de joelhos de cadáveres humanos, Smirk e Morris avaliaram a anatomia e a isometricidade do ligamento patelofemoral medial objetivando sua
reconstrução. Os pontos ideais de inserção do ligamento são
a borda súpero-medial da patela e logo abaixo e posterior ao
tubérculo do adutor no epicôndilo medial do fêmur(16).
FATORES PREDISPONENTES
Autores acreditam que existam alterações anatômicas que
estão relacionadas com recidivas após a luxação aguda da
patela. Segundo Basset, esses fatores são: patela alta, aumento do ângulo Q, hipermobilidade patelar, torção femoral e tibial, joelho valgo, atrofia do músculo vasto medial oblíquo e
displasia femoral ou patelar; enquanto Cofield e Bryan valoRev Bras Ortop _ Vol. 39, No 3 – Março, 2004
A
B
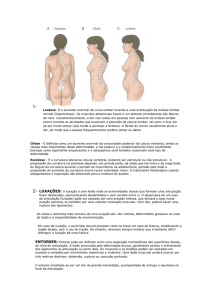
Fig. 1 – Esquema (A) e aspecto
anatômico em cadáver (B) do ligamento femoropatelar medial
Fig. 1 – Schematic (A) and (B) anatomical aspects of medial patellofemoral ligament
displacement, isolatedly contributing with about 60% of the
restrain against that displacement, thus being the first injured
structure during an acute patellar dislocation(10,11).
Besides the medial patellofemoral ligament, literature also
highlights the importance of the vastus medialis obliquus
muscle for patellar stability. This muscle was initially distinctly
described by Lieb and Perry in 1968(12), and later confirmed
by the study by Reider et al in 1981, who reported that this
muscle functions as a dynamic stabilizer at the medial patellar aspect, inserting into the patella at an angle between 55º
and 70º in relation to the midline(13).
More recently, literature has valued the blending of the
medial patellofemoral ligament with the deep fascia from vastus medialis obliquus muscle, suggesting a conjoint action
between the passive ligament structure and muscle dynamics(8).
The medial patellofemoral ligament reconstruction with
gracilis muscle determines the reestablishment of patellar
alignment after deviation caused by injury in a laboratory
biomechanical assay(14). In a recent review on the medial patellofemoral ligament, Amis et al reported that its fibers blend
to the fibers from the vastus medialis obliquus muscle, forming a complex that originates from the femoral medial epicondyle and from the adductor tubercle. Albeit thin, this ligament presents a traction resistance of 208 N, and it is the
primary patellar medial stabilizer. Its action is more important in extension, when it gets under tension, which is not
observed in flexion(15).
67
A.J. HERNANDEZ, E. FAVARO & M.H.F. LARAYA
rizaram a presença de fraturas osteocondrais patelares ou femorais como fatores predisponentes de recidivas, se as mesmas não forem tratadas cirurgicamente(4,17).
Entretanto, Larsen e Lauridsen, em 1982, não encontraram
fatores displásicos responsáveis por recidivas em luxações
agudas da patela e concluíram que tais fatores não podem ser
usados para prever o desenvolvimento de sintomas de instabilidade. Mas sugerem que idade menor que 20 anos está relacionada com maior tendência a recidivas(18).
A importância do fator traumático como causa principal de
luxação aguda da patela é destacada por vários autores(3,19,20).
Ellera Gomes ressalta que, em média, apenas 10% dos pacientes com luxação recidivante da patela citados na literatura foram operados bilateralmente e vários destes fatores predisponentes estão presentes em um único paciente(20).
A frouxidão ligamentar generalizada, embora possa favorecer a ocorrência da luxação aguda ou de suas recidivas, é
considerada por alguns uma característica protetora para a cartilagem articular da patela, diminuindo em duas vezes e meia
a incidência dessas lesões(21).
DIAGNÓSTICO CLÍNICO
A luxação aguda da patela foi considerada por Camanho e
Viegas como sendo de diagnóstico clínico pouco freqüente(22).
Outros autores ponderaram, no entanto, que a condição pode
ser mais freqüente do que se acredita, pois, após a redução
espontânea da luxação, o diagnóstico clínico fica muito difícil(3,23,24,25).
O mecanismo típico da luxação aguda da patela é o trauma
torcional com o fêmur em rotação interna com o pé fixo, ocorrendo contração do músculo quadríceps, tracionando o mecanismo extensor da origem femoral proximal para inserção tibial como a corda de um arco, desse modo criando uma força
lateral de deslocamento da patela. Outro mecanismo possível
é o trauma direto em valgo do joelho ou trauma na borda
medial da patela deslocando-a lateralmente(25).
O paciente tem a sensação de um estalido audível, não conseguindo movimentar a articulação até que ocorra a redução
da luxação de forma espontânea ou, em alguns casos, de forma assistida com extensão do joelho.
Os achados clínicos iniciais da luxação aguda da patela incluem derrame articular, edema, hipermobilidade patelar,
apreensão patelar, dor e equimose ao longo da borda medial
da patela e do tubérculo adutor conhecido como sinal de Bassett(4). Baseados em estudos biomecânicos, Tanner et al sugeriram que o deslocamento lateral e distal da patela, com o
68
Aiming its reconstruction, Smirk and Morris assessed anatomy and isometrics of medial patellar ligament in 25 anatomical knee samples from human corpses. The ideal ligament insertion site is the superomedial border of the patella,
just beneath and behind the adductor tubercle, at the femoral
medial epicondyle(16).
PREDISPOSING FACTORS
Authors believe in existing anatomical changes related to
patellar acute dislocation recurrence. According to Bassett,
these factors include high patella, increase of Q angle, patellar hypermobility, femoral and tibial torsion, valgus knee, atrophy of the vastus medialis obliquus muscle, and femoral or
patellar dysplasia. Conversely, Cofield and Bryan had valued the presence of patellar or femoral osteochondral fractures as recurrence predisposing factors, if not surgically treated(4,17).
However, Larsen and Lauridsen in 1982 did not find any
dysplastic factors responsible for acute patellar dislocation
recurrence, and reached the conclusion that such factors cannot be used to forecast the development of instability symptoms. Nonetheless, they suggest that an age below 20 years is
related to higher recurrence tendency(18).
Many authors highlight the importance of a traumatic factor as the main cause of acute patellar dislocation(3,19,20). Ellera Gomes reports that in average only 10% of patients with
patellar recurrent dislocations mentioned in the literature were
bilaterally operated, and a sole patient presents those several
predisposing factors(20).
Although favoring acute or recurrent dislocation, generalized ligament laxity is considered by some as a protective feature for patellar articular cartilage, with more than twofold
and a half reduction in the incidence of those lesions(21).
CLINICAL DIAGNOSIS
Acute patellar dislocation was considered by Camanho and
Viegas as an infrequent clinical diagnosis(22). However, other
authors claim that such condition may be more frequent than
previously thought, as the clinical diagnosis becomes very
difficult after spontaneous dislocation reduction(3,23,24,25).
The typical acute patellar dislocation mechanism consists
of torsional trauma with the femur positioned in internal rotation with a fixed foot, together with quadriceps muscle contraction, so that the proximal femoral extensor mechanism
acts as a string at the tibial insertion, thus creating a patellar
lateral displacement force. Another possible mechanism is a
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004
LUXAÇÃO AGUDA DA PATELA
joelho a 30º de flexão, seria mais sensível do que a manobra
clássica para a obtenção do sinal da apreensão com o simples
deslocamento lateral direto desse osso(26).
O derrame articular pode ser de grande volume, necessitando eventualmente de esvaziamento por punção. Lesões do
mecanismo extensor (ligamento patelar e tendão do quadríceps) e do ligamento cruzado anterior devem ser incluídas no
diagnóstico diferencial do problema. O exame do joelho contralateral é obrigatório nesses casos.
Freqüentemente, a lesão do ligamento femoropatelar, segundo a maioria dos autores, está localizada próximo ao tubérculo adutor no fêmur(3,24,27,28). Corroborando esse fato, notase que é comum a maior sensibilidade na região do tubérculo
adutor após luxação da patela(4).
EXAMES COMPLEMENTARES
A radiografia é exame complementar importante na determinação de fraturas osteocondrais após o episódio de luxação
aguda da patela; porém, dependendo do tamanho e da localização, pequenos fragmentos podem passar despercebidos, pois
possuem material pouco radiopaco e podem não ser notados.
A radiografia axial da patela deve ser realizada, quando possível, visando melhorar a visualização desses fragmentos(29).
As relações ósseas entre a patela e a tróclea femoral muitas
vezes não traduzem o que ocorre, de fato, dinamicamente(26).
Trikha et al relataram uma série de 10 pacientes com luxação aguda da patela avaliados por meio de ultra-som, exame
clínico e sob anestesia seguidos de reparação artroscópica
das estruturas lesadas; para eles, o ultra-som demonstra adequadamente o estado das partes moles após a luxação aguda
da patela(30).
Outro exame complementar que pode ser utilizado para
avaliação do deslocamento agudo da patela é a ressonância
magnética. Os achados clássicos da luxação aguda da patela
na ressonância magnética são: hemartrose presente em 100%
dos casos, edema da medula óssea envolvendo o aspecto ântero-lateral e lateral do côndilo femoral e o aspecto ínferomedial da patela, além de lesão dos tecidos da face medial do
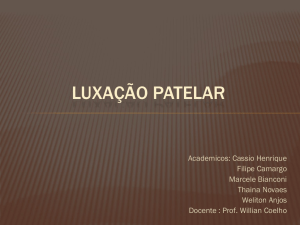
joelho(31) (figura 2).
Kirsch et al, em 1993, publicaram um estudo retrospectivo
de 1.450 achados de imagens de ressonância magnética do
joelho. O deslocamento lateral da patela já reduzido foi diagnosticado através de imagens em 26 casos, sendo que em 73%
destes casos não havia suspeita clínica(31). A ressonância magnética apresenta sensibilidade de 85% e acurácia de 70% para
detectar ruptura do ligamento femoropatelar medial(28).
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004
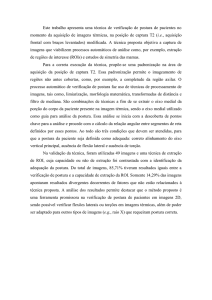
Fig. 2 – Imagem de ressonância magnética com alteração de sinal do ligamento femoropatelar medial (a), da faceta medial da
patela (b) e do côndilo lateral do fêmur (c)
Fig. 2 – Magnetic resonance imaging with signal change at (a) the
medial patellofemoral ligament, (b) medial patellar facet, and (c)
lateral femoral condyle
direct valgus knee blow or trauma at the patellar medial border with a lateral displacement force(25).
The patient feels an audible click, and cannot move the
knee before spontaneous dislocation reduction or, eventually,
with assisted knee extension.
Early clinical findings of acute patellar dislocation include
joint effusion, swelling, patellar hypermobility, patellar apprehension, pain, and ecchymosis along patellar medial border and adductor tubercle, known as Bassett’s sign(4). Based
on biomechanical studies, Tanner et al suggested that patellar lateral and distal displacement, with the knee in 30° of
flexion, would be more sensitive than the classical maneuver
for patellar apprehension sign, which consists of simple, direct patellar lateral displacement(26).
Joint effusion may be large, eventually in need of a joint
tap. Extensor mechanism (patellar ligament and quadriceps
tendon), and anterior cruciate ligament lesions should be included in the differential diagnosis of the problem. The examination of contralateral knee is mandatory in those cases.
According to most authors, the lesion of patellofemoral ligament is often located near the femoral adductor tuber69
A.J. HERNANDEZ, E. FAVARO & M.H.F. LARAYA
TRATAMENTOS
Conservador
O tratamento da luxação aguda da patela é assunto controverso entre os ortopedistas(3,25,32). É interessante notar que a
primeira série de pacientes tratados por método não cirúrgico
relatada na literatura foi a de Cofield e Bryan, em 1977(17), ou
seja, há menos de três décadas, existindo muito poucos estudos prospectivos e randomizados sobre tal assunto(33).
Admite-se que o tratamento não cirúrgico freqüentemente
resulta em recidivas ou persistência dos sintomas de instabilidade(17,18,25,34,35,36). Cofield e Bryan, em 1977, relataram 44%
de recidiva em 48 pacientes com luxação aguda da patela tratados clinicamente(17). Larsen e Lauridsen, em 1982, após avaliar o tratamento não cirúrgico de 79 joelhos com luxação da
patela, concluíram que freqüentemente o tratamento não cirúrgico não é suficiente para restabelecer a estabilidade da
articulação femoropatelar(18). Cash e Hughston, em 1988, em
um trabalho retrospectivo de 30 anos, mencionaram grande incidência de recidivas nos casos tratados conservadoramente(25).
Mäenpää e Letho, em 1997, estudaram 100 pacientes com
luxação aguda da patela tratados de forma conservadora com
seguimento médio de 13 anos e observaram que 63% deles
apresentaram resultados insatisfatórios(35).
Nikku et al, em 1997, publicaram o único artigo randomizado prospectivo que encontramos na literatura, em que, discordando da maior parte dos estudos, concluíram que o tratamento cirúrgico não se mostrou superior ao tratamento
conservador, não o recomendando de rotina(37). Entretanto, o
tempo de seguimento foi de apenas dois anos. Esse fato é de
relevância, pois o risco de recidivas aumenta proporcionalmente com o tempo de seguimento, independente do tipo de
tratamento realizado, sendo menos freqüentes nos casos tratados de forma cirúrgica(33).
No tratamento não cirúrgico, observamos não existir padronização, por parte dos autores, no que se refere ao período
e o tipo de imobilização. Nikku et al, em 1997, utilizaram três
semanas de mobilização, apesar de mencionarem ser favoráveis à mobilização precoce(37), o que também é preconizado
por Hawkins et al(34).
Mäenpää e Letho, em 1997, utilizaram diversos tipos de
órteses (talas, enfaixamentos e imobilizadores plásticos), não
observando diferenças significativas no resultado final. Segundo eles, períodos de imobilização de quatro semanas com
exercícios isométricos ativos e carga parcial, quando tolerados, seguidos de reabilitação de longa duração, costumam oferecer resultados satisfatórios(35).
70
cle(3,24,27,28). Increased tenderness at the adductor tubercle region after patellar dislocation corroborates such fact(4).
COMPLEMENTARY EXAMS
The X-rays are important complementary exams for osteochondral fracture detection after an episode of acute patellar
dislocation, although, depending on the size and location, small
fragments may go undetected and cannot be seen. Patellar
tangential view must be performed whenever possible, in order to improve the viewing of those fragments(29). Many times,
bone relations between patella and femoral trochlea do not
translate what really happens dynamically(26).
Trikha et al reported a series of ten patients with acute patellar dislocations assessed by ultrasound and clinical examination under anesthesia, followed by arthroscopic repair of
injured structures. They reported that ultrasound adequately
shows soft tissue status after acute patellar dislocation(30).
Another complementary exam that may be employed for
acute patellar dislocation is magnetic resonance imaging.
Classical findings of acute patellar dislocation in magnetic
resonance imaging include hemarthrosis, present in 100% of
cases, bone marrow swelling involving anterolateral and lateral aspects of femoral condyle and inferomedial patellar aspect, as well as soft tissue lesion at the knee medial aspect(3)
(figure 2).
Kirsch et al published in 1993 a retrospective study of 1450
findings from knee magnetic resonance imaging. A reduced
patellar lateral dislocation was diagnosed through images in
26 cases, and 73% of those were not clinically suspicious(31).
Magnetic resonance imaging presents 85% of sensitivity and
an accuracy of 70% to detect medial patellofemoral ligament
rupture(28).
TREATMENTS
Conservative
The treatment of acute patellar dislocation poses controversy among orthopedic surgeons(3,25,32). It is interesting to note
that the first series reported in literature of patients treated by
a non-surgical method was published by Cofield and Bryan
in 1977(17), i.e., less than three decades ago, and there are few
randomized, prospective studies on the subject(33).
It is currently thought that non-surgical treatment often results in recurrence or persistence of instability symptoms(17,
18,25,34,35,36). Cofield and Bryan reported, in 1977, 44% of recurrence in 48 patients with conservatively treated acute patellar dislocation(17). Larsen and Lauridsen concluded in 1982
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004
LUXAÇÃO AGUDA DA PATELA
Cirúrgico
Apesar de não ser unanimidade, a literatura sugere que a
abordagem cirúrgica pode ser eficaz no tratamento da luxação aguda da patela, com menor incidência de recidivas(3,24,32).
Ellis, em 1953, durante o encontro da British Orthopaedic
Association, preconizou, pela primeira vez, o reparo da cápsula medial do joelho para a luxação aguda da paleta(17). Posteriormente, Sargent e Teipner relataram que não houve recidivas com esse método em seus casos(38). Lavarde, em 1974,
após tratar cirurgicamente 10 casos de luxação aguda da patela, com excelentes resultados funcionais, preconizou a liberação do retináculo lateral do joelho e sutura em jaquetão do
ligamento femoropatelar medial, com objetivo de prevenir
recidivas e instabilidade(39). Boring e O’Donoghue, em 1978,
não observaram recidivas após tratamento cirúrgico em casos
de luxação aguda da patela, nos quais foi realizado reparo do
retináculo medial do joelho, utilizando técnica cirúrgica descrita por Hauser ou suas modificações(40).
Yamamoto, em 1986, descreveu a reparação artroscópica
da cápsula e do retináculo medial do joelho, associada à liberação do retináculo lateral em 30 casos de luxação aguda da
patela; relatou ter obtido resultados satisfatórios em todos os
casos, exceto em um, no qual houve luxação traumática, e
enfatizou a segurança do método e o benefício causado pela
restauração anatômica dos defeitos provocados pela luxação
da patela(32). Sallay et al, 1996, encontraram, em 15 de 16
pacientes com luxação aguda da patela submetidos à artroscopia seguida de exploração cirúrgica da face medial do joelho, lesão do ligamento femoropatelar medial, que foi suturado e, após seguimento mínimo de dois anos, não observaram
nenhum caso de recidiva(24). Ahmad et al, em uma série de
oito casos de luxação aguda da patela, realizaram liberação
do retináculo lateral do joelho através de artroscopia, seguida
de reparo do ligamento femoropatelar medial e do músculo
vasto medial oblíquo, não relatando nenhum caso de recidiva(3).
Apesar de muitas das técnicas de realinhamento da patela
serem realizadas pelo avanço do vasto medial oblíquo, esse
procedimento ainda permite que a ação desse músculo se exerça preferencialmente no sentido longitudinal e não medial.
Do ponto de vista biomecânico acredita-se que seria mais
apropriada a reinserção do vasto medial oblíquo no tubérculo
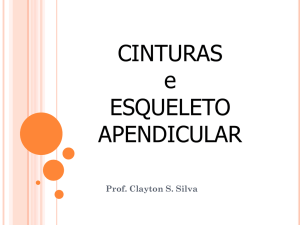
do adutor ou distalmente no tendão do adutor magno, restabelecendo o componente medial da estabilização(15) (figura
3). A ressonância magnética pode auxiliar no diagnóstico e
decisão do local de escolha. Além da reparação, a reconstruRev Bras Ortop _ Vol. 39, No 3 – Março, 2004
that non-surgical treatment is frequently not enough to recover patellofemoral joint stability(18). In 1988, Cash and Hughston in 30-year retrospective study had mentioned a high incidence of recurrence in conservatively managed cases(25).
Mäenpää and Letho in 1997 studied 100 patients with acute
patellar dislocation conservatively treated, with in average
13 years of follow-up, and observed that 63% of them presented unsatisfactory outcomes(35).
Nikku et al published in 1997 the only randomized prospective study found in literature, where, as opposite to most
studies, reached the conclusion that surgical treatment did
not present better results than conservative management, thus
not routinely recommending that approach(37). However, a relevant fact was that follow-up consisted of only two years, while
recurrences risk increases in proportion to follow-up time, no
matter the treatment, and they are less frequent in surgically
managed cases(33).
We have observed a lack of standardization from several
authors as the period of time and immobilization type in nonsurgical treatment. Nikku et al in 1997 employed three weeks
of immobilization, despite the claim of being favorable to early
mobilization(37), also advocated by Hawkins et al(34).
Mäenpää and Letho employed in 1997 several kinds of
orthoses (casting, strapping, and plastic braces) and did not
observe significant differences in the final outcome. According to those authors, four-week immobilization periods with
active isometric exercises and partial weight bearing, followed
by long-time rehabilitation, usually afford satisfactory outcomes(35).
Surgical
Although not unanimous, literature suggests that the surgical approach may be effective for the treatment of acute patellar dislocation, with lower incidence of recurrences(3,24,32).
Ellis in 1953 during the British Orthopaedic Association
meeting first advocated knee medial capsule repair for acute
patellar dislocation(17). Later, Sargent and Teipner reported
no recurrences with such method in their series(38). Lavarde in
1974 treated 10 cases of acute patellar dislocation with excellent functional outcomes, advocating knee lateral retinaculum release and medial patellofemoral ligament plication,
aiming to prevent recurrences and patellar lateral instability(39). Boring and O’Donoghue in 1978 did not observe recurrences after surgical treatment of acute patellar dislocations
managed by knee medial retinaculum repair with the technique described by Hauser or its modifications(40).
71
A.J. HERNANDEZ, E. FAVARO & M.H.F. LARAYA
Fig. 3 – Esquema
da rotura do
ligamento
femoropatelar
medial junto
ao tubérculo
do adutor
Fig. 3
Schematic
of medial
patellofemoral
ligament rupture
at the adductor
tubercle site
ção dessa estrutura tem sido cogitada, embora ainda não existam estudos conclusivos nesse sentido(41).
Por outro lado, Hawkins et al, em 1986, relataram que, independente do tratamento, 30 a 50% dos pacientes de sua
série continuaram a ter sintomas de instabilidade e/ou dor
anterior no joelho(34).
COMENTÁRIOS FINAIS
Apesar dos resultados animadores relatados na literatura
com o tratamento cirúrgico, observamos existir diferentes técnicas utilizadas na luxação aguda da patela, porém, com o
conhecimento fisiopatológico atual, nos parece mais lógico
realizar uma abordagem diretamente no local onde as estruturas foram lesadas. De qualquer forma, o tratamento conservador com imobilização por períodos de até quatro semanas e
fortalecimento muscular precoce seguido de reabilitação pro72
Yamamoto in 1986 described arthroscopic knee medial retinaculum and capsule repair associated to lateral retinaculum release in 30 cases of acute patellar dislocation. The author reported satisfactory outcomes in all cases but one, who
had had a traumatic dislocation; he emphasized the safety of
the method and benefits granted by anatomic repair of defects created by patellar dislocation(32). Sallay et al in 1996
found a medial patellofemoral ligament lesion in 15 of 16
patients with acute patellar dislocation submitted to arthroscopy followed by surgical exploration of the knee medial aspect and ligament suture. A minimum follow-up of two years
did not show any recurrence(24). Ahmad et al in a series of
eight cases of acute patellar dislocation performed knee arthroscopic lateral retinaculum release followed by medial
patellofemoral ligament and vastus medialis obliquus muscle
repair, and reported no recalcitrant cases(3).
Although many patellar realignment techniques include
vastus medialis obliquus muscle advancement, such procedure still allows muscle performance longitudinally, but not
medially. Biomechanically, it is considered that vastus medialis obliquus muscle would be appropriately reinserted in the
adductor tubercle, or distally in the tendon of adductor magnus muscle for reestablishing medial stabilization component(15) (figure 3). Magnetic resonance imaging may be diagnostically helpful and aid for site decision. Besides repair, the
structure reconstruction has been mentioned, although there
are no conclusive studies yet(41).
Conversely, Hawkins et al in 1986 reported that no matter
the treatment, 30% to 50% of patients from their series still
presented instability symptoms and/or knee anterior pain(34).
FINAL COMMENTS
Despite encouraging reports in literature with surgical treatment, we observed different techniques employed for acute
patellar dislocation. Based on the currently known pathophysiology, it seems to us more logical to do a direct approach at
the site where structures have been injured. Anyhow, conservative treatment with immobilization up to four weeks and
early muscle strengthening followed by prolonged rehabilitation is also regarded as correct in the literature.
We cannot forget that, no matter the treatment, there are
patients who continued to present instability symptoms and/
or knee anterior pain, showing the need of more experimental
and clinical studies on such complex clinical condition. Due
to the small number of cases presented by most of the authors,
multicentric studies would probably be the more recommended.
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004
LUXAÇÃO AGUDA DA PATELA
longada também é considerado correto pela literatura apresentada.
Não podemos esquecer de que, independente da forma de
tratamento, existem pacientes que continuaram a ter sintomas
de instabilidade e/ou dor anterior no joelho, demonstrando
que são necessários mais estudos experimentais e clínicos
sobre essa complexa condição clínica. Devido ao pequeno
número de casos apresentados pela maioria dos autores, estudos multicêntricos seriam, provavelmente, os mais recomendados.
REFERÊNCIAS / REFERENCES
1. Mainine S.: Tratamento da Luxação e Subluxação Lateral da Patela [Tese].
São Paulo, Brasil: Faculdade de Ciências Médicas da Santa Casa de São
Paulo, 1999.
2. Gouveia Sobrinho J.L.: Displasia troclear: uma nova classificação das patologias femoropatelares. Rev Bras Ortop 27: 190-196, 1992.
3. Ahmad C.S., Stein B.E., Matuz D., Henry J.H.: Immediate surgical repair
of the medial patellar stabilizers for acute patellar dislocation: a review of
eight cases. Am J Sports Med 28: 804-810, 2000.
4. Basset F.H.: “Acute dislocation of the patella, osteochondral fractures, and
injuries to the extensor mechanism of the knee”. In: Burke E.: American
Academy of Orthopedic Surgeons Instructional Course Lectures, St. Louis,
CV Mosby, Inc., p. 40-49, 1976.
5. Kaplan E.B.: Factors responsible for the stability of the knee joint. Bull
Hosp Joint Dis 18: 51-59, 1957.
6. Arendt E.A., Fithian D.C., Cohen E.: Current concepts of lateral patella
dislocation. Clin Sports Med 21: 499-519, 2002.
7. Warren L.F., Marshall J.L.: The supporting structures and layers on the medial side of the knee. An anatomical analysis. J Bone Joint Surg [Am] 61:
56-62, 1979.
8. Feller J.A., Feagin J.A. Jr., Garrett W.E. Jr.: The medial patellofemoral ligament revisited: an anatomical study. Knee Surg Sports Traumatol Arthrosc
1: 184-186, 1993.
9. Tuxoe J.I., Teir M., Winge S., Nilsen P.L.: The medial patello-femoral ligament: a dissection study. Knee Surg Sports Traumatol Arthrosc 10: 138140, 2002.
10. Conlan T., Garth W.P. Jr., Lemons J.E.: Evaluation of the medial soft-tissue
restraints of the extensor mechanism of the knee. J Bone Joint Surg [Am]
75: 682-693, 1993.
11. Desio S.M., Burks R.T., Bachus K.N.: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 26: 59-65, 1998.
12. Lieb F., Perry J.: Quadriceps function. An anatomical and mechanical study
using amputated limbs. J Bone Joint Surg [Am] 50: 1535-1548, 1968.
13. Reider B., Marshall D.V.M., Koslin B., Ring B., Girgis F.G.: The anterior
aspect of the knee joint. J Bone Joint Surg [Am] 63: 351-356, 1981.
14. Sandmeier R.H., Burks R.T., Bachus K.N., Billlings A.: The effect of reconstruction of the medial patello-femoral ligament on patellar tracking.
Am Sports Med 28: 345-349, 2000.
15. Amis A.A., Firer P., Mountney J., Senavongse W., Thomas N.P.: Anatomy
and biomechanics of the media patello-femoral ligament. Knee 10: 215220, 2003.
16. Smirk C., Morris H.: The anatomy and reconstruction of the medial patellofemoral ligament. Knee 10: 221-227, 2003.
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004
17. Cofield R.H., Bryan R.S.: Acute dislocation of the patella: results of conservative treatment. J Trauma 17: 526-531, 1977.
18. Larsen E., Lauridsen F.: Conservative treatment of patellar dislocations: influence of evident factors on the tendency to redislocation and the therapeutic result. Clin Orthop 171: 131-136, 1982.
19. Atkin D.M., Fithian D.C., Marangi K.S., et al: Characteristics of patients
with primary acute lateral patellar dislocation and their recovery within the
first 6 months of injury. Am J Sports Med 28: 472-479, 2000.
20. Ellera Gomes J.L.: “Reconstrução anatômico-funcional do ligamento patelofemoral medial na luxação recidivante da patela”. In: Pardini Junior A.G.,
Souza J.M.G.: Clínica ortopédica: a articulação femoropatelar. Rio de Janeiro, Medsi, v. 3/3, p. 543-547, 2002.
21. Aglietti P., Buzzi I.R., Insall J.M.: “Disorders of the patello-femoral joint”.
In: Insall J.M., Scott W.N.: Surgery of the knee. 3rd ed., Philadelphia, Churchill
Livingstone, 2001.
22. Camanho G.L., Viegas A.C.: Estudo anatômico e artroscópico do ligamento
femoropatelar medial. Acta Ortop Bras 11: 145-149, 2003.
23. Ellis J.S.: Primary dislocation of the patella [abstract]. J Bone Joint Surg
[Br] 36: 145-146, 1954.
24. Sallay P.I., Poogi J., Speer K.P., Garrett W.E.: Acute dislocation of the patella. A correlative pathoanatomic study. Am J Sports Med 24: 52-60, 1996.
25. Cash J.D., Hughston J.C.: Treatment of acute patellar dislocation. Am J
Sports Med 16: 244-249, 1988.
26. Tanner S.M., Garth W.P. Jr., Soileau R., Lemons J.E.: A modified test for
patellar instability: the biomechanical basis. Clin J Sport Med 13: 327-338,
2003.
27. Avikainen V.J., Nikku R.K., Seppanen-Lehmonen T.K.: Adductor magnus
tenodesis for patellar dislocations: technique and preliminary results. Clin
Orthop 297: 12-16, 1993.
28. Sanders T.G., Morrison W.B., Singleton B.A., Miller M.D., Cornum K.G.:
Medial patello-femoral ligament injury following acute transient dislocation of the patella: MR findings with surgical correlation in 14 patients. J
Comput Assist Tomogr 25: 957-962, 2001.
29. Nayak R.K., Bickerstaff D.R.: Acute traumatic patellar dislocations: the importance of skyline views. Injury 26: 347-348, 1995.
30. Trikha S.P., Acton D., O’Reilly M., Curtis M.J., Bell J.: Acute lateral dislocation of the patella: correlation of ultrasound scanning with operative findings. Injury 34: 568-571, 2003.
31. Kirsch M.D., Fitsgeral S.W., Friedman H., et al: Transient lateral patellar
dislocation: diagnoses with MR imaging. AJR 161:109-113, 1993.
73
A.J. HERNANDEZ, E. FAVARO & M.H.F. LARAYA
32. Yamamoto R.K.: Arthroscopic repair of the medial retinaculum and capsule
in acute patellar dislocations. Arthroscopy 2: 125-131, 1986.
33. Harilainem A., Sandelin J.: Prospective long-term results of operative treatment in primary dislocation of the patella. Knee Surg Sports Traumatol Arthrosc 1: 184-186, 1993.
34. Hawkins N.S.R., Bell R.H., Anisette G.: Acute patellar dislocations: the
natural history. Am J Sports Med 14: 117-120, 1986.
35. Mäenpää H., Lehto M.U.K.: Patellar dislocation: the long-term results of
non-operative management in 100 patients. Am J Sports Med 25: 213-217,
1997.
36. McManus F., Rang M., Heslin D.J.: Acute dislocation of the patella in children. The natural history. Clin Orthop 139: 88-91, 1979.
74
37. Nikku R., Nietosvaara Y., Kallio P.E., Aalto K., Michelsson J.E.: Operative
versus closed treatment of primary dislocation of the patella: similar 2-year
results in 125 randomized patients. Acta Orthop Scand 68: 419-423, 1997.
38. Sargent J.R., Teipner W.A.: Medial patellar retinacular repair for acute and
recurrent dislocation of the patella: a preliminary report. J Bone Joint Surg
[Am] 53: 386-387, 1971.
39. Lavard G.: Traitement des luxations traumatiques récents de la rotule. J Chir
107: 499-514, 1974.
40. Boring T.H., O’Doneghue D.H.: Acute patellar dislocation: results of immediate surgical repair. Clin Orthop 136: 182-185, 1978.
41. Davis D.K., Fithian D.C.: Technics of medial retinacular repair and reconstruction. Clin Orthop 402: 38-52, 2002.
Rev Bras Ortop _ Vol. 39, No 3 – Março, 2004